
Autopsy reports of myocarditis following mRNA vaccinations
A report of 5 myocarditis-related deaths noted various cellular infiltrates in the heart, which are interestingly similar to that found in the arm of one of the vaccinated deceased.

In the search for answers autopsy reports tend to provide some of the most critical evidence for both the virus as well as vaccine adverse reactions.
Strangely, autopsy findings have been rather limited, even as many have succumbed to the virus and an unknown number have been directly affected by the vaccines.
A while back I remarked that SARS-COV2 did not appear to be a neuroinvasive virus based on autopsy reports which didn’t note direct neuronal damage in those who died from the virus. In contrast, an autopsy report published in December 20221 noted rampant viral infection of various organs and tissues in those who died with/from SARS-COV2. The findings from the December 2022 post are rather interesting, although such reports should be examined with the bystander effect in mind as well as the factor of severe illness and comorbidities (a majority of infections may not lead to widespread viremia unless in the most severe cases).
Altogether, they serve as a reminder of the complexities in assessing the progression of both the viral infection as well as the vaccine-related injuries being recognized. Remember that much of the information so far has been disjointed and lacking various context, and at the end of the day an approach towards consilience is the goal.
To that, various reports of myocarditis following a COVID vaccination including deaths have not produced autopsy findings, which would be critical in figuring out a possible mechanism of heart damage, leaving only limited case reports such as with the individual with Parkinson’s who had 3 vaccine doses eventually died weeks after the 3rd dose due to multifocal necrotizing encephalitis as well as a whole host of other comorbidities.2
Thus, in finding the answer to the myocarditis it’s important to look for autopsy and histopathology reports that provide more insights.
Autopsy findings
A few months ago a report came out detailing findings for 5 individuals who had died with suspected myocarditis related to the COVID vaccines.
This report came from Schwab, et al.3 which looked at German registries for deaths within 20 days of a COVID vaccination.
After excluding for other circumstances and narrowing down the autopsy reports to one hospital (Heidelberg University Hospital) the researchers looked at 5 autopsy reports in particular.
Note that the Dallas criteria was used to consider myocarditis in the deceased, which come with limitations as noted in a previous post.
Autopsy reports also included nasopharyngeal samples used to check for viral infection, with all but one report coming back negative for any form of viral infection. The one individual, Patient 5, appeared to have low levels of human herpes virus 6 (HHV6) which could not be ruled out as being a possible contributing factor in the death of the individual.
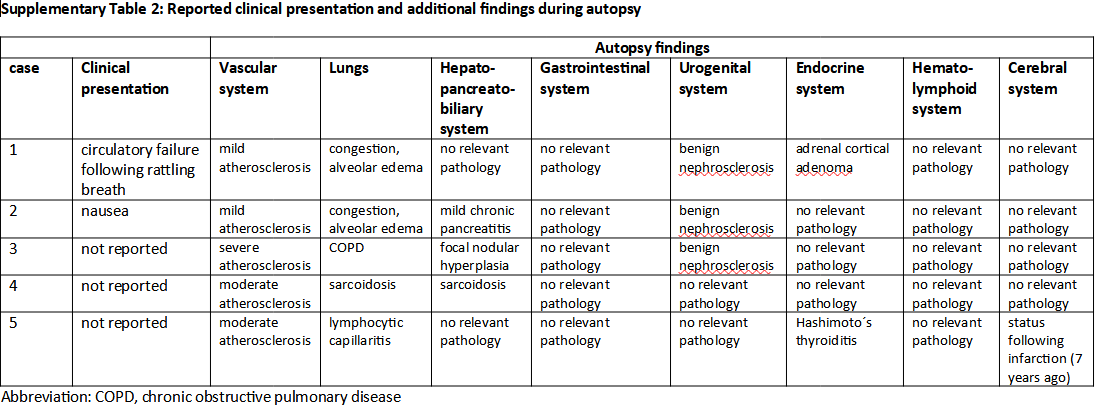
The 5 patients leaned older and had several comorbidities at the time of the autopsy report. The following table shows characteristics of each patient, as well as other clinical presentations and findings during the autopsy of each individual:
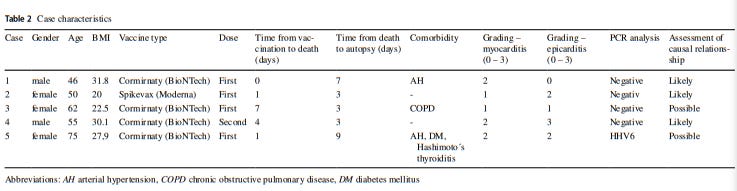
Nearly all 5 deaths occurred within a week of vaccination, with one individual dying within hours after receiving one dose of the BioNTech vaccine (emphasis mine):
Main characteristics of the five cases are presented in Table Table2,2, while further autopsy findings are shown in Supplementary Table 2. Three of the deceased persons were women, two men. Median age at death was 58 years (range 46–75 years). Four persons died after the first vaccine jab, the remaining case after the second dose. All persons died within the first week following vaccination (mean 2.5 days, median 2 days). Clinical findings, blood tests, ECGs or imaging data were not available as deceased persons did not seek medical attention prior to death. Person 1 was found dead 12 h after the vaccination. A witness described a rattling breath shortly before discovering circulatory failure. Person 2 complained about nausea and was found dead soon thereafter. Resuscitation was started immediately but without success, respectively. The other persons were found dead at home without available information about terminal symptoms. According to the available information provided at the time of autopsies, none of the deceased persons had SARS-CoV-2 infection prior to vaccination and nasopharyngeal swabs were negative in all cases.
Histological examinations of the heart noted immune infiltration predominately comprised of lymphocytes. In particular, most of the T-cell subtypes appeared to be of the CD4 subtype relative to CD8:
The histological and immunohistochemical characterization revealed that the inflammatory infiltrate was predominantly composed of lymphocytes. The number of CD3-positive T-cells by far outnumbered the few CD20-positive B-cells detected. In addition, most T-cells belonged to the CD4-positive subset, while only scattered CD8-positive T-cells were seen (Fig. 1, ,2,2, Supplementary Fig. 1/2).

Interesting to this report, and one that I have not seen in other histology reports, was the fact that researchers took samples of one patient’s (Patient 2) deltoid muscle to check for infiltration at the injection site.
Interestingly, and possibly not all-too surprising, the immune infiltration of Patient 2’s deltoid (at the injection site) were similar to that of the hearts in these patients:

Unfortunately, there were no detection of spike or nucleocapsid done in the autopsy report, however one can argue that parallels in histological findings in the deltoid as well as in the heart should be considered sufficient in describing a correlative phenomenon.
In Summary
Based on the autopsy findings, and in accordance with the Dallas criteria and proximity to vaccination the authors suggest that the findings are indicative of vaccine-related myocarditis:
In general, a causal link between myocarditis and anti-SARS-CoV-2 vaccination is supported by several considerations: (A) a close temporal relation to vaccination; all cases were found dead within one week after vaccination, (B) absence of any other significant pre-existing heart disease, especially ischaemic heart disease or cardiomyopathy, (C) negative testing for potential myocarditis-causing infectious agents, (D) presence of a peculiar CD4 predominant T-cell infiltrate, suggesting an immune mediated mechanism. The latter criterion is supported by demonstration of a phenotypically identical T-cell infiltrate at the deltoidal injection site in one of the cases. It has to be emphasized, that a comparable (epi-)myocardial infiltration was neither found in any of the other 20 autopsies performed on bodies found dead within 20 days following an anti-SARS-CoV-2 vaccination nor in the age- and sex-matched cohorts from three independent periods from our autopsy-files.
Based on the autopsy findings and all available data, no other cause of death except (epi-)myocarditis was identified in any of the cases presented here. Hence, myocarditis has to be considered the likely cause of death. From a functional point of view, myocardial damage in our cases is not sufficient to postulate contractile failure as terminal cause of death; thus, arrhythmic failure, either by cardiac arrest or by ventricular fibrillation, has to be assumed as the mechanism leading to the patients’ death. Myocarditis-related acute cardiac arrest due to either asystoly or ventricular fibrillation is a well-established pathomechanism in other causes of acute myocarditis as well [22, 23].
It’s worth noting that the authors remarked that these autopsy findings have not appeared in the 20 years of being associated with the university hospital and appear rather unique:
During the last 20 years of autopsy service at Heidelberg University Hospital we did not observe comparable myocardial inflammatory infiltration. This was validated by histological re-evaluation of age- and sex-matched cohorts from three independent periods, which did not reveal a single case showing a comparable cardiac pathology.
The findings here are critical in elucidating the relationship between myocarditis and the vaccines, although much is still left to be undetermined.
For instance, the lack of spike staining means that we must rely on circumstantial evidence to argue a spike-related effect on the heart.
Also, the ratio of CD4 to CD8-positive T-cell subtypes suggest a possible bias towards antigen recognition/processing relative to cytotoxic cell death. My knowledge on immunology is severely lacking, but it appears that CD4-positive cells are activated by binding to antigen peptides provided by MHC II. This complex focuses more on extracellular antigens rather than intracellular ones, and thus may suggest a response to spike protein debris found within the localized region. In contrast, CD8-positive T-cells binding to antigens presented by MHC I, which focus more on intracellular antigen presentation. That is, an infected cell may present antigen peptides on their surface via MHC I, which makes them a target for cell death as it may suggest that the cell is infected. It’s curious whether the large spike production caused by the vaccines may induce a large degree of scavenging and immune activation. The fact that this bias is seen in both the deltoid and the heart raises questions as to whether the heart is being directly targeted by LNPs, or whether spike proteins that translocate to the heart and become targets in this localized region. However, keep in mind that this bias is relying on qualitative/relative information, and thus infiltration of CD8-positive T-cells may still be considered high.
The researchers raised some remarks with respect to possible intravenous injection of these vaccines, and such a phenomenon can’t be ruled out, although still circumstantial (it would likely be very difficult to discern an intramuscular injection vs an intravenous one if no aspiration was done and recorded prior to injection).
In addition, it’s interesting that all of the autopsy reports note various stages of atherosclerosis, which is a hardening (sclerosis) of blood vessels which may narrow the vessels and reduce blood flow. Atherosclerosis is caused partially by plaque build-up from agents such as cholesterol and cellular debris, and may be a circumstance of aging which can’t be ruled out given the age of some of the individuals reported here. Thus, on one hand we may assume a “spike effect” may be contributing to the atherosclerosis if vascular endothelia are being targeted, or that the results may be both spike and other contributing factors such as lifestyle and aging in these 5 individuals.
The one individual who died within hours of vaccination (Patient 1) was the only person reported to have hypertension, which raises questions as to whether the hypertension may have played some contributing factor via a predisposition for a cardiovascular event.
It’s also important to point out that histology findings are limited to the event actually taking place. For instance, the lack of CD8-positive T-cells, as well as other immunological markers, may be due to the timing of the deaths, in which case the lack of cell types or other findings may be due to the rather short time window between vaccination and death. Figures from the later deaths may provide some additional detail with respect to this short time window and immunological response, although these reports don’t appear in the article. It’s also worth considering that autopsy findings may not correlate to incidences of myocarditis in living individuals who may show a different response.
One additional immunohistochemical report provided was of Patient 4 who died 4 days after a second dose (the only one to have gotten a second dose out of the 5) which noted a lack of CD68-positive macrophages in this man’s myocardium. However, these results are also confounded by the number of vaccine doses, as immunological responses after each dose may differ from prior responses (speculation on my part)4.
Remember that many of the results here don’t provide a purely causative link, and limits in the autopsy reports unfortunately don’t provide a full window into what may have taken place for these individuals.
In Regards to Consilience
Even with the limited amount of information available it’s important to consider what limited information is available.
For instance, one of the first autopsy reports from Gill, et al.5 noted the following with respect to two teenage boys who died within days following their second COVID vaccines:

In contrast to Schwab, et al. there appeared to be a lack of lymphocytic infiltration in these teenagers, instead noting widespread neutrophil infiltration (innate immune system) and damage to contraction bands, more akin to findings seen in takotsubo cardiomyopathy.
Given that these two cases occur in those who are much younger there’s a question as to whether differences in immunological responses may contribute to these differences in findings. In a prior post it was found that some cases of myocarditis in children were associated with full, unbound spike proteins within the blood of these individuals.
This would suggest a possible age-related immune response, in which it’s possible that the predominately innate immune response in children and adolescents may lead to a difference in myocarditis presentation as compared to adults. Unfortunately, the lack of evidence makes it difficult to assess a possibility, and more information should come about to explain possible age-related discrepancies.
When looking at the autopsy provided by Mörz, M. in the individual with Parkinson’s the following was noted with respect to the heart:
Heart: Macroscopic cardiac examination revealed manifestations of acute and chronic cardiovascular insufficiency, including ectasia of the atria and ventricles. Furthermore, left ventricular hypertrophy was noted (wall thickness: 18 mm, heart weight: 410 g, body weight: 60 kg, height: 1.75 m). There was evidence of tissue congestion (presumably due to cardiac insufficiency) in the form of pulmonary edema, cerebral edema, brain congestion, chronic hepatic congestion, renal tissue edema, and pituitary tissue edema. Moreover, there was evidence of shock kidney disorder. Histological examination of the heart revealed mild myocarditis with fine-spotted fibrosis and lympho-histiocytic infiltration (Figure 5). Furthermore, there were chronic arteriosclerotic lesions of varying degrees, which are described in detail under “Vascular system”. In addition to these, there were more acute myocardial and vascular changes in the heart. They consisted of mild signs of myocarditis, characterized by infiltrations with foamy histiocytes and lymphocytes as well as hypereosinophilia and some hypercontraction of cardiomyocytes. Furthermore, mild acute vascular changes were observed in the capillaries and other small blood vessels of the heart. They consisted of mild lympho-histiocytic infiltrates, prominent endothelial swelling and vacuolation, multifocal myocytic degeneration and coagulation necrosis as well as karyopyknosis of single endothelial cells and vascular muscle cells (Figure 5). Occasionally, adhering plasma coagulates/fibrin clots were present on the endothelial surface, indicative of endothelial damage (Figure 5).

Strangely, the results here seem to be a mix of the other two reports, but a strange level of eosinophil infiltration and scattered lymphocytes present. The types of lymphocytes don’t appear to be differentiated, and so what characteristics these lymphocytes contain can’t be determined. Damage to contraction bands are reminiscent of those in the two teenagers as well.
It’s important to remember that this individual received 3 doses of vaccines with the first being an adenoviral vector-based vaccine, being the only individual across these reports to have received that type. His death also occurred weeks after the last dose, and so this time-lapse should be looked at with respect to this time difference.
Also, in contrast to the causes of death provided above this individual appeared to have succumbed to the encephalitis, and so these findings may be related to a less deadly presentation of myocarditis.
Overall, there are plenty of discrepancies between case reports, with limitations in autopsy findings and methodology likely contributing to the heterogeneity in results. At the same time, it’s possible that we shouldn’t assume a consistent pattern in myocarditis reports given individual variability.
Hopefully, those with better insights into immunology can properly parse the results from these autopsies. But for now, it’s clear that data collection and autopsy findings continue to lag behind. Autopsies provide a much clearer window into what may be occurring, and without this information many are left only to speculate as to what is going on.
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Stein, S.R., Ramelli, S.C., Grazioli, A. et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature 612, 758–763 (2022). https://doi.org/10.1038/s41586-022-05542-y
Mörz, M. (2022). A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines, 10(10), 1651. MDPI AG. Retrieved from http://dx.doi.org/10.3390/vaccines10101651
Schwab, C., Domke, L. M., Hartmann, L., Stenzinger, A., Longerich, T., & Schirmacher, P. (2023). Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination. Clinical research in cardiology : official journal of the German Cardiac Society, 112(3), 431–440. https://doi.org/10.1007/s00392-022-02129-5
The following slide noted a lack of macrophages, which again may be due to the timing post-vaccination or due to the number of doses:

James R. Gill, Randy Tashjian, Emily Duncanson; Autopsy Histopathologic Cardiac Findings in 2 Adolescents Following the Second COVID-19 Vaccine Dose. Arch Pathol Lab Med 1 August 2022; 146 (8): 925–929. doi: https://doi.org/10.5858/arpa.2021-0435-SA
Didn't the CDC deliberately avoid doing autopsies and doing other due diligence gathering data on problems with the vaccine?
I've been trying to raise awareness of the fact that there are several high-confidence binding sites for cardiac-related microRNAs in both the Pfizer and Moderna spike sequences. My theory is that the manufacturers added these binding sites to provide a negative feedback mechanism for shutting down spike expression in the heart as microRNAs ramp up due to inflammation. If this is the case, then it is likely that the vaccine manufacturers traded short term risk from acute myocarditis for long term risk due to chronic myocarditis.
https://entropywave.substack.com/p/beware-the-switch-flippers