
GLP-1 of the heart
The updated indicator for Wegovy raises questions on whether cardioprotective effects of GLP-1 RAs are from weight-loss or related to direct actions on the heart and blood vessels.

In researching GLP-1 RAs there appears to be evidence that GLP-1 doesn’t operate on just on one organ system alone.
So far we have highlighted that:
nervous system (same link as for “the pancreas”)
are all targets of GLP-1, whether through direct agonistic effects of GLP-1 receptor binding or my other passive effects.
With the FDA’s new indicator for Wegovy as a possible therapeutic for those at risk of cardiovascular events, this also raises the question of how exactly these medications may help in ameliorating these heart-related events.
The main assumption that we have made so far suggests that weight-loss itself may be responsible for the better cardiovascular outcomes, as obesity is known to correlate with increased risks of heart attacks, strokes, and other maladies.
It’s quite likely that this remains the main explanation for these benefits, however it’s also worth examining whether there may be other explanations.
Interestingly, it appears that GLP-1 receptors are also expressed in heart tissue as well as on the endothelium of blood vessels.
In some part this isn’t too far-fetched of an assumption as glucagon appears to have effects on the heart itself, so it’s likely that other incretin hormones may also impact the cardiovascular system as well. Indeed, in recent years investigation has led to detection of GLP-1 receptors within the heart (Holst, J. J.1):
It is well established that there are glucagon receptors in the heart and that glucagon has inotropic and chronotropic actions on the heart. Now it turns out that there are also GLP-1 receptors in the heart (28, 33, 283). GLP-1 was also demonstrated to increase cAMP levels in adult rat cardiac myocytes (307), but in that study GLP-1 decreased contraction amplitude as opposed to isoproterenol, which augmented amplitude and, again unlike isoproterenol, GLP-1 did not bring about any intracellular calcium transients, but did cause a modest intracellular acidification. Further evidence for a role for GLP-1 in cardiac function was derived from studies in mice lacking the GLP-1 receptor (87). At the age of 2 mo, these animals had reduced resting heart rate and elevated left ventricular (LV) end-diastolic pressure, compared with wild-type controls. At the age of 5 mo, echocardiography and histology demonstrated increased LV thickness. In addition, there was impaired LV contractility and diastolic function after insulin administration. LV contractility was also reduced after exogenous epinephrine. These data suggest that GLP-1 exerts physiologically important effects on cardiac function.
This is evidenced in a study from Baggio, et al.2, in which it appears that GLP-1R mRNA was detected within all four chambers of human heart tissue.
In that regard, it’s possible that GLP-1 itself may stimulate the heart through interaction with GLP-1 receptors which may lead to modulation of cellular glucose uptake, oxidative stress, and cardiomyocyte-related apoptosis.
However, given the very short half-life of GLP-1 it raises a question if circulating GLP-1 can reach levels high enough to induce an effect on the heart. Some studies in which GLP-1 was implemented required supraphysiologic levels- something that receptor agonists can overcome due to their greater half-life and binding affinity, and may not be possible from regular release of GLP-1. However, it does appear that some metabolites of GLP-1 may also show cardioprotective effects, and so it may not be GLP-1 itself that is beneficial but a system of GLP-1 metabolites that interact to produce cardioprotective benefits.
This cardioprotective effect also extends to those who have had myocardial injury, and thus it appears that GLP-1 and GLP-1 RA may help increase cellular functions post-injury, which may also explain some of the benefits seen in clinical trials such as SUSTAIN-6 and SELECT which recruited people with prior histories of cardiovascular disease.
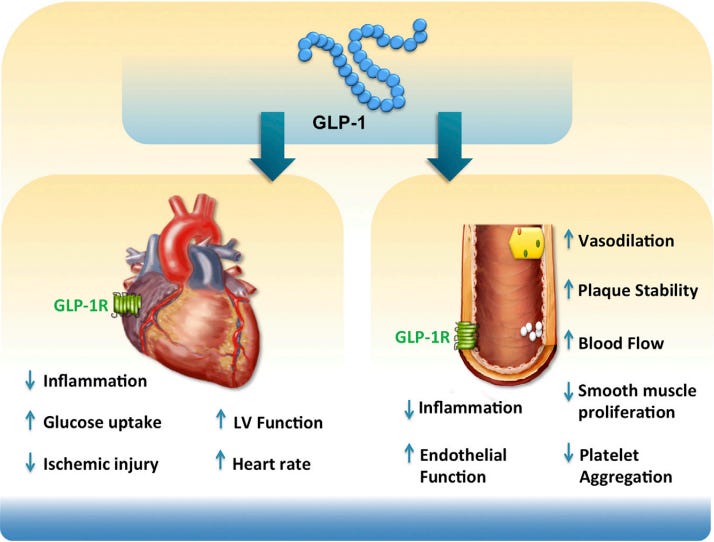
The endothelium has also been found to express GLP-1R, and it’s suggested that binding to these receptors are what may help reduce hypertension and regulate vascular dysfunction.
The main effects appear to be through production of NO as a vasodilator, as well as producing effects similar to the catecholaminergic system(Ferhatbegović, et al.3):
GLP-1 receptor activation induces vasodilation through various pathways. It stimulates production of endothelial nitric oxide (NO), a potent vasodilator, leading to the relaxation of blood vessels and improved coronary blood flow (53, 54). Additionally, GLP-1 agonists may modulate the renin-angiotensin-aldosterone system (RAAS), further influencing vascular tone and blood pressure regulation (54). The vasodilatatory effects of GLP-1 agonists contribute to reduced systemic vascular resistance and, consequently, lower blood pressure.
Although some studies have revealed expression of GLP-1R in endothelial cells the actual cell type isn’t clearly elucidated.
Again, note that the antihypertensive, cardioprotective effects of GLP-1 and GLP-1RA may be derived from effects related to other organs such as effects on kidneys or the nervous system.
Overall, the field of GLP-1 continues to research various ways in which this hormone affects our bodies. More research will hopefully find better explanations and better elucidate the complex biochemical mechanisms that are at play.
What’s important to consider is the balance of mechanistic data along with epidemiological data. That is, even though GLP-1RAs may provide some sort of cardioprotective effect it comes with a large degree of uncertainty in exactly how this effect would occur outside of general benefits related to weight-loss.
Given that these medications have been recognized has having various adverse effects we should raise some concerns on whether these drugs may be associated with possible side effects related to the heart and endothelium.
But it’s also important to ask what may be happening in those who are suffering from cardiovascular disease, and what exactly is happening regarding the GLP-1 that one should be producing. Are people who are diabetic, hypertensive, or at risk of heart failure not producing GLP-1, or has something damaged the cellular responses to GLP-1?
The entire perspective surrounding GLP-1 has been relegated towards the medications. On one hand, the research into GLP-1 RAs has allowed greater insights into what may be happening in the body- consequences of GLP-1 RA administration helps to provide insights into what native GLP-1 may be doing. On the other hand, this has led to a dearth of information regarding GLP-1 itself, meaning that any information that we may come across may relate to the medication in particular and may not be reflective of what actually happens in our bodies.
Greater interest in GLP-1 RAs may thus widen the the gap in information even further. There are many questions that remain to be answered, and quite frankly should be answered before these medications are even further prescribed to even more patients.
This article is intended to be a brief introduction. For those interested in researching the topic further here are some additional articles worth reviewing outside the ones mentioned above:
Solini, et al.4: Incretins and cardiovascular disease: to the heart of type 2 diabetes?
Menghini, et al.5: GLP-1RAs and cardiovascular disease: is the endothelium a relevant platform?
Drucker, D. J.6: The Cardiovascular Biology of Glucagon-like Peptide-1
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Holst J. J. (2007). The physiology of glucagon-like peptide 1. Physiological reviews, 87(4), 1409–1439. https://doi.org/10.1152/physrev.00034.2006
Baggio, L. L., Yusta, B., Mulvihill, E. E., Cao, X., Streutker, C. J., Butany, J., Cappola, T. P., Margulies, K. B., & Drucker, D. J. (2018). GLP-1 Receptor Expression Within the Human Heart. Endocrinology, 159(4), 1570–1584. https://doi.org/10.1210/en.2018-00004
Ferhatbegović, L., Mršić, D., & Macić-Džanković, A. (2023). The benefits of GLP1 receptors in cardiovascular diseases. Frontiers in clinical diabetes and healthcare, 4, 1293926. https://doi.org/10.3389/fcdhc.2023.1293926
Solini, A., Tricò, D., & Del Prato, S. (2023). Incretins and cardiovascular disease: to the heart of type 2 diabetes?. Diabetologia, 66(10), 1820–1831. https://doi.org/10.1007/s00125-023-05973-w
Menghini, R., Casagrande, V., Rizza, S., & Federici, M. (2023). GLP-1RAs and cardiovascular disease: is the endothelium a relevant platform?. Acta diabetologica, 60(11), 1441–1448. https://doi.org/10.1007/s00592-023-02124-w
Drucker D. J. (2016). The Cardiovascular Biology of Glucagon-like Peptide-1. Cell metabolism, 24(1), 15–30. https://doi.org/10.1016/j.cmet.2016.06.009