


FDA updates Ozempic label to include intestinal paralysis as an adverse reaction
Adding to a growing body of safety concerns related to these increasingly popular weight-loss drugs.

On September 22nd the FDA added an additional warning to Ozempic’s label, this time noting ileus, or intestinal paralysis, as a post-marketing adverse reaction, suggesting that these adverse reactions may not have been found or noticed during clinical trials, but have now been reported, especially as these drugs gain in popularity.

This also comes months after reports of stomach paralysis (gastroparesis) in a few individuals, raising growing concerns that these popularized-by-celebrities GLP-1 RA drugs may not be as safe as they are made out to be.
Users of Ozempic-like drugs report stomach paralysis as a side effect

Apologies for readers who may find these reports on Ozempic and other GLP-1 receptor agonists a bit tiring. I personally find that there’s a lot to glean from this Ozempic…
The effect here may be similar to gastroparesis, to the extent that GLP-1 RAs may slow down peristalsis ( contractions/relaxations that move digested food through the gastrointestinal tract), so too may GLP-1 RAs slow down movement of digested material through the intestines, possibly as a mechanism to slow down eating and control insulin spikes (my assumption, at least).
Strangely, this effect was noticed even back in 20171 with the drug Liraglutide (Brand name Victoza) through a study which utilized capsule endoscopy to see the transit time of the endoscope through both the stomach and intestines of Type II Diabetes patients.
The authors noted that, relative to transit time prior to Liraglutide administration, patients provided up to 0.9 mg Liraglutide showed noticeable increases in both gastric and intestinal transit time, suggesting a slowing of bowel movements:
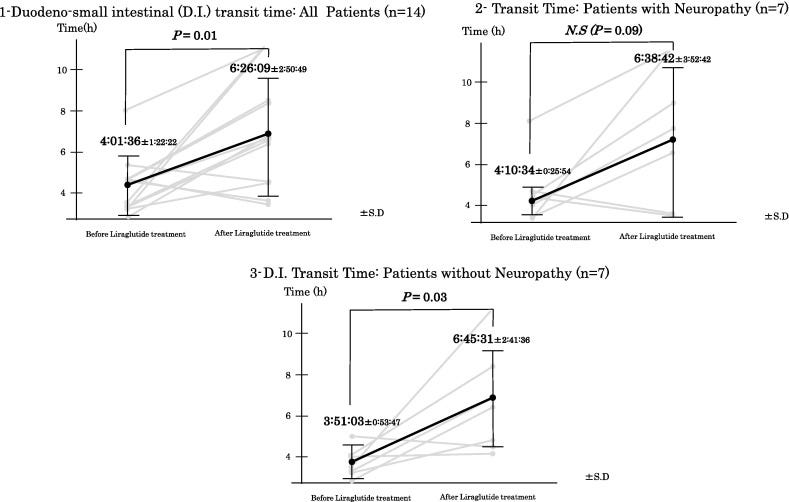
The present study performed capsule endoscopy before and after liraglutide administration and quantitatively evaluated the effects of liraglutide on motility in the gastrointestinal tract.
Liraglutide exhibited gastric-emptying delaying effects, as reported previously. However, the drug also inhibited duodenal and small bowel movements at the same time.
The study was very small, and there were some widely varied results such as a few patients who showed fast transit times following Liraglutide administration, which may be related to diarrhea (this symptom was noted, although considered not severe and not distinctly related to any patient).
That being said, this provides at least some evidence that this slowing down of bowel movements is something that has been documented in prior years. Although it doesn’t explain the phenomena of gastroparesis or ileus in particular2, it does at least suggest a possible risk for these events, especially for those who may be more sensitive to these drugs and therefore may experience stronger responses in reduced bowel movements.
The authors suggest, citing one of their prior studies, that this effect may be related to GLP-1RA activation of the sympathetic nervous system, which may result in a slowing of peristalsis:
Previously, our team reported that the long-acting GLP-1RA liraglutide promotes sympathetic nervous system activity for 24 h [16]. This 24-h promotion of sympathetic nerve activity can activate the greater splanchnic nerve (Th5–9), lesser splanchnic nerve (Th10–11) and sympathetic nerve branch of Auerbach's plexus. Such activation would result in an inhibitory effect of the sympathetic nervous system on intestinal peristalsis, which may extend not only gastric-emptying time, but also duodenal–small bowel-emptying time.
And in 2022 a review of the FDA’s AERS database3 for GLP-1RA-related adverse events noted an unexpected signal for ileus.
Unfortunately, I don’t have access to this study. The Results note the following based on the Abstract (emphasis mine):
A total of 71,515 records involving GLP-1RA monotherapy were submitted to the database, of which 16,350 records were GLP-1RA/IME pairs. Significant disproportionality emerged in five SOCs: 'gastrointestinal disorders' (n = 13,104; lower end of the 95% confidence interval (CI) of the IC [IC025] = 1.34), 'investigations' (n = 6889; IC025 = 0.64), 'metabolism and nutrition disorders' (n = 2943; IC025 = 0.44), 'neoplasms benign/malignant' (n = 1989; IC025 = 0.01), and 'hepatobiliary disorders' (n = 1497; IC025 = 0.38). The most common AEs were pancreatitis, nausea, and weight decrease. Unexpected significant AEs were detected, such as ileus, osteomyelitis, renal cell carcinoma, nephrolithiasis, and drug-induced liver injury.
The actual number of ileus-related events are not provided, but are likely to be low relative to other adverse events.
That being said, the main issue with these adverse events reports is that it notes a severe side effect that many in the public may not be aware about. It certainly undermines the constant announcements that these drugs are safe and effective, and raises a serious question for determining who may be harmed by the use of these drugs, especially as they gain popularity.
It’s worth noting that other GLP-1RAs such as Mounjaro (from Eli Lilly) as well as Wegovy, a higher dosage of Semaglutide than Ozempic, also carry this warning label, and so this actually doesn’t seem out of the ordinary when it comes to this class of drugs, and may be in line with the mechanisms proposed by above.
In a CNN report following the ileus addition to Ozempic’s label, it’s reported that Novo Nordisk, the maker of Ozempic, doubled down on suggesting that Ozempic is safe and effective if used correctly:
“Novo Nordisk stands behind the safety and efficacy of Ozempic® and all of our medicines when used consistent with the product labeling and the approved indications,” the company said.
Strangely, Novo Nordisk also remarks that the slowing down of digestion is something that is commonly known:
“Gastrointestinal (GI) events are well-known side effects of the GLP-1 class,” Novo said in a statement. “For semaglutide, the majority of GI side effects are mild to moderate in severity and of short duration. GLP-1’s are known to cause a delay in gastric emptying, as noted in the label of each of our GLP-1 RA medications. Symptoms of delayed gastric emptying, nausea and vomiting are listed as side effects.”
This fact is a mischaracterization given that most people who are now taking these drugs are unaware of these side effects. This may be due to clinicians who may not be aware of these side effects, or may not even bother to alert patients to their possibility. Patients may also ignore labels on medications, and unless they experience the side effects themselves or see them reported in a mainstream outlet may be none the wiser to these risks.
Sure, the pharmaceutical manufacturers may be aware of these risks, but it certainly doesn’t mean the public are. This is an indication of a clear lack of dissemination of medical information, where recorded knowledge may not be publicly-known knowledge.
As these drugs gain in popularity we may see far more of these adverse reactions. It’s important that people know what they are taking, how they work, and what risks to look out for rather than rely on a nebulous statement of “safe and effective”.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Nakatani, Y., Maeda, M., Matsumura, M., Shimizu, R., Banba, N., Aso, Y., Yasu, T., & Harasawa, H. (2017). Effect of GLP-1 receptor agonist on gastrointestinal tract motility and residue rates as evaluated by capsule endoscopy. Diabetes & metabolism, 43(5), 430–437. https://doi.org/10.1016/j.diabet.2017.05.009
The point of bringing up this study is to make a note that gastroparesis and ileus may be exaggerated responses to GLP-1RAs, to the extent that some individuals may respond so strongly to these drugs that rather than slow down peristalsis, peristalsis just becomes so slow that it becomes detrimental to the individual. It may be that GLP-1RAs may lead to gastrointestinal dysfunction as well, and may explain some persistent paralysis even after stopping these drugs.
Wu, T., Zhang, Y., Shi, Y., Yu, K., Zhao, M., Liu, S., & Zhao, Z. (2022). Safety of Glucagon-Like Peptide-1 Receptor Agonists: A Real-World Study Based on the US FDA Adverse Event Reporting System Database. Clinical drug investigation, 42(11), 965–975. https://doi.org/10.1007/s40261-022-01202-1