
COVID Vaccines and Parkinson's Disease Part IV
Can we glean anything from the autopsy case report?

This is likely to be the last post in this series on Parkinsonism. Here, I re-examined the autopsy report of the 76-year old man who collapsed weeks after his 3rd COVID vaccine, with the intent of finding anything fruitful that may point to a vaccine-related injury. In short, there’s still no evidence to help determine the source of the spike. However, the timing of the vaccines, as well as the worsening of Parkinson’s disease may be corroborated with evidence outlined in previous posts such as the one from yesterday. Thus, this article adds more context but still can’t provide exact answers to the autopsy report.
Hopefully the prior posts have provided additional context to the Parkinson’s/COVID paradigm.
However, what is yet to have been answered, or at least attempted to contextualize, is the case report from Mörz, M.1 of the 76-year old man with Parkinson’s who collapsed and died weeks after his 3rd dose of the COVID vaccine.
As noted in my first post from this series this case report has become a highly contested report, with some good and possibly bad-faith actors downplaying the possibility that this case report is related to the vaccines in some way.
Recently, Joomi Kim made a post in which she further evaluated Dr. Oliver’s remarks on the case report and with respect to Dr. Campbell’s video.
Although I didn’t intend to review some of Oliver’s remarks again, I think given the context of this post it’s worth rehashing a few points that may help with evaluating the case report. However, note that the intent of this post is not to argue the source of the spike, but instead to see if corroborating evidence may support that the vaccine may be related to the case report presented.
Spike in the brain a red herring?
Upon reviewing Oliver’s video again I looked at one remark when referring to a German study on the neuropathology2 in those who died of SARS-COV2.
Around the point of discussing the findings Oliver makes a remark that findings of spike protein in the brain were “incidental” to the severity of neuropathological changes.
I had problems with the term incidental- it suggests that the spike being there may not be pathological in some manner.
So what did the authors mean with the following phrase:
The presence of SARS-CoV-2 in the CNS was not associated with the severity of neuropathological changes.
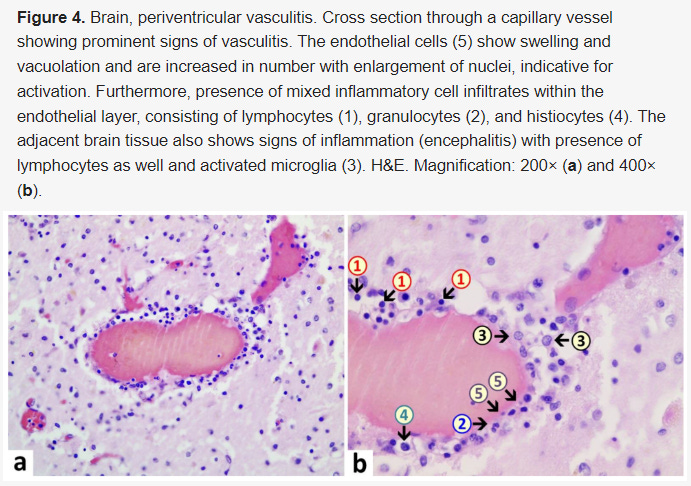
If we look at the results of PCR and immunohistochemistry staining there did appear to be viral proteins and RNA scattered in the brain of these patients, predominately being found in the brain stem (emphasis mine):
Samples from 40 (93%) patients underwent immunohistochemical staining for SARS-CoV-2 spike and nucleocapsid proteins. SARS-CoV-2-positive structures (cells and nerve fibres) were found scattered throughout the brain tissue. In eight (61%) of the 13 cases for which SARS-CoV-2 was detected in the brain by qRT-PCR, at least one SARS-CoV-2 protein could be detected (both spike and nucleocapsid in four cases, spike alone in three cases, and nucleocapsid alone in one case). Notably, in eight patients who were untested or tested negative on qRT-PCR analysis of SARS-CoV-2 RNA in the brain tissues, viral proteins were detectable by immunohistochemistry in the medulla oblongata (spike and nucleocapsid in one case, nucleocapsid alone in one case, and spike alone in six cases; figure 4). In the 16 (40%) cases positive for SARS-CoV-2 proteins on immunohistochemistry, spike protein was detected much more frequently (14 [88%] cases) than nucleocapsid protein (seven [44%] cases). By immunohistochemistry, SARS-CoV-2 could be mapped to isolated cells within the medulla oblongata and in the cranial nerves (either the glossopharyngeal or vagal nerves) originating from the brainstem (figure 5, appendix p 4). Overall, SARS-CoV-2 RNA or proteins were detected in the brain tissues of 21 (53%) of the 40 investigated patients, with eight (20%) patients having both SARS-CoV-2 RNA and protein detected (figure 4).
So maybe spike and other SARS-COV2 proteins may enter into the brain, refuting the argument in my previous post?
Not quite, since it didn’t appear that the presence of spike and nucleocapsid protein were directly involved with CNS damage. Again, it appears that the damage may be due to targeting of nearby cells and other cellular mechanisms such as microglial activation, with the inflammatory response likely causing the damage to various regions of the brain (emphasis mine):
The presence of SARS-CoV-2 RNA and proteins in the brains of patients with COVID-19 in this study is in line with the hypothesis that SARS-CoV-2 can infiltrate the CNS.14 However, the presence of SARS-CoV-2 was not associated with the severity of neuropathological changes. Thus, CNS damage and neurological symptoms might be due to additional factors such as cytokine storm, neuroimmune stimulation, and systemic SARS-CoV-2 infection, rather than by direct CNS damage caused by the virus. We saw a surprisingly uniform presentation of neuropathological findings (ie, activation of microglia, infiltration with CD8-positive T cells) in our patients, irrespective of the clinical severity of COVID-19 in each case. Notably, the neuropathological presentation in patients who died in a domestic setting or in a nursing home did not differ from that in patients who died in hospital wards or ICUs.
The researchers noted that microglial activation and astrogliosis (over production of astrocytes) were found in many of the tissue samples.
Thus, the presence of viral debris in the brain may not be due to direct invasion, but rather the targeting of the endothelium, with eventual loss of BBB integrity allowing the diffusion of spike protein, nucleocapsid protein, and viral RNA into the neighboring regions.3
This is important, because in some regards this may be a mischaracterization of the case series as reported by Oliver who used this case series as a way to suggest that detection of nucleocapsid in the brain does not infer much, when in reality the neuropathology of SARS-COV2 may not be derived from targeting the brain itself.
But this idea is also echoed in the heart study4 presented by both MedCram and Oliver which, again, suggests that the search for nucleocapsid proteins may be a red herring- the virus may not directly target these organs, but instead the pathology is secondary to peripheral endocytosis of spike.
Here’s from the discussion of the heart study (emphasis mine):
The focus of this study was to address a critical question on the common problem of cardiac disease in severe COVID-19: does the pathophysiology of the disease represent direct viral infection of the heart or the systemic manifestations of the cytokine storm and hypercoagulable propensity of the end stage disease state? This study strongly suggests that direct infection of the myocardium by SARS-CoV2 is not a factor in the pathophysiology of cardiac dysfunction. Although it is likely that the systemic manifestations of severe COVID-19 directly impact cardiac function, the primary and novel finding of this study is that there is substantial in situ expression of cytokines and complement activation in the heart secondary to endocytosis of circulating spike proteins by cardiac interstitial macrophages and pericytes which, in turn, induces a myocarditis.
I will contend that Oliver’s point that you don’t always find nucleocapsid in these regions is correct. However, it also doesn’t suggest that one can infer anything with respect to the virus or the vaccines being the source of the spike, and in many ways the search for viral proteins directly in the damaged region is probably not a worthwhile endeavor given these findings.
In regards to the case report
Apologies if the above seemed like a tangent. However, it does appear that the findings from Nuovo, et al,5 as well as the reports above note that direct viral infection is not a contributor to the various pathologies seen with SARS-COV2 or even possibly with the vaccines with respect to direct targeting of the spike to various organs and tissues.
However, when remarking about the Nuovo, et al. findings I was curious if there was evidence from the case report to corroborate the idea that spike does not get into the brain.
Here, the evidence doesn’t suggest that to be the case, but once again it may be argued that direct infiltration of the brain may be secondary to endothelial dysfunction and BBB permeability due to neuroinflammation.
And in fact, the findings from the autopsy report may corroborate this idea of secondary inflammation being related to the worsening Parkinson’s symptoms in this individual, as shown in the histology slides below:

And interestingly in these slides, which show a collection of activated cells around endothelia:
It’s important to remember that this individual was diagnosed with Parkinson’s prior to vaccination, and thus the presence of immune cells can’t be discerned between the spike or the progression of the disease.
Unfortunately, this evidence again doesn’t tell us much about the source of the spike.
However, I would argue that this evidence does, once again, support the findings from Nuovo, et al, and may in fact be suggestive of pathologies related to “the spike effect” even though the spike itself may not directly contribute to organ and tissue damage.
It’s possible that in this individual, the exacerbation of Parkinson’s disease was attributed to the neuroinflammation associated with endothelial dysfunction, and may at least suggest a possible route that led to the cause of death. It may be likely that only after severe damage to the BBB through neuroinflammation did the integrity deteriorate, allowing for spike to bypass the BBB. Again, presence of spike is not indicative of direct spike-related pathology.
Case reports of dyskinesia post-vaccination
Interestingly, several reports, albeit limited, exist with respect to vaccine injury in those with Parkinson’s disease that may provide additional context to the autopsy case report.
In one case series from Erro, et al.6 two people with previously diagnosed Parkinson's disease but no reports of dementia experienced severe dyskinesia after receiving BioNTech's mRNA vaccines.
Dyskinesia refers to a class of movements disorders in which one cannot control the movement of their body. They may be perceived as erratic, jerky movements. Dyskinesia can appear in those with Parkinson’s disease, although the presentation of dyskinesia is different than the typical movement issues seen with PD. In those with PD dyskinesia is generally be related to the medications prescribed, and therefore dosages of therapeutics may need to be altered in patients who present with dyskinesia in order to reduce these symptoms.
When looking at this case series one individual, a 61-year old woman with an 11 year history of PD, began experiencing severe, continuous dyskinesia hours after receiving her 1st dose of BioNTech’s vaccine. Her dosage of medications were decreased to see if this would reduce her dyskinesia, and eventually she was placed on a 75/18.75/200‐mg levodopa/carbidopa/entacapone regimen in contrast with her original 125/31.25/200 mg levodopa/carbidopa/entacapone dosage.
The levodopa increases dopamine serum levels while the other two drugs (carbidopa and entacapone) help maintain elevated levodopa levels.
The other woman, a 79-year old with a 5-year history of PD and occasional instances of peak-dose dyskinesia (dyskinesia that presents when levodopa levels reach their peak), presented with a fever, confusion, delusions, and severe dyskinesia a day after her second BioNTech vaccine. Although her fever disappeared after being prescribed aspirin her confusion and dyskinesia did not appear to return to baseline.
Although these results are rather alarming, there doesn’t appear to be any indication of dyskinesia in the autopsy case report from Mörz, M., with only a mere mention that the individual had worsening of motor symptoms and required a wheelchair. There also isn’t any mention of any alterations to his medications, which may have pointed to a possible indication of dyskinesia if provided evidence of such change in dosage.
The case report does mention that the deceased may have bit on his tongue at the point of his death, possibly due to an epileptic seizure:
Oral cavity: tongue bite was detected with bleeding under the tongue muscle (tongue bite is common with epileptic seizures).
And looking for more information I stumbled upon this review from Dulski, J., & Sławek, J.7 which also noted several cases of dyskinesia in those with PD who received COVID vaccines.
Unfortunately, I haven’t been able to access the actual article although the abstract mentioned the following (emphasis mine):
Five patients, with a mean age of 52, developed dyskinesia at a mean of 25 hours after receiving the COVID-19 mRNA vaccines. One patient had a history of neuropsychiatric symptoms and developed functional dyskinesia of the tongue. Four patients had a previous history of Parkinson's Disease (PD) with a mean duration of 10 years and developed dyskinesia and dystonia, which resolved (n = 2) or improved (n = 2) during the follow-up.
Dyskinesia of the tongue refers to involuntary tongue movements, although those with this form of dyskinesia generally present with their tongues sticking out more than other involuntary tongue movements.
It’s curious whether the deceased in the Mörz, M. case report may have experienced some form of dyskinesia of the tongue, which may have contributed to biting it when he collapsed, but again the ambiguity in the information doesn’t provide us much in being able to piece together these bits of information, again leaving me wanting of more context.
What spikes are being stained?
So far much hasn’t been elucidated with respect to the COVID vaccines in this one autopsy report and whether the spike found is spike from a viral infection or from the vaccines.
Regardless, the fact that SARS-COV2 infections may induce neuroinflammation may suggest an association with vaccine spike and the worsening of Parkinson-like symptoms in this one individual.
More interestingly, the findings of dyskinesia in those with PD who receive the COVID vaccines may point towards a catecholamine-related mechanism of adverse reactions.
But does this mean that there is no way of figuring out whether the individual may have died because of the vaccines?
Interestingly, there may be one thing that may help answer this question— what spike is being stained in these histology results?
Remember that the staining method for SARS-COV2 proteins rely on a method called immunohistochemical staining, or immunohistochemistry.
A bit of a mouthful, but this staining method relies on antibodies that can bind to viral proteins. Usually these antibodies are labeled, and thus when these antibodies are added to a tissue sample they bind to epitopes which match their antibodies and thus provide a color that can differentiate the antibody/antigen complex from other proteins.
Of course, this method is not without its issues as antibodies may bind to proteins other than the intended viral proteins and thus provide false positives. There’s also a degree of subjectivity and concerns over discerning background from actual results.
But the main crux of this topic is not really the color change but more to the point that immunohistochemistry relies on antibodies.
Thus, given what we’ve learned about antibodies we should be aware that different spike proteins may bind different antibodies. We were made aware of this with Omicron’s arrival and the loss of many monoclonal therapies in use since they no longer had the proper epitopes to bind.
This is also remarked upon in the article provided by Joomi Kim8 which looked at the reliability of immunohistochemical staining for various antibodies in use.
As noted, there are a ton of inconsistencies with the use of these staining methods. However, high sensitivity was found with the nucleocapsid protein whereas staining of the spike protein varied.
This was suggested to be due to the nucleocapsid protein remaining relatively conserved across variants while the spike, obviously, did not (emphasis mine):
Assessment of a wide range of commercially available anti-SARS-CoV-2 antibodies showed that only a subset can be reliably used in autopsy tissues (Figure 1, Supplementary Figure 3). Interestingly, anti- nucleocapsid-antibodies showed highest sensitivity. This may be since, of all SARS-CoV-2 proteins, nucleocapsid is produced at the highest levels during the SARS-CoV-2 lifecycle in cells.38 Of note, nucleocapsid-antibodies also performed well in detecting infected cells by the novel VOC Omicron B.1.1.529, while several anti-spike antibodies that detected SARS-CoV-2 WT spike protein failed to detect Omicron. The targeted epitopes of the nucleocapsid may be more structurally conserved and therefore result in more robust detection. Correspondingly, we found much less spike protein than nucleocapsid, based on both, the amount per cell and the general abundance in affected tissues. This should be considered when interpreting studies showing multiorgan tropism and target cell types, especially when using anti-spike-antibodies.1,2,33,39 In fact, in one study the unspecific nature of the used anti-spike antibody (our #3) was noticed between the preprint and the final publications5 and the erroneous interpretation could thus be corrected.
So just like monoclonal antibodies or our own adaptive immune system, the antibody must match the antigen presented.
But we’re also aware that the spike protein used in the vaccines were, up until the bivalent boosters, those of Wuhan spike.
We can take that information and thus look at the timing of the 3rd dose of vaccines in this case report (emphasis mine):
Already on the day of his first vaccination in May 2021 (ChAdOx1 nCov-19 vector vaccine), he experienced cardiovascular symptoms, which needed medical care and from which he recovered only slowly. After the second vaccination in July 2021 (BNT162b2 mRNA vaccine), the family recognized remarkable behavioral and psychological changes and a sudden onset of marked progression of his PD symptoms, which led to severe motor impairment and recurrent need for wheelchair support. He never fully recovered from this but still was again vaccinated in December 2021.
Thus, this individual received a 3rd dose of Wuhan-spike around the time that Omicron began to spread.
This raises a serious question: is the following a staining of Omicron spike or of Wuhan spike?

In arguing the differences between spike, we may raise the following assumptions:
Staining may only be effective for Wuhan spike, in which case if the above staining method stained the spikes presented can we infer that the spike found is Wuhan, and thus likely from the vaccine?
If the staining method is not effective against Omicron spike, then should we expect staining methods for spike to not show anything, and thus may be spike derived from an infection?
In answering this question I looked at which staining method was used by Mörz, M., which was a spike S1 antibody from the company ProSci. The review provided by Joomi didn’t appear to test for this antibody in particular, so it doesn’t provide any indication as to whether it lost binding affinity with Omicron.
However, the ProSci website does indicate that this stain may still bind to Omicron spike:
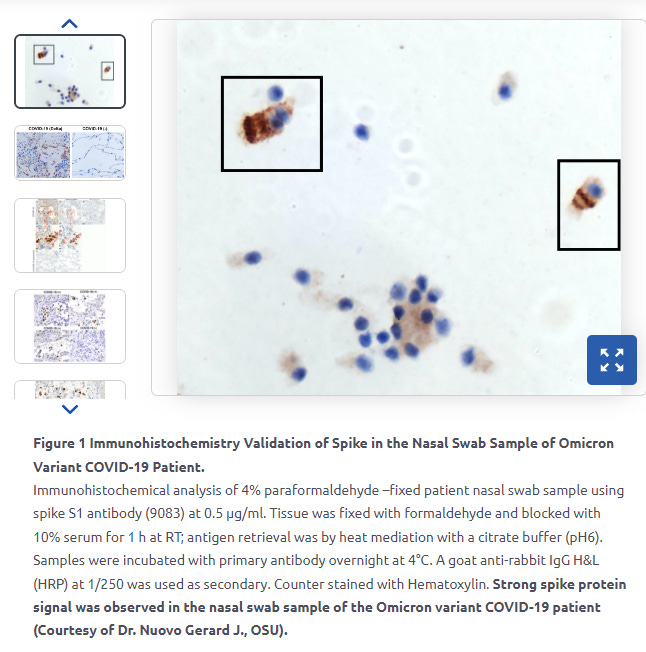
The person who provided this slide appears to be the same person who was the lead author on the Alzheimer’s CNS study reported yesterday.
This information would suggest that we may not, unfortunately, be able to discern between the two spikes in this case report when looking at immunohistochemical staining alone.
Of course, we don’t know if the spike proteins on ProSci’s website were confirmed Omicron with genomic sequencing. We also don’t know which variant, if it was the virus, the individual in the Mörz, M. would have been infected with.
But this does raise another avenue worth examining. Rather than focus on the search for nucleocapsid protein, why not identify which spike is shown in these histology slides?
It’s clear that the difference in spike should point towards a vaccine-related injury or a one of viral infection with more clarity than proximal assumptions with the search for nucleocapsid proteins.
In the search for vaccine-injury, it seems that the identification of spike would provide definitive answers towards a spike vaccine injury. Whether this type of research is actually occurring remains to be seen.
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Mörz M. (2022). A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines, 10(10), 1651. https://doi.org/10.3390/vaccines10101651
Matschke, J., Lütgehetmann, M., Hagel, C., Sperhake, J. P., Schröder, A. S., Edler, C., Mushumba, H., Fitzek, A., Allweiss, L., Dandri, M., Dottermusch, M., Heinemann, A., Pfefferle, S., Schwabenland, M., Sumner Magruder, D., Bonn, S., Prinz, M., Gerloff, C., Püschel, K., Krasemann, S., … Glatzel, M. (2020). Neuropathology of patients with COVID-19 in Germany: a post-mortem case series. The Lancet. Neurology, 19(11), 919–929. https://doi.org/10.1016/S1474-4422(20)30308-2
This argument is more substantiated by the findings from Nuovo, et al. and are not substantiated by the case series from Matschke, et al. However, the findings do appear to corroborate one another.
Mezache, L., Nuovo, G. J., Suster, D., Tili, E., Awad, H., Radwański, P. B., & Veeraraghavan, R. (2022). Histologic, viral, and molecular correlates of heart disease in fatal COVID-19. Annals of diagnostic pathology, 60, 151983. https://doi.org/10.1016/j.anndiagpath.2022.151983
Nuovo, G. J., Suster, D., Sawant, D., Mishra, A., Michaille, J. J., & Tili, E. (2022). The amplification of CNS damage in Alzheimer's disease due to SARS-CoV2 infection. Annals of diagnostic pathology, 61, 152057. https://doi.org/10.1016/j.anndiagpath.2022.152057
Erro, R., Buonomo, A. R., Barone, P., & Pellecchia, M. T. (2021). Severe Dyskinesia After Administration of SARS-CoV2 mRNA Vaccine in Parkinson's Disease. Movement disorders : official journal of the Movement Disorder Society, 36(10), 2219. https://doi.org/10.1002/mds.28772
Dulski, J., & Sławek, J. (2023). Incidence and characteristics of post-COVID-19 parkinsonism and dyskinesia related to COVID-19 vaccines. Neurologia i neurochirurgia polska, 57(1), 53–62. https://doi.org/10.5603/PJNNS.a2023.0011
Krasemann, S., Dittmayer, C., von Stillfried, S., Meinhardt, J., Heinrich, F., Hartmann, K., Pfefferle, S., Thies, E., von Manitius, R., Aschman, T. A. D., Radke, J., Osterloh, A., Schmid, S., Buhl, E. M., Ihlow, J., Dubois, F., Arnhold, V., Elezkurtaj, S., Horst, D., Hocke, A., … Glatzel, M. (2022). Assessing and improving the validity of COVID-19 autopsy studies - A multicentre approach to establish essential standards for immunohistochemical and ultrastructural analyses. EBioMedicine, 83, 104193. https://doi.org/10.1016/j.ebiom.2022.104193