
Addendum: zinc supplementation and copper deficiency
Additional preliminary notes on yesterday's zinc post as it relates to possible copper deficiency.

I received several questions on yesterday’s zinc post about the role of zinc supplementation and copper deficiency based on a sentence I included making such a reference.
I didn’t look into the matter too deeply at the time and left a comment based on a few remarks I found in the literature.
However, given that many people were curious I wanted to look into it a bit deeply and see what dynamics may be at play to cause this zinc supplementation/copper deficiency dynamics.
The primary protein of concern in this situation is called metallothionein.
As can be noticed by the thio metallothionein are small, cysteine-rich proteins that bind heavy metals such as zinc and copper. They are ubiquitous across eukaryotes as nearly every eukaryotic organism appears to use metallothionein. There are about 4 different isomers of metallothionein, with I and II being common among all cell types while III and IV are found in specialized cells.
The cysteine residues make up about 30% of the amino acids of this structure and are pivotal for interacting with metals.
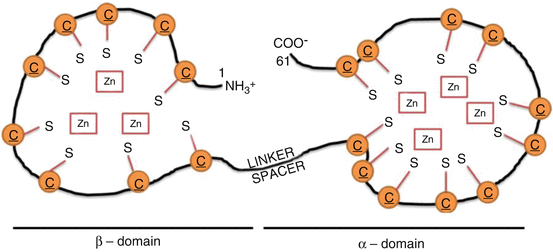
The binding of ions are based on the alpha and beta-domains of metallothionein which each carry different binding capacities (Dziegiel, et al.1):
The two metal-binding domains are separated by a non-cysteine-containing sequence often designated as the spacer or linker (Zangger et al. 2001; Babula et al. 2012). The α-domain consists of amino acids 31–68 and is located on the C-terminal edge, whereas the N-terminal β-domain contains amino acids 1–30 (Zangger et al. 2001; Dziegiel 2004). It has been demonstrated that the α-domain is capable of binding up to four, and the β-domain up to three, bivalent metal ions such as zinc, cadmium, mercury, or lead (Coyle et al. 2002b; Duncan et al. 2006).
One example of this interaction can be seen below for zinc:
The electronegative cysteine residues can interact with positively charged metal cations and may actually be pivotal in redox reactions as the cysteine residues and metal ions may exchange electrons during high levels of oxidation.
Some of these mechanisms can be seen below:

As such, metallothionein is critical for attenuating oxidative damage, and in fact reduced expression of metallothionein may be associated with chronic and severe diseases such as kidney disease, diabetes, and cardiovascular disease.
This chelating activity is also critical in detoxifying heavy metals such as lead and mercury as well.
For such a small protein, metallothionein is critical for our overall health.
Interestingly, metallothionein expression is regulated by zinc levels. Reduced metallothionein levels is associated with reduced levels of zinc, indicating an intrinsic relationship between heavy metals and metallothionein expression.
And that makes sense. Research suggests that metal ions, especially zinc, are responsible for inducing the expression and production of metallothionein I and II by binding to metal-regulatory transcription factor-1 (MTF-1), which then binds to DNA at the promoter region of metallothionein genes and leading to the downstream transcription and eventual synthesis of the protein.
Overall heavy metals, especially zinc, can upregulate the expression of metallothionein as a consequence of dealing with elevated metal levels; an excellent example of cellular feedback mechanisms.
So that brings us to the issue with copper deficiency in response to zinc supplementation.
Copper can also bind to metallothionein, however it appears that copper has a higher binding affinity than zinc for metallothionein, and so even in times of high levels of zinc copper may be chelated as a consequence of elevated metallothionein levels.
The flow of biochemical processes are as follows:
Routine supplementation of zinc increases serum levels.
Circulating zinc may be taken into cells where it can bind to MTF-1 and activate it.
Activated MTF-1 can then bind to the promoter region of metallothionein genes, leading to transcription and then translation of the proteins.
Metallothionein can now scavenge for zinc.
However, metallothionein can also inadvertently bind copper which appears to have higher affinity than zinc for metallothionein.
Circulating copper levels consequently decrease leading to copper deficiency, and long-term copper deficiency may lead to diseases such as anaemia2 and neutropenia,3 along with possible neurological issues.
This is a very loose examination, but here we outlined one possible mechanism responsible for copper deficiency as a consequence of long-term zinc supplementation.
Note that many supplements may use levels of zinc higher than is recommended for daily intake, and so care must be taken for those who taken zinc for extended periods.
Several studies that look at copper deficiency as a consequence of zinc may use measures of zinc above 100 mg, and many zinc supplements may hover around 30-100 mg per serving.
Similar to excessive zinc, be careful in understanding whether prolonged use of zinc may be related to copper deficiency by noting physiological and neurological changes. Also, it’s always good advice to consult medical professionals.
Copper, therefore may be something worth considering with zinc supplementation in order to overcome the copper chelation by metallothionein. However, note that the evidence here has been qualitative, such that no recommended doses for either are provided due to the complexities of pharmacokinetics and bioavailability of these ions (also I’m not a medical professional). Make sure to understand what copper doses would be adequate given the zinc doses. Also, consider whether both would be necessary in the first place or whether it may be overdoing it by excessive supplementation.
So hopefully this helps shed some light on the mechanisms of copper deficiency. It’s always important to be mindful of the things we take, whether medications or supplementation. Sometimes more may not always be better.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Dziegiel, P., Pula, B., Kobierzycki, C., Stasiolek, M., Podhorska-Okolow, M. (2016). Metallothioneins: Structure and Functions. In: Metallothioneins in Normal and Cancer Cells. Advances in Anatomy, Embryology and Cell Biology, vol 218. Springer, Cham. https://doi.org/10.1007/978-3-319-27472-0_2
*As a note, I have drawn nearly all of the information from this article from this reference.
Anaemia is reduced hemoglobin levels and the inability to properly transport oxygen. People who have anaemia may feel tired and fatigued.
Neutropenia is reduced levels of neutrophil.
Thanks for both these. I was going to say something related to copper yesterday, but the day got away from me.
Yes to supplementation if you have a copper poor diet. BTW, tofu and beans is a good source
For a list of foods
https://www.copperh2o.com/blogs/blog/ultimate-guide-to-foods-with-copper