
The Complications of “Long Covid” Part I
An introduction into “Long COVID”, where the name came from, and prior evidence of lingering viral symptoms.

This series is in response to both Subscribers Patty and Peter’s inquiries into Long COVID. Hopefully I will be able to write about some of the topics posted in this prior post. This was meant to be only one post, although it appears this may be turning into an anthology series. I will try to keep this series brief!
COVID has been extensively discussed in everyday discourse. Arguments about the severity of the disease and the harm it may bring about on our society always weighed heavily and were an area for highly contentious debates. When arguing against many of the mandates and lockdowns, proponents of these mandates have always brought up concerns over the long term effects of COVID infection.
At the beginning not much was really known about the long term effects from being infected with COVID. However, months into the pandemic more information came about, and emerging evidence suggested that many people who have fully recovered from a bout with SARS-COV2 continue to have lingering, persistent symptoms. Even as mounting evidence supports the idea of “long-COVID”, there is still so much that is not known about the cause of these persistent symptoms or if there are ways to treat it.
Here, I’ll provide a brief overview to the idea of persistent symptoms after full recovery from the infection. This will include a brief introduction, some of the symptoms, the causes for these symptoms, and if there are any treatment options available. I will also dive, albeit briefly, into the parallels of post-vaccine induced injury and what relationships can be drawn to long-COVID.
Introduction
What is “Long COVID”
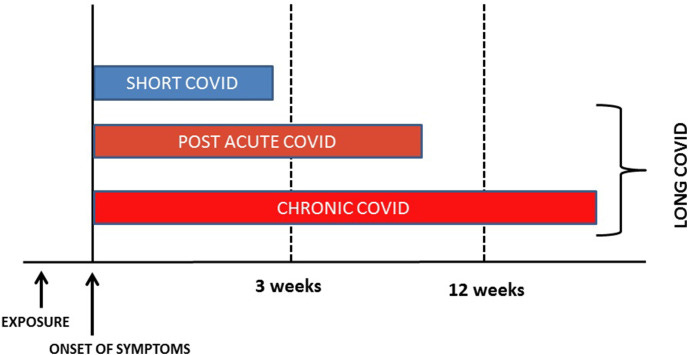
Long COVID is a difficult term to narrow down. In short, it refers to symptoms that someone experiences after there is no evidence of replicating virions after a SARS-COV2 infection. These symptoms are usually referred to as Post-COVID sequelae. The time frame is highly malleable, but it usually refers to symptoms that persist weeks after an infection.
The first reported instances of persistent COVID infections began a few months after COVID began making its way onto the shores of various countries. Initial reports of COVID indicated that many who became infected may experience “mild” illness and would make a full recovery. Although that is true for many, several people, even with mild illness, continued to experience COVID-like symptoms weeks after the infection.
Here’s a few excerpts from Callard, F. & Perego, E. detailing this point:
Emollient descriptions of mild illness did not fit with people's often overwhelming experiences. In March, patients started sharing experiences on social media, drawing attention to possible Covid-related sequelae (e.g. Pope, 2020). In April, newspapers started publishing first-person accounts documenting how challenging recovery from COVID-19 could be (e.g. Lowenstein, 2020). Articles often drew on resources developed within patient-founded groups – e.g. Body Politic COVID-19 Support Group (https://www.wearebodypolitic.com/covid19, founded by Fiona Lowenstein and Sabrina Bleich), and Facebook groups (e.g. https://www.facebook.com/groups/longcovid, founded by Claire Hastie).
On 5 May, the British Medical Journal (BMJ) published Paul Garner's account of suffering seven weeks through a ‘roller coaster of ill health, extreme emotions and utter exhaustion’ (Garner, 2020). Garner, an infectious diseases professor, also appeared in a feature (Harding, 2020b), which, by 10 August, had been read over 1 million times (Harding, 2020a). Garner's account travelled internationally, gathering a wider patient community around what he termed the Covid ‘long tail’. Garner reported patients took his account to medical appointments to provide evidence of the realness of their symptoms (Colbert et al. n. d.). Patient-made evidence in the form of one case study was important when no peer-reviewed articles had yet documented long-lasting symptoms. Non-hospitalized patients were at that point literally beyond the gaze of biomedical research. Patients also challenged ‘mild’: Felicity Callard, then seven weeks into Covid, anatomized the ‘mild’, emphasizing how little was known about whether mild illness was actually mild (Callard, 2020).
The actual assessment of long COVID is very difficult. In many instances, especially at the beginning of the pandemic, there usually was no confirmatory evidence of someone having COVID. Also, because many people were not able to seek medical attention due to lockdowns months may go by before seeing a physician, in which case the symptoms may be attributed to any number of other diseases.
Self-reporting and online surveys have also muddied the waters by not providing any way to properly assess the degree and severity of these symptoms and whether they can be attributed to COVID. This became apparent when JAMA released an observational study which suggested that many symptoms may wrongfully be attributed to COVID, such that people who believed they had COVID (without any evidence) may be more likely to attribute lingering symptoms to COVID. This study doesn’t indicate that long COVID doesn’t exist, but that it may not be as prevalent as was originally believed.
A Video Overview
To provide some more context and general look into long COVID, here is an interview YouTuber and comedian Jimmy Dore had with Dr. Ram “Yo” Yogendra. For some perspective, Jimmy Dore was somewhat hesitant of the lockdown measures and the hiding of possible treatments like Ivermectin by the media. However, when he began feeling symptoms similar to long COVID after receiving his second mRNA vaccine he became openly critical of forced vaccination campaigns. He was not the only one within his immediate vicinity as well to experience symptoms. Both his wife and one of his producers had adverse reactions as well, although Jimmy’s continued to persist months after his second shot. Because of this he began seeking treatment for his post-vaccine symptoms and ended up being referred to Dr. Yo.
Dr. Yo was one of the first proponents of Hydroxychloroquine as a therapeutic agent against SARS-COV2. His main area of work during COVID was actually treating patients with long COVID symptoms. However, when many people began to present with symptoms of long COVID and other adverse reactions after receiving their vaccines, part of his attention went to treating these people as well.
The following discussion is a brief interview in which Dr. Yo provides his perspectives on long COVID including its possible causes, possible treatment options, and a brief discussion about “Medical Oligarchy”, a term somewhat related to the phrase institutional capture that has circulated around. This video will help setup the rest of these posts and the discussions ahead.
The Origins of Long COVID’s Name
The term “Long COVID” actually comes by many different names. Common terms and phrases include “Long Hauler COVID”, “Chronic COVID”, “Post-COVID Syndrome”, etc. For the sake of brevity we will stick with the term “Long COVID”.
The first mainstream use of the term “Long Hauler” came from a piece in The Atlantic by Ed Yong who interviewed several people who had supposedly “mild” COVID that persisted long after the infection was over, leading him towards several support groups for these people struggling with lingering symptoms.

Later, Dr. Elisa Perego (one of the co-authors from the above article) began to use the term “Long COVID” as a truncation of “Long-term COVID illness” and the phrase began to make its way into common vernacular:
Long Covid as a term gained consistency in just a few weeks. #LongCovid was first used by Elisa Perego, from Lombardy (a very hard-hit, early hotspot) on 20 May (Perego, 2020), as a contraction of long-term Covid illness, to summarize her experience of disease as cyclical, progressive, and multiphasic. She used #LongCovid to intervene ontologically in formulations of COVID-19 in peer-reviewed papers – by complicating the ‘biphasic’ disease pathway common in peer-reviewed publications (e.g., Lescure et al., 2020), and pointing to multiple sequelae. In June, #LongCovid became increasingly prominent – complementing other hashtags used by emergent patient collectivities (e.g. #apresJ20 in French, #covidpersistente in Spanish; #MitCoronaLeben in German; #koronaoire in Finnish; #長期微熱組 in Japanese; see also patient websites https://www.apresj20.fr and https://apuakoronaan.fi).
‘Long Covid’ moved from social to print media in late June when a newspaper described how doctor Jake Suett had joined a ‘Long Covid’ support group (Keay, 2020). This group (https://www.longcovid.org) changed its name to ‘Long Covid Support Group’ in response to growing use of #LongCovid – having previously added #Covid1in20 to its name on 23 May in response to the COVID-19 Symptom Study incidence data (personal communication, Claire Hastie, August 19, 2020).
Although many online communities began to sprout up in response to the emergence of Long COVID, the medical community was hesitant to adopt the term or acknowledge its existence. There was no concrete evidence that validated the existence of persistent COVID symptoms and many medical professionals brushed off the notion being purely based on anecdotal evidence. It did not help that, early on in the pandemic, PCR tests were too few to come by, and therefore most people who presented with symptoms of COVID never had their illness confirmed through PCR. Although serology tests may help confirm prior infections, it does not provide an accurate timepoint for symptom onset of the actual disease and whether lingering symptoms afterwards could be attributed to said COVID infection.
However, many physicians began to see that some of their patients still presented with some form of lingering symptoms weeks afterwards. As more and more anecdotal evidence began to spring up it became very difficult to argue that Long COVID did not exist for many people.
Why did it take so long for Long COVID to be acknowledged? Well, it may surprise people to believe that COVID is not the only infection to cause long persistent symptoms, and issues with acknowledgment of post-infectious symptoms may provide some context.
“Post-Viral Syndrome”
When I first started watching videos on COVID in the middle of 2020, I came across some videos on Long COVID which detailed the struggles of understanding it. Even at the time there were many questions as to what Long COVID was or if it even existed. However, what surprised me was the amount of people within the comments section talking about how they were infected with the common cold or seasonal flu many years ago and just never fully recovered afterwards. It revealed that “Long COVID” was not necessarily new to COVID itself, but may be indicative of a larger relationship between us humans and other pathogens.
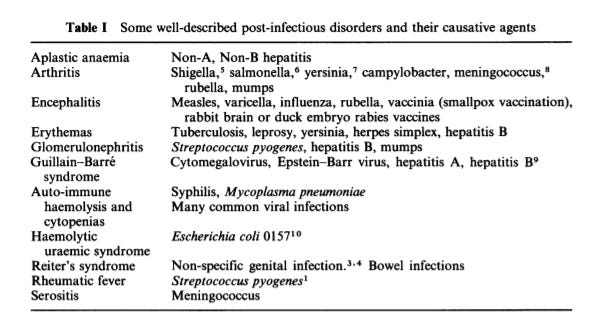
Before Long COVID there was the phrase “Post-Viral Syndrome”, and it refers to a wide array of conditions that tend to emerge or persist after a viral infection. Evidence from many years back have indicated the presence of post-infection symptoms from both viral and bacterial infections within the literature, although we will stick with the term “Post-Viral Infection” here.
However, the idea that people may experience lingering symptoms after an infection was overlooked due to parochial and bigoted thinking at the time.
B.A. Bannister gives an account of this issue in an article from 1988, specifically in regards to post-viral fatigue syndrome:

The word “hysteria” comes about quite often in regards to post-infection symptoms. Neurological/psychological symptoms of fatigue, myalgia, and brain fog appear more frequently in women than in men. Because of possible sexist viewpoints of the time, many of these symptoms were easily brushed off and attributed to hysteria rather than to lingering symptoms from prior infections. This likely led to a misattribution of these symptoms that set back real examinations into post-viral infections. Considering that post-viral symptoms are not just neurological or psychological in pathology, this meant that many within the medical community overlooked a large number of conditions because of backwards thinking and narrow-minded practices.
Even in 1988 a review of post-viral syndrome by M.I. Archer suggested that a “balanced” approach should be taken in regards to post-viral syndrome, suggesting that its manifestation is likely to be attributed to “organic disease” as well as “hysteria”.

Once again, allusions are drawn to the gendered nature of post-viral syndrome as a means of downplaying the symptoms to nothing more than psychological, although the evidence is apparent that manifestations of post-viral syndrome may be sex-linked and that different symptoms may be more prevalent in different sexes.
Fortunately, this idea was still seen as contentious even for the time, as seen in a response letter by J.C. Murdoch:

Nonetheless, the controversies over the realities of post-viral syndrome likely set back any actual investigations into its prevalence and causative agents for many years. It likely explains why not much research has come about in regards to this field of medicine, and also why many people may be oblivious to the fact that SARS-COV2 is not the only virus to leave persistent symptoms after infection.
This points to medicine’s more tortuous past and how outdated modes of thinking has severely altered the course of modern day medicine. Blindspots may have prevented proper science from being conducted under the guise of arrogant, parochial thinking.
Modernity and the Examination of Long COVID
It’s fortunate that the same can’t be said in modern times as it relates to COVID. Ironically, even at a time when massive nationwide lockdowns were occurring many online groups were able to come together to disseminate information. The power of social media most certainly helped, and as advocacy into the nature of Long COVID grew it brought awareness within the mainstream eye to take this information seriously.
Doctors who may have been hesitant to argue the prevalence of Long COVID may have been more inclined to acknowledge its presence due to outcry on social media and anecdotal examinations of their own patients.
Also, modern day techniques for evaluating patients such as the use of MRIs, CT scans, immunological assays and other testing procedures help to validate the notion that lingering symptoms can be traced back to pathophysiological changes after COVID infection. In that sense, modernity provided the proper avenues to both advocate and medically validate the notion of long COVID, something that would not have been possible to the same degree in the 1960s during the “schoolgirl mass hysteria” outbreak.
But even with all of these advancements and nearly two years of studies, long COVID is still difficult to clamp down. Its symptoms are extremely varied and their causes are just as broad.
The next installment will provide a broad overview of post-COVID sequelae and the possible causes of these symptoms.
Ironically, Dore was live-broadcasting a review of John Campbell's youtube review of ivermectin studies as your post went out, confusing his newer viewers (Dore's footprint has exploded thanks to his anti-narrative Ukraine takes).
If you haven't seen it already, Yogendra and Bruce Patterson both discussed the current state of their Long Covid research a few weeks ago on Mobeen's channel. As fast as things are moving, I am pretty sure it's still the most up-to-date glimpse into the Long Covid issue (until the new results Patterson alludes to finally post to preprint) - https://youtu.be/XX30o9GOQiE
Thank you for picking up this topic. I have been working with two people who struggle with this syndrome and was struck especially by the 80’s information and do remember it actually. Ironically, one of these women was given disability status, not because of her extreme physical findings, but for her behavior disorder. Whatever! She is unable to work. She had Covid-19 in 2020 with lingering problems and thought getting the vaccine would help. After each dose her previous problems became more exaggerated. She elected to try ivermectin since none of her physicians had offered anything to help. None had done a physical exam including those at the post Covid clinic even though some of her problems were visible. If I did not have before and after photos, I would be skeptical of reports of her improvements. Within 24hrs she had dramatic improvements and more continued to occur. I knew her to have behavioral issues before this, but doubt they would account for her Raynaud’s hands, Ehlers Danlos-like hypermobility, or urinary bladder retention to mention a few. After a course of IVM, bladder function normalized, her hands are normal color, and her musculoskeletal system was responding to therapy. She powers through trying to get back to normal; others would have given up faced with the same issues.
The second woman saw some relief from her POTS symptoms after a short course of IVM, but her fatigue and cardiac symptoms persist. “I’ve aged 10 years this year.” She continues her EMT teaching position despite it all.
People such as these need physicians who are curious enough to listen, do actual physical exams and address each set of unique problems appropriately. Too many “systems” physicians practice cookie cutter EMR medicine clicking through the drop down boxes. Mental health is impacted by impaired physical health no doubt. Every condition has a psychological component.
Thankfully there are a few physicians who have found diagnostic labs which help direct therapies. Dr Been has YouTube videos addressing these patients. https://youtu.be/XX30o9GOQiE
The frustrating part remains. If people are treated early, hospitalizations and long term consequences (death or disability) could be avoided. We must continue to press for early treatment using safe, effective repurposed drugs to reduce mortality and prevent permanent disability. We must seek out physicians who care to practice the art and science of healing.