After posting, I probably should have asserted that this at least suggest that vaccines are not better than natural immunity- they are at least comparable, with the slight caveat that natural immunity may have a better ARR, or may not wane as suddenly as vaccinated.
I suppose if we want to get antagonistic, us natty folk can circle around the vaccinated and chant "one of us":
Yes, I'm not quite sure why he banned people. Do you know of how many people he banned?
I usually try to stay out of the drama since that enters into the whole social media side of this stuff. I did watch part of his livestream (I believe for Novavax and the FDA briefing) and there was a section in which he was describing his background. I suppose it's a point for many to attack him with because he was not trained in the US, so maybe that is part of it?
I tend to agree with natural immunity. The study at least indicates it lasts longer than the vaccine (slightly). I think the predictive model may be one to be careful of (protection 3 years on). I just wish we had more studies to come to better conclusions.
Ah I see! Honestly the moderators can be strange on all social media sites. It's somewhat a thankless job, and yet it's a role in which people may (whether intentionally or not) exert power onto others they may not normally have. Reddit is notorious for such a thing, as are some Moderators on Youtube. One generally hopes that the streamer would notice and respond to Moderators.
Considering it's not Dr. Mobeen himself, it does help a bit in his favor. Sometimes Streamers may have no idea what's going on, which can be unfortunate for such a situation as this. And honestly, I hope you wouldn't feel as if you need to censor yourself lest someone see such remarks. That may just enter into the realm of pettiness on the Moderator's behalf. But I suppose I should leave it at that.
Very interesting! When I read these kinds of studies, I always remind myself that PCR tests sometimes are false positive, giving something like 2% false positives. So if you test 1,000 people three times, you would get incidence of 60, or 6% or so, even if none of them had Covid.
This brings up a question that is actually burning in my mind: WHAT IS A REINFECTION?
For example, let's say that I, a previously infected unvaccinated individual, come in close contact with an ill person. Am I "reinfected" if I test positive some time later, despite having no symptoms?
The reason for my question is that last winter, my wife had Covid and I took care of her and did not get ill. After a week or so, I realized that on one recent evening I did feel slightly funny in my nose, which was such a fleeting feeling that it was possibly nothing at all.
But I always wonder, unfortunately without a definitive answer, what if that evening I did a PCR test on my nose and came up positive. Was I "reinfected"? It is a question to which I do not know the answer to, but it is very important for me and for all people.
My own answer, which is probably not perfect, is that a properly defined reinfection must at least involve symptoms such as fever and viremia and a reasonably low Ct threshold.
This study seems to define reinfection as a "positive PCR test", which always makes me wonder how many of those reinfections were not true illnesses.
For all intents and purposes, it appears as though reinfection and breakthrough are measured by PCR tests. The article from science considered breakthrough infections in some of the HCWs yet a good portion of them were asymptomatic- they only tested positive. And so in many cases asymptomatic infection tends to be included within the analyses.
There's a lot of variables when it comes to testing. As someone who used to do PCR testing I kind of saw how sensitive the tests were. It's generally why I avoid looking at case reports as some measure of what's going on. When you're told from the beginning that 40% of infections are asymptomatic, we should be cautious in assuming that all infections now (and reinfections) would be symptomatic in nature.
So we have to work within the parameters of the study, and generally look at these studies with some qualifier. Something along the lines of "reinfections are occurring [as confirmed through a positive PCR test]".
Thanks for highlighting this one, since at this point I reflexively avoid studies from Qatar because they're usually test-negative-controlled junk.
Note 1 on ARR is that a rational choice for the time-span is required. No time-span that doesn't include at least one full wave makes much sense. On the other hand a time-span that includes both a before and after-wave lull also might not make sense. But at the same time, waves are not alike, so the absolute risk reduction through one wave won't be the same through another, as in Alpha vs Delta (very few cases) vs Omicron for Qatar. This is really something that just needs to be scrutinized on a study-by-study basis. For example the CDC MMWR almost always selects stupid time spans.
Note 2 is that vaxxes almost certainly perform differently according to to-wave-injection-timing. So a low absolute risk reduction if injecting before a lull would probably look much better if injecting before a wave. Both the trials and the mass roll-out timed things unfavorably in this regard in most places (though Canada had a spring 2021 wave and so the timing was more favorable there).
Note 3 is that vax timing will probably never be perfect in practice. So you would want to look at natural immunity's durability through that lens - in practice, a lot of vax injections are going to give zero return on investment because of bad timing. Natural immunity doesn't seem to have this problem.
Alpha infection efficacy vs Omicron is interesting. I would think the Alpha wave had the most accurate distinction between infected and not due to better testing vs 2020 + higher case rate vs Delta. Maybe there is a bias for higher unrecorded 2020 infections in the control group (because they were less likely to be a positive in Alpha) and so the control group performed at a better-than-naive rate in Omicron. Don't know why that wouldn't be the same for Alpha vs Delta though...
You know Brian, thinking about it I probably jumped the shark in the inclusion of the ARR. So much for restraining myself. I should have remembered that the clinical trials were limited to 28 days, and so to do such a calculation was DEFINITELY improper.
I'm not sure with the Alpha portion. I suppose that would require sifting through prior Qatar data to figure out that factor. I was wondering about variants and cross reactive immunity, but I believe studies looking at neutralization or just RBD antibodies usually indicate that Beta is the variant that has the strange drop-off (unless I'm mixing it up with Alpha).
That sort of sounds more like the ancient Planas, et al study which compared post-Wuhan infection (at 12 months) and vax-based (at week 16) binding vs Beta / Alpha / Delta and generated mad headlines because no one ever knew that antibodies are meant to fade over time.
*edit OK actually this one is pretty directly on point https://www.nejm.org/doi/full/10.1056/NEJMc2119236 - all the VOC-convalescents do badly vs Omi, but I guess Beta the worst. However, a quick trip to Supplemental Table S1 shows that the Alpha were middle-aged, Beta almost all 80 year-olds, and Delta young adults. lol.
Oh yes, the biggest factor of all- old, withered B cells biasing the results! I kid, but seriously shouldn't we talk of immunosenescence a lot more than is already discussed? Not only are the elderly more susceptible, but they're the ones to least likely to be able to produce the antibodies and immune response necessary against a "novel" coronavirus.
And I don't think it's from just that study. It feels like all studies reported that Beta was the wonky variant, but again all of these studies were immunological shake and bake so there's already that problem.
Also, the Qatar study presents with a strange situation since they mention the number of international workers (which also tends to skew young- another hit for the ARR tangent), and I think you were alluding to that. So there's the dynamics of accuracy and consistency at play here.
This was an interesting slightly eye opening interview. Still trying to fathom, why such an enforced myopic solution? Israeli Vaccine Chief: We have made mistakes:
7.30 on: “I’m all for a nasal vaccine for example”…
….that would be able to better mimic the immunity we get from the disease”…..
It’s interesting that Novavax is supposed to also have epitopes as well as just the spike focus, although it’s probably out of date as not targeted to the current omicron I believe? Also there was a vaccine design with no spike, which we don’t talk about much, which apparently is looking to be a pan coronavirus vaccine, trying to copy what a healthy young immunity does re “memory B cells that bind SARS-CoV-2 and weakly cross-react with other coronaviruses”, again poss an epitope vaccine moving away from just the spike.
So, what's interesting is that flu vaccines should have pointed us to the issues with an intramuscular vaccine. There's been plenty of questions as to whether influenza vaccines are not very effective because they are not introduced in a manner that follows the route of infection (i.e. intranasally). It's a bit ironic that a new vaccine vehicle was provided in the old manner, but there is the issue with mRNA and dispersion if provided intranasally.
Novavax supposedly has the spike protein studded on the surface of their carrier structure called an ISCOM. It'd be interesting because it's one of the only vaccines that would avoid your body needing your body to produce the spike, and so that makes one wonder if that would be considered safer.
I would like to hear about that vaccine with no spike. I'm not sure how that would come to fruition, mainly because if one were to stop the virus from entering cells you would target it via the spike. It's the main paradox with the vaccine in which the cure (prophylactic) may be the disease in this scenario.
Thanks for the link re Novavax. Yes, the conclusion seems to be that a myopically targeted IM vax is not very good for this type of virus.
Novavax maybe better just re non mRNA and poss. PEG problems for some. As you mention it has still been flagged re myocarditis as they all are; I’d like to understand why that is. Also more about the spike? re: https://youtu.be/mbaQNKXh7qg
This is a link discussing a poss ‘pan coronavirus’ vaccine. The original link was moved when I shared it and the new link also had removed the statement which discussed healthy young immune response etc. being a clue for poss future vaccines. How well it would work I’m not sure, or if it will go anywhere?
There was also a study recommending perhaps an epitope vaccine, but that study was not well received shall we say, because it suggested problems with the spike, I think Merogenomics also did a vid looking at that.
Valneva was going to be produced in the UK, it’s supposed to be a traditional deactivated virus and adjuvant. However the UK said it wasn’t going ahead re the company broke contract, which they deny. The UK then said they wouldn’t have approved it anyway, but the reasons were not made clear. However since then we have a billion deal with Moderna. Apparently the mRNA hasn’t performed as well as its other maligned competitors, I need to find the info link where that was said, but we have high Gates influence in the UK press and MHRA.
There is talk now of nasal solutions as well, which has been presented before, apparently a while ago Israel even had one stating it helped prevent coronavirus by over 95%, but I’m not sure what happened to that, but others are now emerging. Even talk it will eventually be something you just buy over the counter? Everything seems to depend on influence of vested interests, rather than what might actually be better.
A friend of mine had an anti body positive test over a year and a half later, nearly two years with natural immunity. The question is what other aspects of immunity other than certain antibodies are happening via the current vaccines, as I believe you mentioned in another article?
Covid for me was 2 days achy, a week of a cold, but with less coughing than a prior respiratory virus and less nose blowing than a cold and two weeks feeling a bit more fatigued, no vax, so natural immunity.
I caught it from my partner who had 2xAZ, but won’t be having boosters. He unfortunately developed headaches which were of concern and long covid like symptoms and wasn’t quite himself for a few months. When he then got covid we treated him the second day with an early treatment protocol. He had flu like symptoms was a rough for 3-4 days and then after a week felt better, no major cough, but was fatigued for 2-3 weeks. However after that he then felt more like his old self, before the post vax problems, which seem to have resolved touch wood. He is also diabetic so more vulnerable category. I also added other recommended vits minerals , enzymes etc. which I also took. Our son had a cold for a week and mild dry cough, natural immunity.
We have so many studies out about the robustness of natural immunity, but like the one you mentioned it would be good to have more. Myself and son are in a natural immunity control group, monitoring general health of people and to see how often they get covid etc. Its trying to get approved recognition, so good luck to them with that!
It’s a coronavirus, even a souped-up one was always going to mutate and prob join all the other coronaviruses that circulate, I’m not sure the myopic presented ‘solution’ has made that any better, I would say worse…
Yes, I wrote another post a while after the Novavax one when the myocarditis concern was raised, suggesting that the spike protein is the main culprit. We sort of knew that, since studies came out indicating that the spike was cytotoxic, and so it really wouldn't make sense how the spike from the vaccine would be nontoxic but the one from the virus is, when they need to be antigenically similar in order to produce immunity against the virus.
One of Joomi Kim's first Substack posts discussed the spike, and it's likely that the cytotoxicity of the spike wasn't recognized until the vaccines were in development.
Thanks for the link. Honestly, articles such as that are frustrating because it feels like it takes forever for them to discuss what the article is about, and when they do is muddied from being surrounded by other ramblings.
I think this is the important part:
"The research team identified one particular receptor-binding domain site that is present on SARS-CoV-2, its circulating variants and SARS-related bat viruses that makes them highly vulnerable to cross-neutralizing antibodies. [...]
"Basically what we've done is take multiple copies of a small part of the coronavirus to make the body's immune system respond to it in a heightened way," Saunders said. "We found that not only did that increase the body's ability to inhibit the virus from causing infection, but it also targets this cross-reactive site of vulnerability on the spike protein more frequently. We think that's why this vaccine is effective against SARS-CoV-1, SARS-CoV-2 and at least four of its common variants, plus additional animal coronaviruses.""
And so they essentially looked for a region with conserved epitopes across different coronaviruses, rather than use the entire spike. This is interesting, however to what extent this region remains conserved is a predicament. I suppose it's something to look out for, and there may be still be questions if that conserved region is still bioactive (may still be cytotoxic).
Wow, I'm sorry he had to go through that. It's difficult, because given our situation we may have this slight inclination to see a situation and go "yes, it's the vaccines that are making it worse!" Or I'm at least speaking for myself at the moment. In reality, there could be so many factors as well and it's so hard to figure out the relevant information from all of the noise that's going on right now.
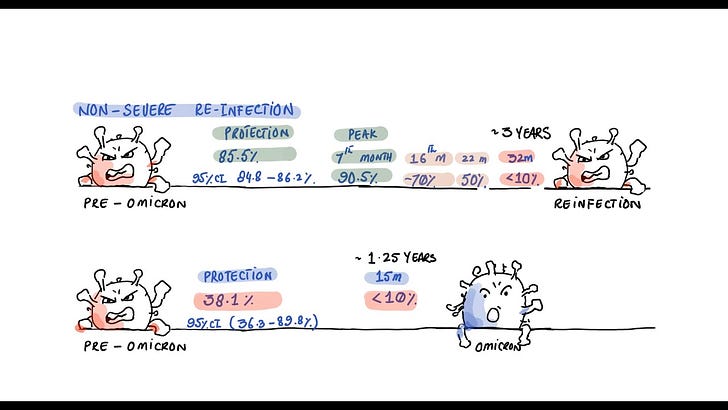
One of the biggest issues is that many of those natural immunity studies came out pre-Omicron, so we don't know anything about this current Omicron era. I think the findings of this study are important since it at least tells us that natural immunity may not be protective against Omicron, and that would at least explain the "blank slate" situation for many of us (not quite blank, but not sure what other phrase to use here). The problem now is that we need more studies like these, but it's likely that we won't be provided that possibility anymore.
The protocols so are likely to have done worse, mostly because it halted immune training for the entire world by telling us not to interact with others. For us adults, it may not be too bad since we have had years of immunological training through getting sick, but for children they missed out on two critical years of learning for their immune system. Ironic that children are behind in both school and their immune system. I wrote about this phenomenon which some scientists referred to as "immunity debt" and may explain why children are getting so sick, and with pretty serious symptoms.
It's just another reason why we have screwed ourselves and younger generations with such a ridiculous global policy of lockdowns for a virus that apparently 40% of infected people present asymptomatic for.
I completely agree. Thank you for the detailed response, it’s much appreciated, as are all the critiques and in depth research around this. Yes, regarding immunity debt. However as yet, I’m not so forgiving either over the continued deliberate lies and abuse of power around this. Genuinely misguided, inept, corrupt or both…
Certainly we can be critical of those in power who continue to lie and pit us against each other, but we have to keep in mind what is important. We can criticize the vaccines, those in power, and all those factors but we should also make sure to remain rational when we look up the information.
Thanks for the reply. Your answer does help some; I now better understand the limitations of the study (its narrow focus). So then, what role does the Innate system play in protection against reinfection? Or, is it that the Adaptive system will always dominate? Argh! I'm still so confused.
That's a nuanced answer as well. Generally speaking, the innate immune system is in charge of all types of infections. It's nonspecific, so it job is to target anything that doesn't seem quite right unlike the adaptive immune system which essentially plasters "Wanted" posters all around alerting the immune system what specifically to look for. I believe it's the innate immune system that actually leads to the hyper-inflammatory state in COVID (or at least plays a large role). There is also an idea that the innate system is actually trainable, although to the extent that trained immunity lasts I am not sure.
In general, both work together with the innate immune system indiscriminately killing things that should be there while the adaptive immune system selectively targets the virus. It's generally believe that the adaptive immune system helps to mount a quicker attack via recall. I think it makes it difficult because we usually consider them separate when they work in tandem.
And don't be worried about being confused! Honestly, all of this immunological stuff is new to me and so there's tons I either still don't know or will get wrong. The problem isn't the confusion, but understanding that this whole thing is a continuous process of learning. Try to overcome the confusion and learn to parse the information.
I'll also say, confusion is not a bad thing. Confusion tells you that you're dealing with a lot of information and trying to relate them together and making sense of all of the information. I think it's much better to be confused rather than to be obstinate. So really don't beat yourself up over being confused. I'd be surprised if you weren't! Just learn how to grow and move away from the confusion.
The more I learn the more confused I become. It was my understanding that the benefits of natural immunity over vax immunity was in the overall protection granted by natural infection (immune system interacting with all parts of the virus) compared to the highly specific (a particular protein of the virus) protection conferred by vaccination. {while noting that the benefit of vaccination over natural infection is in the risk reduction of severe outcome}
Now, is this no longer correct? Was this just an Immunology 101 myth? This paper, and your analysis, seems to suggest so. Unless I'm misunderstanding something, of course.
No, and apologies if I have confused you with this post. Naturally immunity certainly is broader (targets different proteins), but in the grand scheme of protection we have to look at the utility of targeting other proteins. In the case of a viral infection, the main concern is stopping the virus from interacting with our cells in the first place. The best way is to stop it from binding to our receptors, and in the case of SARS-COV2 that means targeting the spike. Both natural and vaccine-induced immunity hopefully leads to this end goal.
Now, it is true that other proteins will be targeted via naturally immunity. If we take the Nucleocapsid protein we know that we produce anti-N antibodies against this protein (it's how the CDC originally differentiated natural immunity from vaccine-induced immunity by looking for anti-N antibodies in blood sera).
However, what does the Nucleocapsid protein do? Well, the N-protein is responsible for winding up the viral RNA and making it more compact. Therefore the N-protein is sequestered within the virus.
This raises questions then- how would I target something that resides inside the virus? Our antibodies don't know it's there, and there's no way for the antibodies to squeeze into the virus to find those N-proteins. Because of this, the N-protein only makes itself known after a virion infects a cell, causes more N-proteins to be released as well as the N-protein that may explode outward if one of our cells lyse.
And that's the general issue. At the point that our immune system is made aware of the N-proteins the virus is likely on its way of undergoing massive replication. One of the only ways to target the protein is during viral replication, and if we target N-proteins that have spewed out of a cell that doesn't stop the actual virions from going to other cells and infecting them.
This is a long-winded response, but although we have broader immunity against other viral proteins the important factor is figuring out which ones stop the virus from infecting in the first place. That's why the N-protein is not the go-to protein to target, because it's not involved with infection like the spike protein is.
So hopefully that clears it up. A study such as this which checks if reinfection is reduced wouldn't be concerned about other viral proteins because it's the spike we're concerned about with infection.


After posting, I probably should have asserted that this at least suggest that vaccines are not better than natural immunity- they are at least comparable, with the slight caveat that natural immunity may have a better ARR, or may not wane as suddenly as vaccinated.
I suppose if we want to get antagonistic, us natty folk can circle around the vaccinated and chant "one of us":
https://www.youtube.com/watch?v=mRe8J4scGtU
Yes, I'm not quite sure why he banned people. Do you know of how many people he banned?
I usually try to stay out of the drama since that enters into the whole social media side of this stuff. I did watch part of his livestream (I believe for Novavax and the FDA briefing) and there was a section in which he was describing his background. I suppose it's a point for many to attack him with because he was not trained in the US, so maybe that is part of it?
I tend to agree with natural immunity. The study at least indicates it lasts longer than the vaccine (slightly). I think the predictive model may be one to be careful of (protection 3 years on). I just wish we had more studies to come to better conclusions.
Ah I see! Honestly the moderators can be strange on all social media sites. It's somewhat a thankless job, and yet it's a role in which people may (whether intentionally or not) exert power onto others they may not normally have. Reddit is notorious for such a thing, as are some Moderators on Youtube. One generally hopes that the streamer would notice and respond to Moderators.
Considering it's not Dr. Mobeen himself, it does help a bit in his favor. Sometimes Streamers may have no idea what's going on, which can be unfortunate for such a situation as this. And honestly, I hope you wouldn't feel as if you need to censor yourself lest someone see such remarks. That may just enter into the realm of pettiness on the Moderator's behalf. But I suppose I should leave it at that.
Very interesting! When I read these kinds of studies, I always remind myself that PCR tests sometimes are false positive, giving something like 2% false positives. So if you test 1,000 people three times, you would get incidence of 60, or 6% or so, even if none of them had Covid.
This brings up a question that is actually burning in my mind: WHAT IS A REINFECTION?
For example, let's say that I, a previously infected unvaccinated individual, come in close contact with an ill person. Am I "reinfected" if I test positive some time later, despite having no symptoms?
The reason for my question is that last winter, my wife had Covid and I took care of her and did not get ill. After a week or so, I realized that on one recent evening I did feel slightly funny in my nose, which was such a fleeting feeling that it was possibly nothing at all.
But I always wonder, unfortunately without a definitive answer, what if that evening I did a PCR test on my nose and came up positive. Was I "reinfected"? It is a question to which I do not know the answer to, but it is very important for me and for all people.
My own answer, which is probably not perfect, is that a properly defined reinfection must at least involve symptoms such as fever and viremia and a reasonably low Ct threshold.
This study seems to define reinfection as a "positive PCR test", which always makes me wonder how many of those reinfections were not true illnesses.
For all intents and purposes, it appears as though reinfection and breakthrough are measured by PCR tests. The article from science considered breakthrough infections in some of the HCWs yet a good portion of them were asymptomatic- they only tested positive. And so in many cases asymptomatic infection tends to be included within the analyses.
There's a lot of variables when it comes to testing. As someone who used to do PCR testing I kind of saw how sensitive the tests were. It's generally why I avoid looking at case reports as some measure of what's going on. When you're told from the beginning that 40% of infections are asymptomatic, we should be cautious in assuming that all infections now (and reinfections) would be symptomatic in nature.
So we have to work within the parameters of the study, and generally look at these studies with some qualifier. Something along the lines of "reinfections are occurring [as confirmed through a positive PCR test]".
Thanks for highlighting this one, since at this point I reflexively avoid studies from Qatar because they're usually test-negative-controlled junk.
Note 1 on ARR is that a rational choice for the time-span is required. No time-span that doesn't include at least one full wave makes much sense. On the other hand a time-span that includes both a before and after-wave lull also might not make sense. But at the same time, waves are not alike, so the absolute risk reduction through one wave won't be the same through another, as in Alpha vs Delta (very few cases) vs Omicron for Qatar. This is really something that just needs to be scrutinized on a study-by-study basis. For example the CDC MMWR almost always selects stupid time spans.
Note 2 is that vaxxes almost certainly perform differently according to to-wave-injection-timing. So a low absolute risk reduction if injecting before a lull would probably look much better if injecting before a wave. Both the trials and the mass roll-out timed things unfavorably in this regard in most places (though Canada had a spring 2021 wave and so the timing was more favorable there).
Note 3 is that vax timing will probably never be perfect in practice. So you would want to look at natural immunity's durability through that lens - in practice, a lot of vax injections are going to give zero return on investment because of bad timing. Natural immunity doesn't seem to have this problem.
Alpha infection efficacy vs Omicron is interesting. I would think the Alpha wave had the most accurate distinction between infected and not due to better testing vs 2020 + higher case rate vs Delta. Maybe there is a bias for higher unrecorded 2020 infections in the control group (because they were less likely to be a positive in Alpha) and so the control group performed at a better-than-naive rate in Omicron. Don't know why that wouldn't be the same for Alpha vs Delta though...
You know Brian, thinking about it I probably jumped the shark in the inclusion of the ARR. So much for restraining myself. I should have remembered that the clinical trials were limited to 28 days, and so to do such a calculation was DEFINITELY improper.
I'm not sure with the Alpha portion. I suppose that would require sifting through prior Qatar data to figure out that factor. I was wondering about variants and cross reactive immunity, but I believe studies looking at neutralization or just RBD antibodies usually indicate that Beta is the variant that has the strange drop-off (unless I'm mixing it up with Alpha).
That sort of sounds more like the ancient Planas, et al study which compared post-Wuhan infection (at 12 months) and vax-based (at week 16) binding vs Beta / Alpha / Delta and generated mad headlines because no one ever knew that antibodies are meant to fade over time.
*edit OK actually this one is pretty directly on point https://www.nejm.org/doi/full/10.1056/NEJMc2119236 - all the VOC-convalescents do badly vs Omi, but I guess Beta the worst. However, a quick trip to Supplemental Table S1 shows that the Alpha were middle-aged, Beta almost all 80 year-olds, and Delta young adults. lol.
Oh yes, the biggest factor of all- old, withered B cells biasing the results! I kid, but seriously shouldn't we talk of immunosenescence a lot more than is already discussed? Not only are the elderly more susceptible, but they're the ones to least likely to be able to produce the antibodies and immune response necessary against a "novel" coronavirus.
And I don't think it's from just that study. It feels like all studies reported that Beta was the wonky variant, but again all of these studies were immunological shake and bake so there's already that problem.
Also, the Qatar study presents with a strange situation since they mention the number of international workers (which also tends to skew young- another hit for the ARR tangent), and I think you were alluding to that. So there's the dynamics of accuracy and consistency at play here.
This was an interesting slightly eye opening interview. Still trying to fathom, why such an enforced myopic solution? Israeli Vaccine Chief: We have made mistakes:
7.30 on: “I’m all for a nasal vaccine for example”…
….that would be able to better mimic the immunity we get from the disease”…..
(Re better mucosal protection apparently)
https://www.youtube.com/watch?v=bnMMYJKZvnU
It’s interesting that Novavax is supposed to also have epitopes as well as just the spike focus, although it’s probably out of date as not targeted to the current omicron I believe? Also there was a vaccine design with no spike, which we don’t talk about much, which apparently is looking to be a pan coronavirus vaccine, trying to copy what a healthy young immunity does re “memory B cells that bind SARS-CoV-2 and weakly cross-react with other coronaviruses”, again poss an epitope vaccine moving away from just the spike.
Thanks for the link ASmith.
So, what's interesting is that flu vaccines should have pointed us to the issues with an intramuscular vaccine. There's been plenty of questions as to whether influenza vaccines are not very effective because they are not introduced in a manner that follows the route of infection (i.e. intranasally). It's a bit ironic that a new vaccine vehicle was provided in the old manner, but there is the issue with mRNA and dispersion if provided intranasally.
Novavax supposedly has the spike protein studded on the surface of their carrier structure called an ISCOM. It'd be interesting because it's one of the only vaccines that would avoid your body needing your body to produce the spike, and so that makes one wonder if that would be considered safer.
https://moderndiscontent.substack.com/p/a-look-into-novavaxs-covid-vaccine
I would like to hear about that vaccine with no spike. I'm not sure how that would come to fruition, mainly because if one were to stop the virus from entering cells you would target it via the spike. It's the main paradox with the vaccine in which the cure (prophylactic) may be the disease in this scenario.
Thanks for the link re Novavax. Yes, the conclusion seems to be that a myopically targeted IM vax is not very good for this type of virus.
Novavax maybe better just re non mRNA and poss. PEG problems for some. As you mention it has still been flagged re myocarditis as they all are; I’d like to understand why that is. Also more about the spike? re: https://youtu.be/mbaQNKXh7qg
This is a link discussing a poss ‘pan coronavirus’ vaccine. The original link was moved when I shared it and the new link also had removed the statement which discussed healthy young immune response etc. being a clue for poss future vaccines. How well it would work I’m not sure, or if it will go anywhere?
https://medicalxpress.com/news/2021-05-vaccine-blocks-covid-variants-coronaviruses.html
There was also a study recommending perhaps an epitope vaccine, but that study was not well received shall we say, because it suggested problems with the spike, I think Merogenomics also did a vid looking at that.
Valneva was going to be produced in the UK, it’s supposed to be a traditional deactivated virus and adjuvant. However the UK said it wasn’t going ahead re the company broke contract, which they deny. The UK then said they wouldn’t have approved it anyway, but the reasons were not made clear. However since then we have a billion deal with Moderna. Apparently the mRNA hasn’t performed as well as its other maligned competitors, I need to find the info link where that was said, but we have high Gates influence in the UK press and MHRA.
There is talk now of nasal solutions as well, which has been presented before, apparently a while ago Israel even had one stating it helped prevent coronavirus by over 95%, but I’m not sure what happened to that, but others are now emerging. Even talk it will eventually be something you just buy over the counter? Everything seems to depend on influence of vested interests, rather than what might actually be better.
A friend of mine had an anti body positive test over a year and a half later, nearly two years with natural immunity. The question is what other aspects of immunity other than certain antibodies are happening via the current vaccines, as I believe you mentioned in another article?
Covid for me was 2 days achy, a week of a cold, but with less coughing than a prior respiratory virus and less nose blowing than a cold and two weeks feeling a bit more fatigued, no vax, so natural immunity.
I caught it from my partner who had 2xAZ, but won’t be having boosters. He unfortunately developed headaches which were of concern and long covid like symptoms and wasn’t quite himself for a few months. When he then got covid we treated him the second day with an early treatment protocol. He had flu like symptoms was a rough for 3-4 days and then after a week felt better, no major cough, but was fatigued for 2-3 weeks. However after that he then felt more like his old self, before the post vax problems, which seem to have resolved touch wood. He is also diabetic so more vulnerable category. I also added other recommended vits minerals , enzymes etc. which I also took. Our son had a cold for a week and mild dry cough, natural immunity.
We have so many studies out about the robustness of natural immunity, but like the one you mentioned it would be good to have more. Myself and son are in a natural immunity control group, monitoring general health of people and to see how often they get covid etc. Its trying to get approved recognition, so good luck to them with that!
It’s a coronavirus, even a souped-up one was always going to mutate and prob join all the other coronaviruses that circulate, I’m not sure the myopic presented ‘solution’ has made that any better, I would say worse…
Yes, I wrote another post a while after the Novavax one when the myocarditis concern was raised, suggesting that the spike protein is the main culprit. We sort of knew that, since studies came out indicating that the spike was cytotoxic, and so it really wouldn't make sense how the spike from the vaccine would be nontoxic but the one from the virus is, when they need to be antigenically similar in order to produce immunity against the virus.
https://moderndiscontent.substack.com/p/all-roads-lead-to-spike-protein?s=w
One of Joomi Kim's first Substack posts discussed the spike, and it's likely that the cytotoxicity of the spike wasn't recognized until the vaccines were in development.
https://joomi.substack.com/p/coming-soon
Thanks for the link. Honestly, articles such as that are frustrating because it feels like it takes forever for them to discuss what the article is about, and when they do is muddied from being surrounded by other ramblings.
I think this is the important part:
"The research team identified one particular receptor-binding domain site that is present on SARS-CoV-2, its circulating variants and SARS-related bat viruses that makes them highly vulnerable to cross-neutralizing antibodies. [...]
"Basically what we've done is take multiple copies of a small part of the coronavirus to make the body's immune system respond to it in a heightened way," Saunders said. "We found that not only did that increase the body's ability to inhibit the virus from causing infection, but it also targets this cross-reactive site of vulnerability on the spike protein more frequently. We think that's why this vaccine is effective against SARS-CoV-1, SARS-CoV-2 and at least four of its common variants, plus additional animal coronaviruses.""
And so they essentially looked for a region with conserved epitopes across different coronaviruses, rather than use the entire spike. This is interesting, however to what extent this region remains conserved is a predicament. I suppose it's something to look out for, and there may be still be questions if that conserved region is still bioactive (may still be cytotoxic).
Wow, I'm sorry he had to go through that. It's difficult, because given our situation we may have this slight inclination to see a situation and go "yes, it's the vaccines that are making it worse!" Or I'm at least speaking for myself at the moment. In reality, there could be so many factors as well and it's so hard to figure out the relevant information from all of the noise that's going on right now.
One of the biggest issues is that many of those natural immunity studies came out pre-Omicron, so we don't know anything about this current Omicron era. I think the findings of this study are important since it at least tells us that natural immunity may not be protective against Omicron, and that would at least explain the "blank slate" situation for many of us (not quite blank, but not sure what other phrase to use here). The problem now is that we need more studies like these, but it's likely that we won't be provided that possibility anymore.
The protocols so are likely to have done worse, mostly because it halted immune training for the entire world by telling us not to interact with others. For us adults, it may not be too bad since we have had years of immunological training through getting sick, but for children they missed out on two critical years of learning for their immune system. Ironic that children are behind in both school and their immune system. I wrote about this phenomenon which some scientists referred to as "immunity debt" and may explain why children are getting so sick, and with pretty serious symptoms.
https://moderndiscontent.substack.com/p/paying-back-the-immunity-debt
It's just another reason why we have screwed ourselves and younger generations with such a ridiculous global policy of lockdowns for a virus that apparently 40% of infected people present asymptomatic for.
I completely agree. Thank you for the detailed response, it’s much appreciated, as are all the critiques and in depth research around this. Yes, regarding immunity debt. However as yet, I’m not so forgiving either over the continued deliberate lies and abuse of power around this. Genuinely misguided, inept, corrupt or both…
Certainly we can be critical of those in power who continue to lie and pit us against each other, but we have to keep in mind what is important. We can criticize the vaccines, those in power, and all those factors but we should also make sure to remain rational when we look up the information.
There is also the other side:
https://www.pandemicdebate.com/post/covid-19-policy-israeli-immunologist-writes-open-letter-it-is-time-to-admit-failure
Thanks for the reply. Your answer does help some; I now better understand the limitations of the study (its narrow focus). So then, what role does the Innate system play in protection against reinfection? Or, is it that the Adaptive system will always dominate? Argh! I'm still so confused.
That's a nuanced answer as well. Generally speaking, the innate immune system is in charge of all types of infections. It's nonspecific, so it job is to target anything that doesn't seem quite right unlike the adaptive immune system which essentially plasters "Wanted" posters all around alerting the immune system what specifically to look for. I believe it's the innate immune system that actually leads to the hyper-inflammatory state in COVID (or at least plays a large role). There is also an idea that the innate system is actually trainable, although to the extent that trained immunity lasts I am not sure.
In general, both work together with the innate immune system indiscriminately killing things that should be there while the adaptive immune system selectively targets the virus. It's generally believe that the adaptive immune system helps to mount a quicker attack via recall. I think it makes it difficult because we usually consider them separate when they work in tandem.
And don't be worried about being confused! Honestly, all of this immunological stuff is new to me and so there's tons I either still don't know or will get wrong. The problem isn't the confusion, but understanding that this whole thing is a continuous process of learning. Try to overcome the confusion and learn to parse the information.
I'll also say, confusion is not a bad thing. Confusion tells you that you're dealing with a lot of information and trying to relate them together and making sense of all of the information. I think it's much better to be confused rather than to be obstinate. So really don't beat yourself up over being confused. I'd be surprised if you weren't! Just learn how to grow and move away from the confusion.
The more I learn the more confused I become. It was my understanding that the benefits of natural immunity over vax immunity was in the overall protection granted by natural infection (immune system interacting with all parts of the virus) compared to the highly specific (a particular protein of the virus) protection conferred by vaccination. {while noting that the benefit of vaccination over natural infection is in the risk reduction of severe outcome}
Now, is this no longer correct? Was this just an Immunology 101 myth? This paper, and your analysis, seems to suggest so. Unless I'm misunderstanding something, of course.
No, and apologies if I have confused you with this post. Naturally immunity certainly is broader (targets different proteins), but in the grand scheme of protection we have to look at the utility of targeting other proteins. In the case of a viral infection, the main concern is stopping the virus from interacting with our cells in the first place. The best way is to stop it from binding to our receptors, and in the case of SARS-COV2 that means targeting the spike. Both natural and vaccine-induced immunity hopefully leads to this end goal.
Now, it is true that other proteins will be targeted via naturally immunity. If we take the Nucleocapsid protein we know that we produce anti-N antibodies against this protein (it's how the CDC originally differentiated natural immunity from vaccine-induced immunity by looking for anti-N antibodies in blood sera).
However, what does the Nucleocapsid protein do? Well, the N-protein is responsible for winding up the viral RNA and making it more compact. Therefore the N-protein is sequestered within the virus.
This raises questions then- how would I target something that resides inside the virus? Our antibodies don't know it's there, and there's no way for the antibodies to squeeze into the virus to find those N-proteins. Because of this, the N-protein only makes itself known after a virion infects a cell, causes more N-proteins to be released as well as the N-protein that may explode outward if one of our cells lyse.
And that's the general issue. At the point that our immune system is made aware of the N-proteins the virus is likely on its way of undergoing massive replication. One of the only ways to target the protein is during viral replication, and if we target N-proteins that have spewed out of a cell that doesn't stop the actual virions from going to other cells and infecting them.
This is a long-winded response, but although we have broader immunity against other viral proteins the important factor is figuring out which ones stop the virus from infecting in the first place. That's why the N-protein is not the go-to protein to target, because it's not involved with infection like the spike protein is.
So hopefully that clears it up. A study such as this which checks if reinfection is reduced wouldn't be concerned about other viral proteins because it's the spike we're concerned about with infection.
Thanks for this detailed breakdown of the study! 👍🏽🌷