


NAC & COVID
Examining some of the evidence for NAC use in treating and preventing COVID.

So far we’ve gone over some of the pharmacological effects of NAC and pointing to its ability to restore glutathione levels being its main mechanism of action.
Here, we’ll look at some of the clinical data in regards to NAC use against COVID and see what the evidence tells us.
A few important studies
Before we look specifically at COVID, I wanted to cite two studies that have been referenced quite a few times in the literature. These two studies are likely what was used to make a case for the use of NAC, similar to other repurposed drugs such as Ivermectin or Hydroxychloroquine which relied on previous clinical studies.
Attenuation of influenza-like symptomatology and improvement of cell-mediated immunity with long-term N-acetylcysteine treatment (De Flora, et. al.)
One such study that has been referenced multiple times is a study from De Flora, et. al. which looked at long-term NAC supplementation and whether that would attenuate symptoms of the flu during the cold season.
In this study, researchers provided effervescent NAC tablets1 to participants and measured their rate of influenza-like infection over the cold seasons. They also measured participants' cell-mediated immunity to see if NAC would have an effect on immunological responses to infections:
The present multicentric study, referred to as the NACIS study (acronym for N-acetylcysteine in Immune System), was designed in order to evaluate the efficacy of NAC, administered orally throughout the cold season, in preventing the occurrence and reducing the severity of influenza-like episodes in general, and specifically those caused by the influenza A/H1N1 virus. Another goal of this study was to assess the effect of NAC treatment on cell-mediated immunity.
The researchers found that the NAC group had fewer incidences of influenza-like symptoms and that symptoms were more mild within the NAC group compared to the placebo group:
Of the 99 influenza-like episodes occurring in 62 subjects within the placebo group, 47 (48%) were classified as mild, 46 (47%) as moderate, and 6 (6%) as severe, according to the criteria reported in "Materials and methods". Of the 46 influenza-like episodes occurring in 37 subjects within the NAC group, 33 (72%) were classified as mild, 12 (26%) as moderate, and 1 (2%) as severe. As assessed by χ2 analysis, the frequency of mild forms was higher in the NAC group than in the placebo group, with a difference approaching the significance threshold (p=0.06), whereas the frequency of moderate forms was significantly higher in the placebo group than in the NAC group (p=0.02). The differences were particularly pronounced by mid-season, after 3 months of treatment, when mild, moderate and severe episodes were 9, 22 and 3 in the placebo group and 8, 4 and 0 in the NAC group, respectively (p=0.002), and after 4 months, when mild, moderate and severe episodes were 10, 6 and 0 in the placebo group and 3, 0 and 0 in the NAC group, respectively (p=0.006).

Interestingly, the researchers measured cell-mediated immunity2 as well using a test similar to an allergy test, such that participants had their skin exposed to 7 different antigens to see if there would be a reaction (i.e. rash or other skin alterations). Given these limitations, the researchers found that long-term use of NAC increased the number of immunological competent (normoergic- their skin reacted to the antigen) participants and attenuated the number of nonresponsive (anergic-their skin did not respond) participants.

The results of this study are interesting, as both the NAC group and the placebo group started with the same cell-mediated response at month 0, suggesting that NAC may have helped improve cell-mediated immunity by the end of the 6 month assessment.
Overall, the results of this study provided some of the first looks into NAC as a possible prophylactic against respiratory infections. You’ve likely seen this study mentioned in reference to the 25% of NAC participants who experienced influenza-like symptoms compared to the 79% in the placebo group3. I've seen it referenced in many online articles as an argument in favor of NAC use for respiratory infections because of these findings.
As a caveat, note that some of the reporting provided to the researchers are heavily subjective and dependent upon the participant’s self-reporting:
Each subject was supplied with a personal diary card, and instructed to fill in any sign and/or symptom suggestive of an influenza-like episode, based on a suitable check list. Influenza-like episodes were assessed based on the presence of two or more of the following signs and/or symptoms: fever (≥38°C), asthenia, lack of appetite, headache, myalgia/arthralgia, coryza/rhynorrhoea, sore throat, catarrh and cough. At monthly intervals, the clinicians evaluated the diary card and performed a complete medical examination. The patients were also asked to contact the clinicians soon after the onset of any sign or symptom, and, whenever necessary, additional clinical examinations were performed.
As such, there’s a possibility that some patients may not have reported their symptoms which may have altered their symptomatic status (i.e. wrongly categorized them as asymptomatic, seroconverted). This is a general consequence of studies that rely on self-reporting since it’s hard to discern how transparent participants are being in their note-taking or awareness of their own symptoms.
However, given these results there was some founded hopes that NAC may serve as a useful prophylactic for influenza, and that use may be broadened to other respiratory illnesses such as COVID.
N-acetylcysteine improves oxidative stress and inflammatory response in patients with community acquired pneumonia (Zhang, et. al.)
A more recent study from Zhang, et. al.4 looked at the role of NAC in attenuating oxidative damage and the inflammatory response from pneumonia-like illness.
Oxidative damage and inflammation are intrinsically tied, and it’s assumed that these two are likely to lead to pulmonary damage during a case of pneumonia. Therefore, attenuating both should, in theory, lead to improved outcomes with reduced organ damage.
Patients who were diagnosed with pneumonia were randomized to either a group that was provided standard of care5 (control group) or one that was provided standard of care along with 600 mg of NAC twice a day (1200mg/day) for 10 days.
The diagnostic and inclusionary criteria were as follows:
The CAP diagnostic criteria were as follows: an acute pulmonary infiltrate evident on chest radiography and consistent with pneumonia; symptoms of a lower respiratory tract infection: fever, cough, and purulent sputum, with confirmatory findings of a clinical examination; acquisition of the infection outside a hospital, long-term care facility, or nursing home. The patients were included if they had the diagnostic criteria defined above, were diagnosed with bacterial community-acquired pneumonia according to American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) Guidelines[13,14] and if they were aged ≥18 years.
Because this study wanted to look at NAC in attenuating oxidative damage and inflammation, the researchers measured biomarkers from participants to see if there would be indications of improvement6:
The primary endpoint indicators were the changes in oxidative stress parameters (MDA, TAOC, SOD) and TNF-a after treatment in the NAC group compared with those in the nonNAC group. The secondary endpoint indicator was whether there was a difference in CT scores after treatment in the NAC group compared with the non-NAC group.
Relevant biomarkers were measured at the start of the study as well as at the 7 day mark. Improvements to biomarkers between the NAC group and the standard-of-care group showed that patients provided NAC showed greater improvement measures of the oxidative biomarker MDA as well as the inflammatory cytokine TNF-α relative to the non-NAC group. Measures of TAOC also appeared to have improved in the NAC group to a higher degree, however for SOD measures there didn’t appear to be significant improvements compared to the non-NAC group:
After 7 days plasma levels of MDA and TNF-a decreased more (MDA: p 0.004, TNF-a:p <0.001) in the NAC group than the non-NAC group, and there was a reliable increase of TAOC content in the NAC group (p 0.005). An improvement was seen in plasma SOD activity after treatment, but there was no significant difference in the rise of plasma SOD activity between groups (p 0.368). The results are shown in Table 3 and Fig. 2. No side effects were reported with NAC administration.

Interestingly, CT scan results, which were used to measure improvements with pneumonia, showed no statistically significant improvements in the NAC group compared to the non-NAC group7, inferring that pulmonary damage and pneumonia may not be alleviated through NAC use.
So although this study did not show greater improvement scores for NAC patients, the results do suggest that NAC may reduce oxidative stress and inflammation caused by pneumonia.
What’s important from this study is that the researchers used a highly accessible form of NAC (tablets) which would be easy to administer at an at-home environment, similar to the one given in the De Flora, et. al. study8.
However, it’s worth noting that this study used a very small sample size, likely driven by issues in recruitment9:
Initially 86 patients were considered for inclusion in the study. Twenty-nine patients were excluded and so 37 cases were in the NAC group and 24 cases in the non-NAC group. Eighteen cases did not complete the study. So, 39 pneumonia patients completed the study. Of these, 21 subjects were included in the NAC group and 18 in the non-NAC group.
This may have altered results due to not having the eligibility necessary for meeting effect size.
Also, note that the researchers never examined the etiological agent responsible for pneumonia, such that there was no information as to whether the pneumonia was caused by a viral, bacterial, or fungal infection. The researchers do rely on CT scans for diagnosis, as well as if participants met the guidelines for bacterial pneumonia from the American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA):
Another limitation is that the study did not record details of the etiologic agent. Patients in our study were diagnosed with bacterial community-acquired pneumonia according to ATS/IDSA Guidelines. For the pathological features, treatment and disease course of tuberculosis and fungus infection are different from those of bacterial pneumonia, patients considered to have tuberculosis or fungus infection were not included. Primary viral pneumonia was defined in patients presenting during the acute phase of influenza virus illness with acute respiratory disease and unequivocal alveolar opacification involving ≥2 lobes with negative respiratory and blood bacterial cultures. There might be some differences in oxidative stress status between bacterial and viral pneumonia.[26] Primary viral pneumonia cases were not admitted to the study either.
Since different infections are likely to lead to different levels of oxidative damage and inflammation, we should keep in mind that the results here are likely to be influenced by the type of pathogen i.e. no direct relationship to viral pneumonia in this study.
In short, these two studies- along with a few others not mentioned here- provide much of the basis for examining NAC within the context of COVID. Given these results it’s no wonder why NAC has been looked at, and considering that NAC is widely available (or at least used to be) it makes sense why research continues to look into NAC as a possible prophylactic and therapeutic against COVID.
NAC/COVID Clinical Studies
When looking at NAC with respect to COVID, I’ll be blunt and say that the results are conflicting. Heck, the results are conflicting for clinical studies of Ivermectin, Hydroxychloroquine, Fluvoxamine, Remdesivir… you get the idea.
Therefore, it’s sometimes more important to parse out differences in methodology rather than the actual results, as differences in results could alter the conclusions of a clinical trial. Remember that this heterogeneity is found in many clinical studies which makes it hard to directly compare studies.
Here are few things to look out for in clinical studies:
Dosing: Differences in dosing are going to have an effect, such that higher doses may be more therapeutic while also increasing the likelihood of adverse reactions. Note that studies may not have a standard therapeutic dose and the dose used may be one derived from prior studies rather than ones that have shown a good degree of effectiveness.
Loading dose: Some studies may also use what’s called a loading dose followed by a maintenance dose. A loading dose essentially provides a high level of the drug/supplement up front followed by lower doses, with the assumption that quickly ramping up the serum levels of a therapeutic within minutes bypasses the gradual increase that may take hours or even days, meaning that therapeutic levels can be reached more quickly. It may also attenuate much of the metabolism that occurs through the first pass effect, with the caveat that toxicity may occur as a consequence. Note that some studies may or may not use a loading dose and that may influence results.
Timing: What should be made clear at this point is that timing of a therapeutic is important. For the most part, early use of an antiviral therapeutic is better- target the pathogen at very low levels before there needs to be concerns over balancing damage from the pathogen and possible adverse reactions from the therapeutic. However, remember that the therapeutic effects should still match the disease. COVID is considered to be at least a biphasic disease with viral infection being followed by systemic inflammation of multiple organs. This means that the timing of NAC should corroborate with the intentional use of the drug- could early NAC use affect the inflammatory response needed to mount a proper immune response against an antigen, contrasted with late use during a cytokine storm that may attenuate the oxidative damage and hyperinflammatory response? It’s worth examining what the intended use of NAC is within a clinical study to understand if the timing seems appropriate with respect to the MOA.
Route of administration: A few studies will either rely on oral or intravenous administration of NAC. Remember that oral use suffers from low bioavailability due to the first pass effect with the pro being that oral administration is far easier and can be done at home during the early stages of the infection. Intravenous NAC use may increase serum levels more quickly with the caveat that it may require an in-hospice setting.
Measures of Improvement: Results are interpreted based on the markers being measured. As such, the results of some studies are contingent upon which measures are looked at. Some may look for biomarkers indicating oxidative stress or inflammation such as the Zhang, et. al. study while others may look at oxygen levels, mortality, and days hospitalized. Keep in mind that the interpretations of results rely on the measures taken.
There are likely to be a few more things worth considering, but we’ll look at a few studies and examine differences in methodology.
A pilot study on intravenous N-Acetylcysteine treatment in patients with mild-to-moderate COVID19-associated acute respiratory distress syndrome (Taher, et. al.)
The first study we’ll look at is one from Taher, et. al.10 that intended to use NAC to treat COVID during the early stages of ARDS. The intended use of NAC within this study was to see if NAC could dampen the excessive inflammatory response during ARDS:
Considering this evidence, it is speculated that NAC target multiple mechanisms related to COVID-19 excessive inflammation. Thus, it is reasonable to assess NAC as a potential therapy for COVID-19. However, at present, clinical information on using NAC for COVID-19 treatment consists almost exclusively of single case reports [21–23] and one small case series study [24]. Hence, we designed this double-blind, placebo-controlled study to determine whether patients with mild-to-moderate COVID19-associated ARDS would benefit from intravenous NAC administration as adjuvant therapy to standard therapy.
Patients were randomized to either receive intravenous NAC at a dosage of 40mg/kg/day11 diluted in a 5% dextrose solution for 3 days. The placebo group was given intravenous dextrose solution alone. All participants were also given antioxidant supplements such as Vitamin C (1000 mg bid), Vitamin D (1000 mg bid) and Zinc (50 mg daily).
It’s also worth noting that a majority of participants also received other medical interventions such as Hydroxychloroquine, Dexamethasone, Azithromycin, and other antiviral agents (Table 1).
Primary outcomes looked at 28-day mortality rates and measures of clinical improvement:
As the primary efficacy outcomes, the following were compared between the two groups from baseline up to day 28 post-randomisation: (1) overall 28-day mortality, (2) clinical status on study day 28, using an 8-point ordinal scale of the WHO Master Protocol (V.3.0, 3 March 2020) […]
Secondary outcomes included measures such as ventilation, ICU/hospital stay, and measures of organ damage and ARDS.
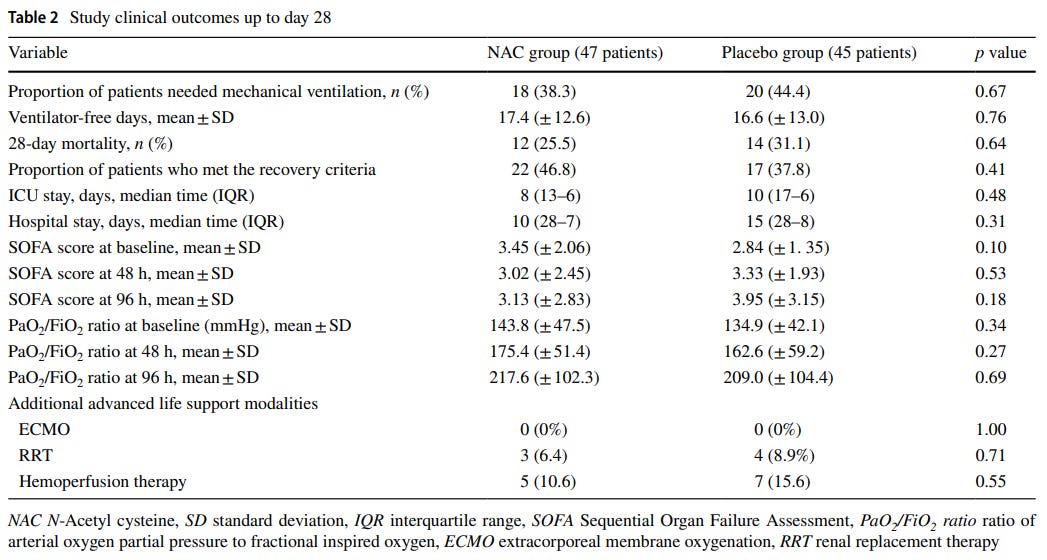
Although the results showed reduced mortality and greater improvement among the NAC group the results did not meet statistical significance:
According to the obtained results, although the overall 28-day mortality rate was lower in the NAC group than to the placebo group [12 of 47 patients (25.5%) in the NAC group vs. 14 of 45 patients (31.1%) in the control group], no statistically significant differences were found between the two groups (p value = 0.64; Table Table2).2). Results regarding the comparison of the distribution of the clinical status at day 28, using the 8-point ordinal scale of the WHO, are shown in Fig. 2. Although the distribution of the clinical status at day 28 in the NAC-treated group shifted towards better outcomes than did placebo-treated group, it did not reach a statistical significance level (p value = 0.83).
And it appears that secondary outcomes were comparable among the NAC groups and the non-NAC groups (Table 212).
Based on these results the researchers suggest that NAC did not appear to improve clinical outcomes within their study.
There’s a few possible reasons for this, with one clear observation being that the 3-day use of NAC may not have been long enough to see improvement.
There’s also an issue of timing. Median time of symptom onset for these patients was 7 days, but note that this symptom onset period is likely referring to the initial start of the disease and not the start of ARDS symptoms, although the measures used to diagnose ARDS appear to be consistent with other studies13. With no indication with time of ARDS onset and start of therapeutics (aside from diagnosis at time of hospitalization), it's hard to determine if delayed use of therapeutics may influence the response. Granted, it may be assumed that hospitalization may occur immediately after ARDS symptom onset. It's also a bit of an oxymoron to suggest mild-to-moderate ARDS symptoms.
One thing that may be worth considering is the cellular stress occurring during ARDS. Given the prior post on NAC’s mechanisms of action, it appears that it is Glutathione and not NAC that is the main active metabolite responsible for antioxidation.
That would mean that cells must uptake NAC, have it undergo deacetylation to form L-cysteine within the cytosol, and then enter into the necessary enzymatic pathway to form GSH.
Although this may be readily achieved under normal or mild cellular stress, this may not be possible when cells are undergoing severe stress and damage already- the cells may not have the capacity to produce GSH. This may explain why NAC may be considered ineffective during symptoms of ARDS, and if that’s the case it may be worth looking into use of GSH rather than NAC to bypass the necessary enzymatic reactions that may not be possible under high cellular stress.
So severe symptom onset may not be just a consequence of GSH depletion, but also the cells’ inability to initiate GSH repletion as well when under high stress.
Overall, the results of this study may be a consequence of implications and hindsight- when patients may need to start presenting with worse symptoms before they are given treatments they may paradoxically be too deep into their infection. It’d be impossible for researchers to determine who may convert over from typical flu-like symptoms into ARDS, but it may also be argued that use of NAC may not wait until it’s too late.
Although the general evidence for NAC use is conflicting, the researchers do suggest that additional research should be done into looking at NAC:
However, although the current clinical data are conflicting, there is a rationale to study NAC as an adjunct therapy to prevent and treat COVID-19 infection. Research has revealed that despite the potent antioxidant and anti-inflammatory effects of NAC, unlike glucocorticoids with intrinsic immunosuppressive drawbacks, NAC is not immunosuppressive. In fact, NAC not only does not increase the risk of infections but also, through regulatory actions on the immune system, may decrease the risk of infections [33].
Combined Metabolic Activators Accelerates Recovery in Mild‐to‐Moderate COVID‐19 (Altay, et. al.)
This study is rather exhaustive so we won’t go into too many details. However, unlike the Taher, et. al. study this one looked at patients with mild-moderate COVID symptoms and whether the use of metabolic activators could lead to quicker and better improvement of patients.
Metabolic dysfunction is considered to be driving factor for many different diseases including COVID, so it was assumed by the researchers that a combination of metabolic activators (CMA) should be beneficial in fighting COVID.
In this study, researchers deployed a combination of L-serine, L-carnitine, and NAC. Some participants also received standard of care which included Hydroxychloroquine or Favipiravir14:
Treatment started on the day of diagnosis. Both placebo and CMA were provided in powdered form in identical plastic bottles containing a single dose to be dissolved in water and taken orally one dose in the morning after breakfast and one dose in the evening after dinner. Each dose of CMA contained 3.73 g l‐carnitine tartrate, 2.55 g N‐acetylcysteine, 1 g nicotinamide riboside chloride, and 12.35 g serine. All participants also received oral HQ or FP for 5 d. The patients were contacted by telephone daily to assess symptoms and adverse events. All patients came for a follow‐up visit on Day 14. Further information is provided in the Appendix in the Supporting Information.
This study is interesting since it was one that did not provide weight-dependent doses. It’s also an early study with people being recruited at time of PCR positive testing.
It’s also worth noting a few concerning details, such as randomization leading to a 3:1 ratio between CMA groups and standard of care, so the group sizes are not comparable. Also, note that this study skewed younger (mid-30s) than other studies and most participants did not have comorbidities, which may explain the positive results in this study compared to other studies.
The important results here would be from Section 2.1 and 2.2, but I’ll take from the 2.2 results which looked at the number of days until symptom-free onset until Day 14.
Fortunately the researchers provide an easy to read chart and graph:

Part A outlines the study timeline, with Part B being the more important graph here. CMA participants are shown in blue while Placebo group is shown in orange. The graph maps the number of days until a participant has been considered to be symptom free from COVID, and the results suggest that symptoms alleviated far quicker in the CMA group than the Placebo group with half of the participants becoming symptom-free by day 6 and day 9 respectively. Interestingly, CMA participants appeared to have no more symptoms by day 10.
Although both groups were provided either Hydroxychloroquine or Favipiravir, the researchers conducted a separate analysis controlling for these drugs as possible confounders, and the results suggest that CMA reduced days of symptoms independent of the additional drugs:
We observed that the mean recovery time was again shorter in CMA group than in placebo group (5.76 vs 9.32 d, p < 0.0001) in the patients treated with HQ only (Figure S1A, Supporting Information) and (5.54 vs 8.77 d, p = 0.00034) in the patients treated with FP only (Figure S1B, Supporting Information). We also compared the independent effect of the HQ and FP on COVID‐19 patients and found that these two drugs had a similar efficacy on the recovery of the patients in all (Figure S2A, Supporting Information), placebo (Figure S2B, Supporting Information) and CMA (Figure S2C, Supporting Information) patient groups. Hence, we observed that CMA administration accelerated the recovery of the COVID‐19 patients independent of the standard therapy.
As an early treatment option these results seem very promising. However, there is an issue of these results being highly subjective. Symptom measures were taken over the phone and only a full medical examination was given at the 14 day mark, suggesting that patients may not have been transparent about their results. Symptoms are also not an indication of infection, so there are some tenuous associations as well:
For the primary purpose, the proportion of patients who fully recovered from COVID‐19, as demonstrated by being symptom free within the 14 d of the initial diagnosis of COVID‐19, was determined. This was amended to include self‐reporting of daily symptoms and clinical status using a binomial scale (present/absent) via daily telephone visits by clinical staff.
There is also the matter of NAC being given in conjunction with other supplements that may confound the results as well.
But even given these caveats the study does provide some promising results, especially within the context of early use therapy.
Should NAC be used for COVID?
Although we covered a few studies here there are quite a few that have not been evaluated. In essence, the results are conflicting, likely due to methodology.
The Taher, et. al. study looked at NAC within the context of ARDS, and at that point the use may be considered too late. Compounded with the fact that cells may be under too much stress to produce GSH there may be arguments that GSH may be considered a more rational supplement to use.
The Altay, et. al. study has quite a few caveats but does provide some promising results for early use where NAC may be more beneficial. This is taking into account that control of inflammation itself does not attenuate immune function, which was argued against in the Taher, et. al. Discussion.
But probably the most important feature from all of these studies is that there appears to be overwhelming evidence in support of the safety and tolerability of NAC. Even if the drug in question may have conflicting evidence, the lack of egregious toxicity and adverse reactions should suggest that NAC use not be hindered by concerns over possible toxicity.
Hopefully as more studies come about more evidence can substantiate the use of NAC. For now, remember to do your own research and seek out additional medical advice to see if NAC would be viable for your given circumstances.
And apologies for this rather long-winded post, the next one will hopefully be much shorter and just be a look at L-cysteine, NAC, glutathione, and why one may be used over the other.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Experimental group were told to take one 600 mg effervescent NAC tablet twice a day (after breakfast and at bedtime). Placebo group was given effervescent tablets to control for blinding.
Given the methodology, cell-mediated immunity was measured based on a skin test in which participants had 7 different antigens applied to their skin. Formation of a rash or skin reaction was considered to be indicative of an adequate immune response (normoergic) while no skin reaction was classified as having no immune response (anergic):
In particular, the subjects were classified as: anergic in case of total absence of skin reactivity to any antigen; hypoergic in case of skin reactivity to ≤2 antigens yielding a cumulative skin reaction diameter <10 mm; and normoergic in case of skin reactivity either to ≥3 antigens or ≥2 antigens when the cumulative skin reaction diameter was ≥10 mm.
Therefore, keep in mind that these results are somewhat quantitative. I’m not sure to what extent this study would be considered standard in the immunological field, so I can’t provide any additional context.
The takeaway from this method is one similar to allergy tests, with the assumption that a rash or other skin reactions is indicative of an immunological response to target the given antigen.
Refer to Table 3 of the study for those numbers.
Zhang, Q., Ju, Y., Ma, Y., & Wang, T. (2018). N-acetylcysteine improves oxidative stress and inflammatory response in patients with community acquired pneumonia: A randomized controlled trial. Medicine, 97(45), e13087. https://doi.org/10.1097/MD.0000000000013087
Standard of care provided by the researchers were rather ambiguous:
The conventional pneumonia medication included: antibiotics, expectorants, and antitussives.
The study uses a few measurements to determine oxidative stress. For instance, MDA refers to the compound Malondialdehyde, which is produced during fatty acid peroxidation of membrane fatty acids. It essentially serves as a marker to indicate that oxidative damage is occurring; higher levels of MDA indicate more oxidative damage, as it is assumed that the presence of MDA suggests a high oxidative environment.

TAOC refers to Total Antioxidant Capacity, and is a measure of blood serum or other bodily fluid’s antioxidant capabilities. It’s a general term that encapsulates different biomolecules such as antioxidant enzymes, proteins, and vitamins and may not provide a quantitative measure for specific antioxidants. As such, note that this term has been somewhat controversial as it doesn’t relate directly to specific antioxidants. For example, within the context of NAC is higher antioxidant capacity related to elevated glutathione levels through NAC administration, is it NAC itself, or is NAC/GSH attenuating cell damage allowing other antioxidant enzymes to be produced? TAOC assays aren’t intended to provide an explanation of which antioxidant is present, but is a measure of how much.
SOD refers to the enzyme Superoxide Dismutase which is responsible for converting superoxide, an extremely reactive oxygen species into the less reactive hydrogen peroxide. Note that hydrogen peroxide itself can cause oxidative damage, but relative to superoxide it is considered less toxic. Within this chain of reactions hydrogen peroxide is then converted into water and oxygen by the enzyme catalase, although this enzyme is not being measured in this assay.
 - Chemistry LibreTexts")

The Zhang, et. al. study doesn’t indicate which tablet was used, so I assume it was an effervescent tablet similar to the one used in the De Flora, et. al. study.
Many of these patients were excluded for old age or for other comorbidities, including prior diagnosis of viral pneumonia:

Taher, A., Lashgari, M., Sedighi, L., Rahimi-Bashar, F., Poorolajal, J., & Mehrpooya, M. (2021). A pilot study on intravenous N-Acetylcysteine treatment in patients with mild-to-moderate COVID19-associated acute respiratory distress syndrome. Pharmacological reports : PR, 73(6), 1650–1659. https://doi.org/10.1007/s43440-021-00296-2
If we assume the average male size to be 75 kg, that’s about 3000 mg/day given intravenously.
Measures of ICU stay as well as oxygen levels were considered to be comparable.
All Patients with a diagnosis of mild-to-moderate COVID19-associated ARDS admitted to the hospital were screened for enrolment in the study. Patients were eligible if they were: at least 18 years; had received a diagnosis of COVID-19 defined as either the positive SARS-CoV-2 on polymerase chain reaction testing (RT-PCR) in a respiratory tract specimen and/or clinical and radiological findings compatible with COVID-19 severe pneumonia, met the criteria for mild to moderate ARDS using the Berlin criteria [4] defined with oxygen saturation of less than 94% at rest on room air (i.e., with no supplemental oxygen) or the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2 ratio) of less than 300 mm Hg and more than 100 mm Hg, and less than 48 h from their hospital admission.
It appears that participants were given either one or the other, so there would be issues in considering whether one drug may have had a greater effect than other when examining the results.
Very much looking forward to your next post comparing L-cysteine, NAC, and glutathione, in particular for healthy individuals that were vaxxed and then experienced mild to severe covid vaccine adverse effects (e.g, irregular heart rate). Some thought on supplementing a omnivore diet vs. vegan/vegetarian diet might also be of use, as well as answering whether this should be a daily supplement or whether it should be temporarily taken until any adverse effects appear to have stopped. The question of the future availability/accessibility of these products might also be an interesting factor to address too. Other supplements of interest are PQQ and DMG. How these relate to glutathione-related supplements or other considerations of use would also be appreciated.
I’ve been supplementing with NAC and Glutathione for a couple years. I think it’s a real big boost for one’s immune system. When I heard a few doctors (alternative media of course) recommend these supplements among many, I thought it can’t hurt. I think it helps immensely with the healing process of your body! I just had a cancerous uterine tumor removed (in hospital for 3 days), cancer gone and I healed well! Praise God!