
Long COVID is real, yet nobody seems to be able to provide an accurate measure on its prevalence.
Neither the CDC's current data nor surveys reporting "no Long COVID" seem to provide accurate data on how many people are suffering.

Over the past few months there has been this strange increase in people who have argued that Long COVID doesn’t exist, or that Long COVID is just an attempt to get ahead of vaccine adverse events.
I’ve been steadfast in my criticisms of these remarks, mostly due to the fact that viral infections have always been considered as a possible hypothesis for symptoms of myalgia and chronic fatigue syndrome that plague many individuals.
However, because these symptoms tend to present in women, the medical establishment has overlooked post-viral syndromes for decades, and instead taking the position that these syndromes are a sign of hysteria or mania, especially if they appeared among groups of women.
I’ve described some accounts of doctors leading up to even the 1980s who have made such remarks in my series on Long COVID:

However, I think this article from Bannister, B.A.1 outlines this issue well:

And so, a lack of investigation has led us to the point we are today, where a dearth of information on post-viral syndrome leads us into a novel pandemic where reports of Long COVID arrive in droves, leading to these reports of Long COVID as being synonymous to COVID alone rather than part of a broader role in viral infections and chronic maladies.
But because of this lack information in the literature, the strange response has been that to against the notion that ‘absence of evidence is not evidence of absence’.
That is, because there isn’t much information on post-viral syndrome people have taken this to somehow mean that Long COVID is a farce, relying on data from surveys even though these surveys are highly subjective, heavily biased, and in fact don’t appear to measure Long COVID in some instances.
And yet, these surveys are still used to downplay the actual extent of Long COVID.

So studies haven’t properly captured the actual degree of Long COVID people may be suffering, but has the CDC done a better job?
Outlets have recently reported that a CDC document noted a possible 7% Long COVID rate in the US…based on survey data.

Well, that’s great, because it tells us that even the CDC is relying on survey data to provide any insights into the actual extent of Long COVID in the US, which immediately also tells us that this data cannot be accurate.
The data came from a 2022 survey conducted by the National Center for Health Statistics to measure how many people had Long COVID at the time of the interview.
Unlike other surveys, this one was at least partially done in a person’s home, with over 20,000 surveys collected:
Data from the 2022 National Health Interview Survey Sample Adult interview (n = 27,651) were used for this analysis. The National Health Interview Survey is a nationally representative household survey of the U.S. civilian noninstitutionalized population. It is conducted continuously throughout the year by the National Center for Health Statistics. Interviews are typically conducted in respondents’ homes, but follow-ups to complete interviews may be conducted over the telephone.
On the surface, the results are pretty alarming, suggesting a possible 7% of Americans may have or had Long COVID. Note that this is data based on a 2022 survey, which may not encapsulate people who suffered from Long COVID during the more virulent variants as many of these people were likely infected with some subvariant of Omicron, so it’s likely that Long COVID reports in 2022 may be lower relative to prior years.
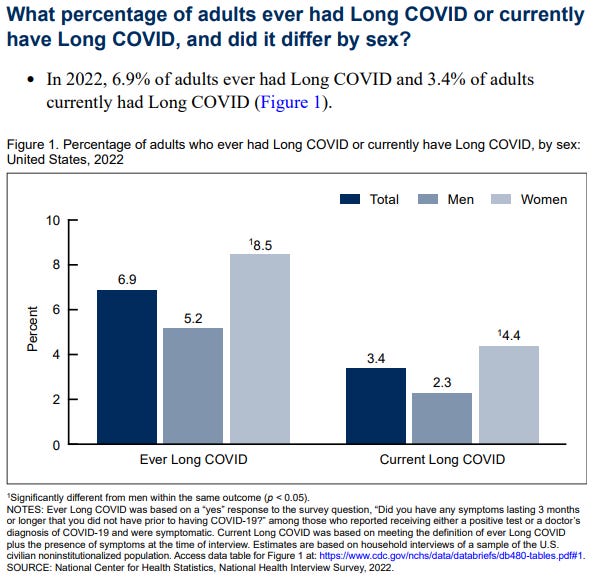
The report makes the following remarks in its summary as well:
In 2022, 6.9% of adults ever had Long COVID and 3.4% of adults currently had Long COVID. For both outcomes, prevalence estimates were higher among women compared with men, adults ages 35–49 compared with other age groups, and adults living in more rural areas compared with those living in large central metropolitan areas. Prevalence estimates were lower among Asian adults compared with other racial and ethnic groups, and adults with family incomes of 400% or more of the federal poverty level compared with those with incomes from 200% through 399% of the federal poverty level.
So is this a better representative number for Long COVID?
Not exactly, as the alleged cases of Long COVID were based on self reports, with the definition of Long COVID used in the survey being the following:
Long COVID: Ever Long COVID was based on a “yes” response to the survey question, “Did you have any symptoms lasting 3 months or longer that you did not have prior to having COVID-19?” among those who reported receiving either a positive test or a doctor’s diagnosis of COVID-19 and were symptomatic. Current Long COVID was based on meeting the definition of ever Long COVID plus the presence of symptoms at the time of interview.
So as long as someone tested positive or had a doctor’s diagnosis, along with persistent symptoms then they met the criteria of Long COVID.
Although a bit of a better definition, it still leaves room for a good deal of subjectivity, relying on people to recall their symptom onset relative to their COVID infection.
All this tells us is that the CDC’s numbers on Long COVID probably aren’t accurate.
However, the higher rate of Long COVID among women seems to be in line with a sex-bias for chronic fatigue syndrome and autoimmune disease, such that these issues seem to occur more frequently among females, so this may be in line with what one would expect when it comes to post-viral syndromes.
But all of this just tells us that we, once again, have an area where we do not have any accurate data, the same as with people suffering adverse events post-vaccination, actual deaths related to COVID, deaths related to the vaccine, etc…
This speaks of a lack in an agreed upon definition of Long COVID as Long COVID itself is a rather nebulous term. Inconsistencies in definition, along with data collection and methodology across studies also means that there is no agreed upon diagnostic criteria which can be used to assess for Long COVID.
Although some studies have suggested some symptoms to look out for when it comes to Long COVID, a recent article published in Nature2 seems to argue that they have found a way of assessing for Long COVID through looking at immune profiles of patients:

Unfortunately, the article is behind a paywall, and other means of accessing don’t seem to have this article yet. As of now, the Abstract seems to make the following remarks (emphasis mine):
Post-acute infection syndromes (PAIS) may develop after acute viral disease1. Infection with SARS-CoV-2 can result in the development of a PAIS known as “Long COVID” (LC). Individuals with LC frequently report unremitting fatigue, post-exertional malaise, and a variety of cognitive and autonomic dysfunctions2–4; however, the biological processes associated with the development and persistence of these symptoms are unclear. Here, 273 individuals with or without LC were enrolled in a cross-sectional study that included multi-dimensional immune phenotyping and unbiased machine learning methods to identify biological features associated with LC. Marked differences were noted in circulating myeloid and lymphocyte populations relative to matched controls, as well as evidence of exaggerated humoral responses directed against SARS-CoV-2 among participants with LC. Further, higher antibody responses directed against non-SARS-CoV-2 viral pathogens were observed among individuals with LC, particularly Epstein-Barr virus. Levels of soluble immune mediators and hormones varied among groups, with cortisol levels being lower among participants with LC. Integration of immune phenotyping data into unbiased machine learning models identified key features most strongly associated with LC status. Collectively, these findings may help guide future studies into the pathobiology of LC and aid in developing relevant biomarkers.
I’ll have to wait for access to this article to actually see what the study entails. In the meantime, it is interesting that these patients appear to show elevated immune response, and even appear to show evidence of possible Epstein-Barr virus reactivation, which appears to be more common than previously realized.

All this to say, even 3 years on there doesn’t appear to be accurate data on Long COVID sufferers, and studies continue to rely on either subjective or nebulous definitions in order to figure out Long COVID patients. The recent Klein, et al. piece may be what’s needed to actually characterize and distinguish Long COVID sufferers from those dealing with other maladies.
In the end, we can argue that Long COVID is real while simultaneously saying the data and evidence coming out is lackluster.
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Bannister B. A. (1988). Post-infectious disease syndrome. Postgraduate medical journal, 64(753), 559–567. https://doi.org/10.1136/pgmj.64.753.559
Klein, J., Wood, J., Jaycox, J. et al. Distinguishing features of Long COVID identified through immune profiling. Nature (2023). https://doi.org/10.1038/s41586-023-06651-y
You can get it on this post which was a year ago also see comments Jean Michel Wendling and Guy Van den Eede
.
Professor Erwin Loh
https://www.linkedin.com/posts/erwinloh_longcovid-blood-fatigue-activity-6965645627112263680-EBrg
⬇️⬇️⬇️⬇️⬇️⬇️
Blood abnormalities found in people with Long Covid
https://www.science.org/content/article/blood-abnormalities-found-people-long-covid
⬇️
Distinguishing features of Long COVID identified through immune profiling
https://www.medrxiv.org/content/10.1101/2022.08.09.22278592v1
How many and what percentage of people suffering “long Covid” symptoms are unvaxxed?