
The masking issue compounds.
Brief commentary on the recent mask systematic analysis, as well as my personal account of "long masking" and remarks on Long COVID.

Recently several people have pointed to a systematic review which looked at physio-metabolic alterations during mask use. I’ll point to The Naked Emperor as one I recall writing about this post, although many others have taken to commenting about this article as well.
As such, I won’t take to breaking down this review, but rather pointing to some interesting findings, as it adds more criticisms towards mask mandates and the possible health consequences.
A Quick Review
The review1 was published in Frontiers recently, and reviewed over 2,000 articles which included key search terms such as mask grade (eg. N95), symptoms such as hypoxia, carbon dioxide, and many other search terms.

In the end the review included 54 studies, with 14 being randomized control trials (RCTs):
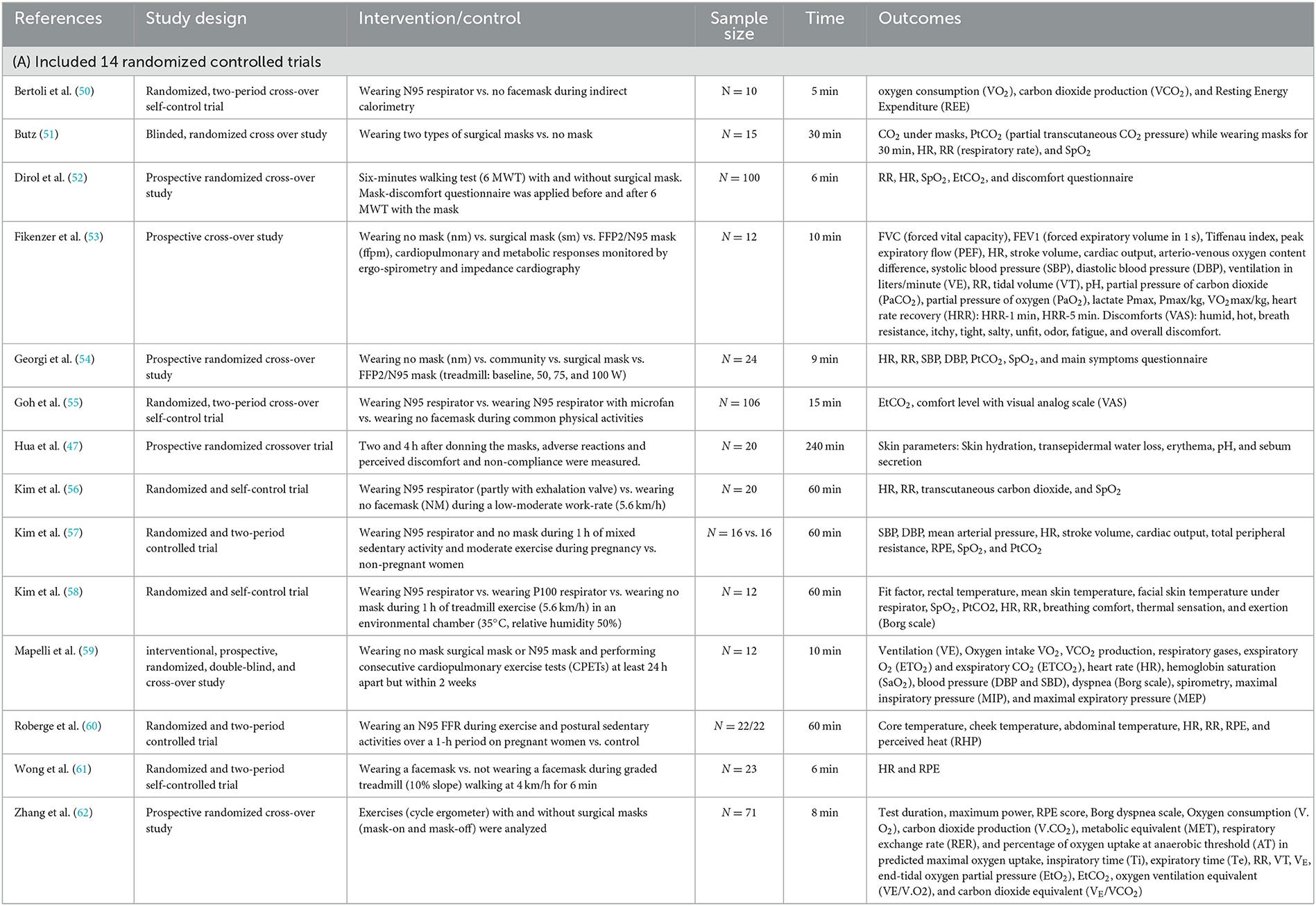
Note that many of these studies measured different outcomes and thus provides a good deal of heterogeneity (as is the case of all reviews and meta-analyses).
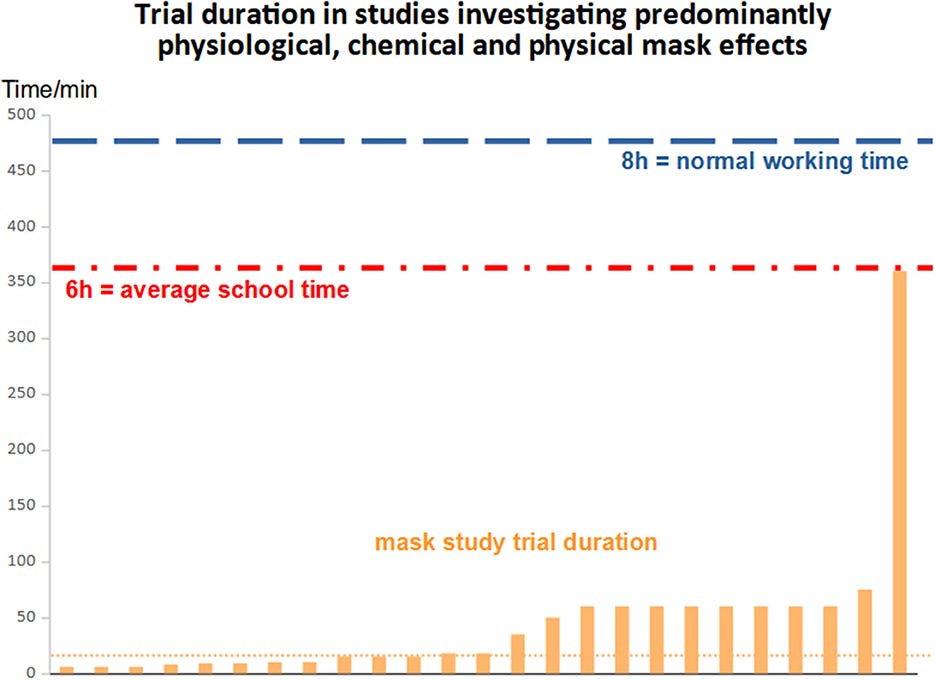
Interestingly, many of these studies looked at the effects of mask wearing for very brief periods of time; the median study looked at mask wearing for 18 minutes, with the longest period of mask-wearing being 360 minutes:
The median experimental time of the studies included in the meta-analyses (mostly controlled trials) on physiological, physical, and chemical face mask effects was 18 min with an interquartile range (IQR) of 50 min (min.: 6 min, max.: 360 min). There was a major variation in mask wearing durations with several outliers leading to a large standard deviation (mean of 45.8 min with a standard deviation of 69.9 min). Therefore, the mean was not an appropriate parameter to characterize this distribution).
The study with the longest experimental duration (360 min, observational) included only 21 healthy participants, which corresponds to 2.2% of the total population studied (n = 934).
To jump ahead, if we consider the scope of health consequences due to masking for short periods (as suggested in the studies reviewed), one has to question the actual effects of daily masking during an entire day of school or work.
Note that none of the studies included in this review actually come close to the period of masking during work or schooling. This suggests that any findings in this review may actually be worse in real-life given that these studies have failed to capture the real effects from longer mask wearing.
Many of the findings are likely to have been symptoms you may have personally experienced, such as increased humidity and temperature, itchiness, and discomfort while wearing a mask.
Many of these symptoms would at least corroborate with the idea of maskne, and the likelihood that the dead space within a mask creates a conducive environment for skin pathobionts to grow and cause issues.
But rather striking is the evidence that suggests reduced gas exchange, with some of the studies noting a reduction in oxygen and an increase in carbon dioxide (emphasis mine):
Our meta-analysis clearly depicts that masks, and especially the N95 masks, significantly restrict O2 uptake and hinder CO2 release. Based on the meta-analytic effect sizes defined by Cohen (102), the effect size for CO2 retention (as per PtCO2, ETCO2, and PaCO2 outcomes) is medium for all mask types and is larger for N95 masks. The effect size for O2 uptake disturbance (as per SpO2 outcome) is relatively smaller but highly significant (p = 0.0004; Figures 2A, B, 9A). Such respiratory gas-exchange discrepancy can be attributed to the constantly increased dead space ventilation volume (14, 60, 65, 103, 104) (i.e., continuous rebreathing from the masks dead space volume) and breathing resistance (14, 53, 59, 66, 67, 83). Continuous CO2 rebreathing causes the right-shift of hemoglobin-O2 saturation curve. Since O2 and CO2 homeostasis influences diverse down-stream metabolic processes, corresponding changes toward clinically concerning directions may lead to unfavorable consequences such as transient hypoxemia and hypercarbia, increased breath humidity, and body temperature along with compromised physiological compensations etc.
As noted above, masking creates an inherent barrier of gas exchange. Although the pores of surgical masks may be rather large relative to the size of gas molecules for oxygen and carbon dioxide, it’s likely the rate of respiration that severely limits the free exchange of gasses between the mask dead space and the outside environment.
That is to say, it’s quite plausible that oxygen/carbon dioxide exchange does not equilibrate before one inhales/exhales again, thus leading to the buildup of carbon dioxide.
But what’s rather interesting is that the build-up of carbon dioxide doesn’t appear to provide a feedback mechanism to compensate for the loss of oxygen. Although carbon dioxide is considered to be a product of respiration levels of oxygen and carbon dioxide must be balanced and tightly regulated within the body.
Strangely, it appears that this wasn’t the case in the studies reviewed, and may point to the artificial mechanism of mask wearing as being a key factor:
Our findings depicted an absence of typical compensatory reactions to transient hypercarbia thereby implying a suppression of a physiological response owing to the unusual conditions of wearing a mask. The reasons behind this phenomenon, i.e., the absence of a rise in the respiratory rate and ventilation, remain unclear. The simultaneous change in the adverse direction (CO2 rise and simultaneous O2 fall with concomitant dead space- and resistance enlargement caused by the mask) may be responsible for this. The drop in SpO2 and the rise in CO2 (PtCO2, ETCO2, and PaCO2) with no major changes in the heart rate in our meta-analysis also transpires to be an unexpected reaction.
Overall, this systematic review rebuts the mainstream notion that masking has no downsides. Rather, there are likely to be long-term ramifications from masking, especially for those who suffer cardiovascular or respiratory issues.
In children there are serious concerns with respect to the development of children and adolescents who may have been deprived of oxygen for several years.
To that, the authors raise the contradictory argument made to mask benefits in their Discussion:
All of these mask-related symptoms contradict a state of wellbeing and health as defined by the WHO. According to the WHO; “health is a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity” (172). Based on our findings, the use of face mask in the hope of maintaining health is unfortunately contradicting the WHO's definition of health. Regarding all the possible side effects of mask and their still unproven efficacy against viral transmission within the general population (5, 10, 173, 174), health seems not to be substantially preserved by wearing face masks.
An Anecdote of Long Masking
Originally, I was not going to consider discussing this post as other people have already.
But I think in some regard the findings of this review are things that many of us have likely lived with.
That is to say, I’m quite sure many of us who were forced to wear masks experienced headaches and tiredness. I even recall several family members describing how they felt exhausted and had headaches after wearing masks.
Personally, I found that I experienced something a lot worse. When we were mandated to mask at my prior job I started noticing a pinning feeling in my throat. It’s hard to describe, but almost as if coarse hairs were stuck in my throat. It made me cough more often, and after eating lunch I would produce a ton of mucus.
It got to the point that I actually thought it was COVID (this was in the early months when no one could explain what exactly COVID was).
It turned out not to be COVID (at least from what the PCR result suggested), but that feeling lingered for quite a long time, and it was really only after I stopped masking that the irritation began to subside (it does still occur rather infrequently, but still does nonetheless).
Suffice to say, I was bought into a lot of the paranoia early on, and I wouldn’t be surprised if the masking had caused some harms to me. Ironically, I will state that the masking did help to wake me up to a lot of craziness going on as my COVID test led me to the every common issue of “take some Tylenol and call an ambulance if you have trouble breathing”.
I wish I actually kept that paper from when I had to get my test, but something about being presented with such a paper showed me that a lot of what was going on didn’t really make much sense. So I guess some good came from my long masking breathing issues. 🤷♂️
Long COVID Further Confounded
Now, one aspect of this systematic review that people have touched upon is the overlap between adverse consequences of masking as well as symptoms of long COVID, which include symptoms of headaches and fatigue.
The authors raise questions towards the possibility that some symptoms of long COVID may have been mistaken for issues related to masking:
Regarding the numerous mask symptoms an important question arises: Can masks be responsible for a misinterpreted long-COVID-19-syndrome after an effectively treated COVID-19 infection? Nearly 40% of main long-COVID-19 symptoms (171) overlap with mask related complaints and symptoms described by Kisielinski et al. as MIES (14) like fatigue, dyspnea, confusion, anxiety, depression, tachycardia, dizziness, and headache, which we also detected in the qualitative and quantitative analysis of face mask effects in our systematic review. It is possible that some symptoms attributed to long-COVID-19 are predominantly mask-related. Further research on this phenomenon needs to be conducted.
It’s important to remember that measures of Long COVID are so broad that most studies won’t be able to properly discern true Long COVID from symptoms relating to other factors.
Note that a recent study from Norway highlights the fact that most studies intended to capture Long COVID are inherently designed to fail- you’re essentially shuffling people from COVID negative to COVID positive groups.
Because of this there’s an incentive to argue that Long COVID doesn’t exist.
I’ve hammered this point before, but it’s worth repeating that nuance and acknowledgement of the unknown should always be used when looking at data.
More importantly, different ideas can be held at the same time without either being contradictory.
For instance, we can argue the following, along with caveats:
Long COVID is real and people may be suffering from different forms of post-viral syndrome
At the same time, most studies intended to look at Long COVID are designed to fail due to the use of such a broad diagnostic criteria that essentially captures a lot of background noise.
The extent of actual Long COVID sufferers are likely to be far lower than is reported. It’s important to remember that one cannot claim certainty based on ambiguity.
Above all, policies should not be designed on the basis of fear. Long COVID shouldn’t be used as an argument towards lockdowns, especially due to the lack of clear findings with respect to actual Long COVID suffers.
Apologies for those tired of hearing this point, but it’s an important reminder that much of the discourse requires more complex and nuanced thinking rather than to rely on reactionary rebuttals.
It’s quite clear that we may never actually get a true measure of Long COVID sufferers in the same ways we likely will never get true numbers of the vaccine injured. However, it’s important to always assess information within the context of unknowns.
*As a bit of an aside, it appears that many people are starting to move away from covering topics related to COVID. It’s a bit of a shame as there’s still so much left to be uncovered. At the same time, I can’t help but feel burn out from covering COVID.
Therefore, I’m hoping to return to doing a few seasonal posts in conjunction with COVID and other pharmaceutical-related posts. I interestingly went down a weird rabbit hole related to flower petals. If there’s anything spring-related that people would like to see covered please feel free to comment!
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Kisielinski K, Hirsch O, Wagner S, Wojtasik B, Funken S, Klosterhalfen B, Kanti Manna S, Prescher A, Sukul P and Sönnichsen A (2023) Physio-metabolic and clinical consequences of wearing face masks—Systematic review with meta-analysis and comprehensive evaluation. Front. Public Health 11:1125150. doi: 10.3389/fpubh.2023.1125150
Bees, please. and all manner of pollinators, from elephants to hummingbirds. Write away.
And thanks for your excellent work!
Thanks for covering this also ❤️🙏