


Vaccination in 5-11 Year Old Children During Omicron
A quick look at the risk/benefits of vaccinations in Singaporean children, and the incessant need to vaccinate in general.

Note: I forget to do this often, but please remember that this information is intended to be informative, not prescriptive, so do not use this information as a validation for your medical options. Please consult doctors and medical professionals for information and suggestions.
With concerns over children and COVID vaccination, we must always look at the balance between safety and efficacy to see whether the benefits outweigh the risks.
Yesterday, a paper was published within the New England Journal of Medicine (NEJM) which measured positive rates, hospitalizations, and adverse reactions in children who received Pfizer’s COVID vaccine.
Dr. John Campbell covered this study in his YouTube video published today:
The paper in question is the following one from Tan, et. al.1

This study doesn’t differ from ones seen in prior clinical studies, and so we won’t look too deeply into the data aside from the concerning points, including whether the vaccines were effective during the Omicron wave and the level of adverse reactions that took place.
Study Introduction
Singapore began allowing children under the age of 12 to be vaccinated at the end of December 2021, yet vaccines were considered voluntary:
Schools were open with the use of masks mandated, but children younger than 12 years of age were not subject to measures that restricted adults who were not fully vaccinated from entering selected venues. In Singapore, the vaccination of children 5 to 11 years of age with two 10-μg doses of BNT162b2 administered at least 21 days apart commenced on December 27, 2021, starting first with older children (9 to 11 years of age) and then with children 5 to 8 years of age 2 weeks later. Vaccination is voluntary in Singapore, and parental consent is required.
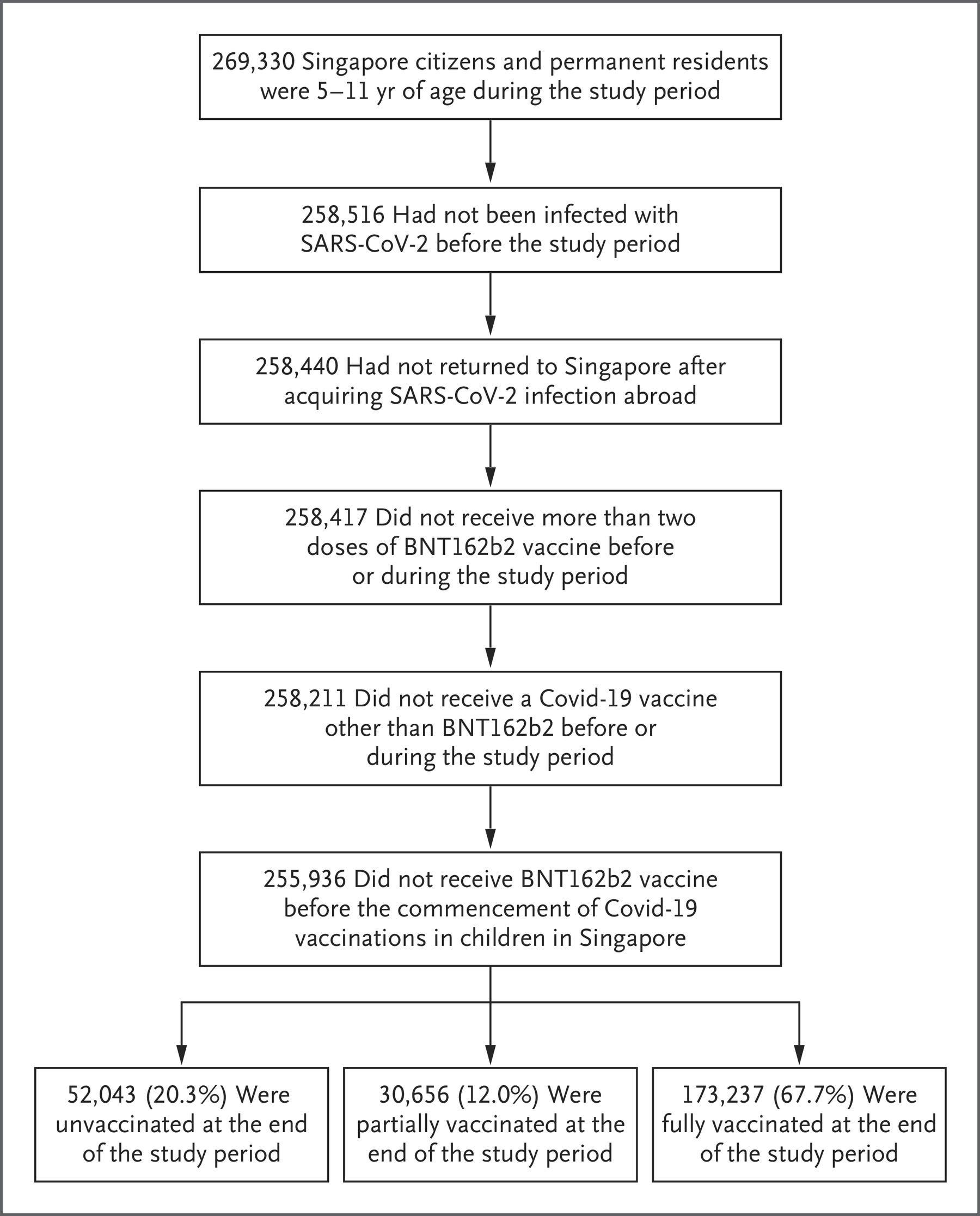
The study took place from January 21, 2022 until April 8, 2022. The study excluded anyone who was previously infected with COVID or were vaccinated before the starting point. The study population can be seen in the chart below.
Rates of positivity were measured with both antigen and PCR tests, with PCR tests being used to validate more severe symptoms. What’s important for this section is how hospitalization was measured (emphasis mine):
We analyzed the incidences of all reported SARS-CoV-2 infections (positive on PCR, rapid antigen testing, or both) and PCR-confirmed infections, which serve as a proxy for increased severity of illness. To examine the effect of vaccines on more severe illness, we analyzed the incidence of hospitalization for Covid-19. During the omicron outbreak, admission to hospitals was based on clinical indications of symptomatic SARS-CoV-2 infection in clinically unwell children, including but not limited to severe pneumonia and multisystem inflammatory syndrome in children (MIS-C). The onset of severe illness for which hospitalization was warranted was defined as the date of confirmed infection. Because of the time lag between SARS-CoV-2 infection and hospitalization and the potential risk of excluding patients in whom infection developed during the study period but who were hospitalized after the study period, we restricted the hospitalization analysis to patients who were notified of confirmed infection up to and including April 1, 2022 (i.e., 7 days before the end of the study period).
So severe pneumonia and MIS-C were some of the symptoms used as indicators of severe illness and hospitalization. This will be important when we compare measures.
Results
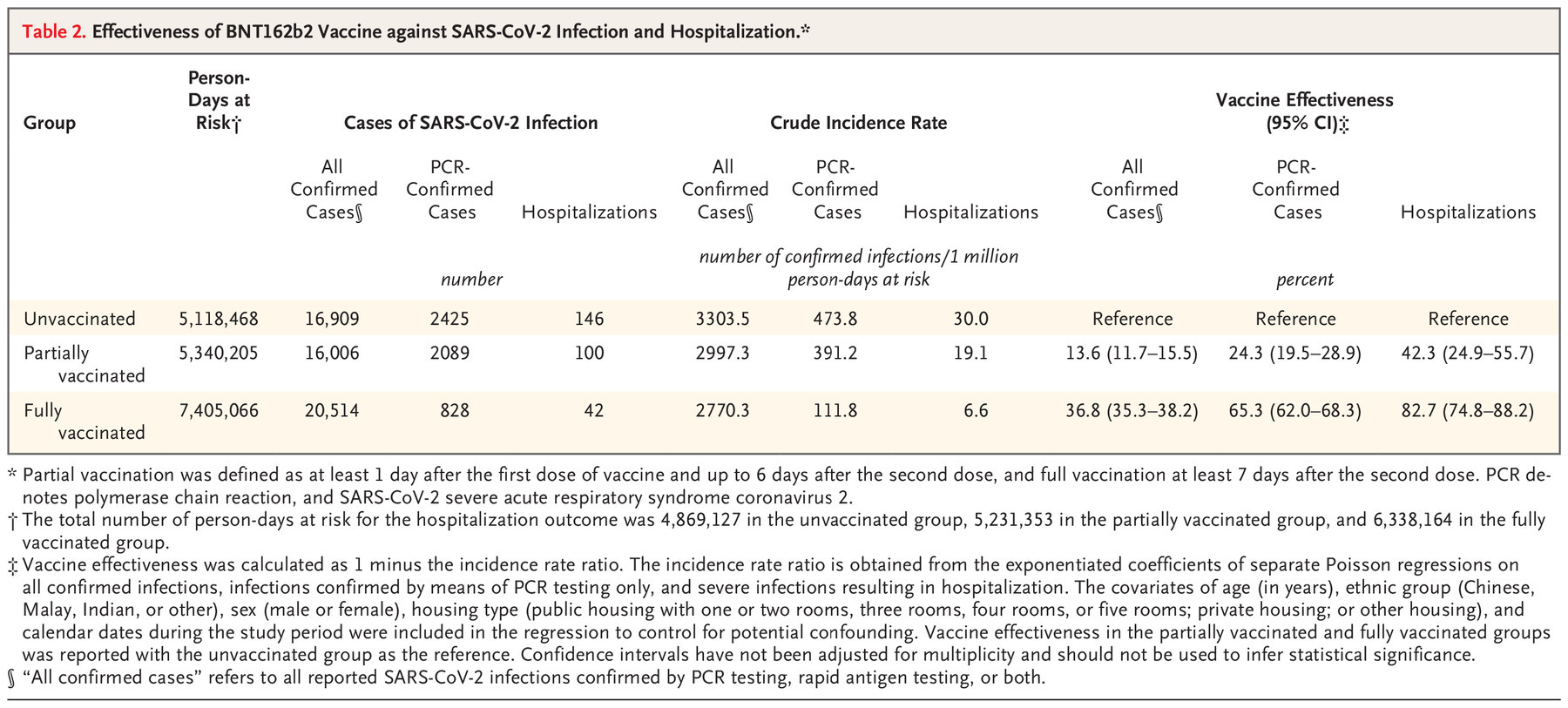
So we won’t dive too deeply into this portion. It’s the same information we tend to get with these types of studies which generally provide relative risk reduction rather than absolute risk reduction.
And, as is typical of Omicron infections, there generally doesn’t appear to be robust protection from infection, but “protects” against severe infection. However, protection from infection is something that is well-known by now.
So just on these metrics alone, we can find the typical messaging that vaccination may not protect against infection, but it may reduce severe illness. We’ll discuss the latter argument a bit further on later.
But just to have a little fun with the data, I decided to do some ARR calculations. This won’t be comparable to the values above because their vaccine effectiveness calculations were based on Poisson regressions, which take into account several variables such as age, sex, and socio-economic status.
Instead, we can calculate a separate RRR value based on the population data and the hospitalization information above (you can refer to my prior post on RRR vs ARR for help). We know that 52,043 children were unvaccinated at the end of the study and 173,237 children were fully vaccinated.
Using the corresponding hospitalization rates of 42 and 146, respectively, we can get an RRR value around 91.36% vaccine efficacy against hospitalization.
Again, remember that we are taking several liberties with this information (including when children were considered fully vaccinated, as well as all of the demographic variables that were controlled for), so our percentage is skewed higher. However, in such a case it’s important that when the information isn’t exactly accurate, it at least remains consistent.
Using the same data, we can calculate the ARR, which comes out to about 0.2562% efficacy against hospitalization.
Remember that RRR is a measure at the point of exposure- if a child becomes exposed, how protected would they be from infection and hospitalization. ARR takes into account the odds a child would become exposed in the first place. Thus, ARR tells us how likely a child may be exposed, infected, and if they may require hospitalization, all of which appear to be low numbers already.
These numbers are important because the current messaging argues that hospitalization and severity of illness are reasons to vaccinate2. Therefore, we should expect the data to substantiate such a position, and in such a case it’s hard to argue that to be the case given these numbers.
But if these numbers don’t provide much convincing, there appeared to be 5 children requiring supplemental oxygen during the time of this study. What’s even more egregious is that only 1 child was unvaccinated while 2 were partially vaccinated and the other 2 were fully vaccinated:
Among hospitalized children, only five received supplemental oxygen, four of whom were admitted to the intensive care unit. Of these five children, one was unvaccinated, two were partially vaccinated, and two were fully vaccinated. No deaths attributable to Covid-19 (as determined by the cause of death reported to the Ministry of Health) were observed during the study period.
So 4 of the 5 children were vaccinated, yet still required supplemental oxygen. There could be many reasons why these children required it in particular. It could be that these vaccinated children were already severely immunocompromised, and thus vaccination was considered an option for more “protection” even though they were likely to suffer severe illness regardless.
However, this does raise questions as to how “protective” these vaccines are from severe infection given the lack of information and evidence.
Adverse reactions
So with questionable effectiveness out of the way, we should look into the safety profile of these vaccines for these children.
Unfortunately, there only appears to be this little comment in the discussion section:
In Singapore, 22 serious adverse events after vaccination (0.005% of all doses administered) among children 5 to 11 years of age were reported to the Health Sciences Authority as of February 28, 2022.20
Now, we don’t know how many of these children were included in the above study, but based on the percentage of total doses administered that appears to be 22 adverse events out of 440,000 vaccine doses within the given age group. It’s difficult to compare this data to the above study anyways since vaccinations for those age 8-11 started at the end of December, while this study wasn’t conducted until the Omicron era.
However, all adverse reactions should be considered very concerning. The study didn’t explain what “serious” entailed, but the study links to this government document which provides the following footnote:
An adverse event is classified as serious when the event resulted in hospitalisation/extended stay in hospital, resulted in a significant reduction in functioning level/disability, resulted in a life-threatening illness (e.g. anaphylaxis) or death, resulted in birth defects or is a medically important event.
So we can assume that a serious adverse event would possibly require hospitalization, and considering that this data is a few months behind from the above study there are likely to be several more unreported adverse events at the time the Tan, et. al. study was completed.
Remember, this data isn’t quite comparable to the data within this study due to the difference in timeframes. The researchers also did not mention the level of adverse events in their own study, so there’s nothing to use as a reference.
Regardless, this once again raises questions as to the actual safety profile of these vaccines, and the actual risk of continuously enforcing vaccination on the young.
The Incessant need to Vaccinate
With Ba.4/Ba.5 on the rise there continues to be a greater push for vaccination. With school returning in a month we may see more messaging that enforces children be vaccinated.
The need to vaccinate must always operate under the factors of safety/efficacy, as well as the risk/benefit paradigm. Here, there just doesn’t appear to be strong evidence to support the need to vaccinate (at least in my opinion).
In general, children are considered to be the least likely to need hospitalization- the data within this study points towards that argument as well. And yet there continues to be this large need to vaccinate children.
Just as an example for how well children do with COVID, I tried looking up how many children have died from Omicron in Singapore. There appears to be this article released just today in Singapore’s todayonline.com, which raises questions as to the timing of this article in particular- but that’s a different concern for now.

Singapore probably has one of the lowest deaths in the world, with only about 1,400 recorded deaths so far, including none in children- until a few weeks ago (allegedly, but not substantiated):
On June 27, an 18-month-old boy became the first patient below the age of 12 to die from Covid-19. The cause of death was encephalitis (inflammation of the brain) due to Covid-19, as well as viral infections caused by the respiratory syncytial virus and enterovirus.
Then last Sunday, a four-year-old girl who contracted Covid-19 died from pneumonia. Like the boy, she was previously well and had no past medical history, the Ministry of Health (MOH) said.
The wording here is pretty misleading. The “cause of death” being due to COVID-19 means that, well, COVID would be the cause.
However, one of the doctors interviewed in this article actually rebukes COVID as the cause in both instances:
In the case of the boy, the infection by the respiratory syncytial virus and the Covid-19 virus may have been incidental.
As for the four-year-old girl, he [Professor Paul Tambyah, president of the Asia Pacific Society of Clinical Microbiology and Infection- taken from the article] said that he did not have the full details of her case and symptoms, but noted that there were reports in the media about her vomiting and frothing at the mouth when she collapsed.
This suggests that she might also have had a brain inflammation, which has been reported in children with viral infections in the past.
Prof Tambyah added that deaths from pneumonia due to Covid-19 is extremely rare, especially among children.
And so these two cases may be tied to other viral infections (the infant appeared to have a coinfection with RSV).
All throughout the article there were mentions that other factors are likely to blame for the deaths, and considering that no deaths in children have occurred so far it doesn’t seem to be likely starting now with Omicron (although more evidence would be needed to substantiate the claim).
So Singapore, with no recorded deaths in children from COVID, appear to be vaccinating their children with vaccines of unknown safety.
So it makes this point rather moot in the Tan, et. al. discussion, given that the risks have always been low to begin with:
Our findings indicate the protective effect of vaccination against infection and severe illness. We found that the vaccine effectiveness against hospitalization was higher with full vaccination with two doses of BNT162b2 (82.7%) than with partial vaccination with one dose (42.3%).
And there’s also this little bit of information about infectivity:
Beyond the short-term and long-term health risks of SARS-CoV-2 infection in children (including MIS-C21 and “long Covid”22), high infection rates among children may lead to transmission to older adults23 and may increase the risk of overwhelming existing health care capabilities during the omicron wave. It appears that these risks can be mitigated by the vaccination of children.
So there’s an argument here that children should be vaccinated in order to reduce spreading the infection to others (similar messaging we’ve seen before).
Except there’s plenty of evidence now that proves the contrary, including Dr. Fauci himself admitting that the vaccines don’t reduce infection.

And this is even substantiated by the researchers own data, which shows a huge drop in protection against infection the further out from the second dose one goes:

In short:
the vaccines don’t stop infection
the risk of severe illness is very low in children to begin with, and
there are concerns about the risks of adverse events, especially in children
And yet vaccinations of children continues on, regardless of the issues raised in the above bullet points.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Cohen-Stavi, C. J., Magen, O., Barda, N., Yaron, S., Peretz, A., Netzer, D., Giaquinto, C., Judd, A., Leibovici, L., Hernán, M. A., Lipsitch, M., Reis, B. Y., Balicer, R. D., & Dagan, N. (2022). BNT162b2 Vaccine Effectiveness against Omicron in Children 5 to 11 Years of Age. The New England journal of medicine, 387(3), 227–236. https://doi.org/10.1056/NEJMoa2205011
I originally conducted ARR and RRR values looking solely at the positive rates and comparing it to hospitalization, but I wasn’t sure how proper of a calculation that would be, and therefore decided to remove it since so many liberties have already been taken with the data. However, if anyone was curious, I got an ARR of 0.6587% and an RRR of 76.29%.
So Dr Campbell says "the risk benefit analysis has dramatically changed" lol.
I haven't seen ARR of the "benefit" of the jabs preventing/reducing severe analysis before this, but now we see the man behind the curtain. Thank you so much for providing the RRR and the ARR from this study. ARR of a quarter of one percent! I never believed the mantra of "protection from severe illness and hospitalization" Grauchi et al promoted, plus 4 of 5 needing oxygen were vaccinated! and now I see that house of cards fallen down. Lies, lies and damned lies all along.
Again, thanks for this review and analysis