
Study notes high rates of Gastrointestinal Adverse Events in those taking GLP-1 RAs
Evidence continues to mount that this class of drugs may not be as "safe and effective" as initially thought.

In following a post earlier in the week noting ileus, or intestinal paralysis, being included in the FDA’s label for Ozempic, a recent study published in JAMA1 seems to provide further evidence that these highly popularized and sought after drugs may not be as safe as they appear to be.

Published Thursday, the study looked at a random sampling of over 16 million patients between the years 2006 and 2020 for their use of GLP-1 RAs Semaglutide or Liraglutide and compared incident rates to those of a comparator drug bupropion-naltrexone (brand name Contrave) which has been used for weight-loss for several years.
Because of the timeframe in which the study was conducted researchers limited their inclusion criteria to those who both did not have diabetes and also were not taking anti-diabetes medications, while also having evidence of obesity up until inclusion into the study:
We used a random sample of 16 million patients (2006-2020) from the PharMetrics Plus database (IQVIA), a large health claims database that captures 93% of all outpatient prescriptions and physician diagnoses in the US through the International Classification of Diseases, Ninth Revision (ICD-9) or ICD-10. In our cohort study, we included new users of semaglutide or liraglutide, 2 main GLP-1 agonists, and the active comparator bupropion-naltrexone, a weight loss agent unrelated to GLP-1 agonists. Because semaglutide was marketed for weight loss after the study period (2021), we ensured all GLP-1 agonist and bupropion-naltrexone users had an obesity code in the 90 days prior or up to 30 days after cohort entry, excluding those with a diabetes or antidiabetic drug code.
For those curious Contrave is an oral therapy comprised of Bupropion (aka Wellbutrin), which exerts its effect by inhibiting the reuptake of neurotransmitters such as dopamine and norepinephrine. There are a few other effects on the CNS as well, but the general intent is that bupropion eventually leads to appetite suppression.
Naltrexone (brand name Revia) is an opioid antagonist and has generally been used for those dealing with alcohol and opioid dependency. It’s alleged that blocking of opioid receptors reduces the euphoric effects of opioids such as heroin, and hopefully results in reductions in opioid dependency. The use of Naltrexone for obesity appears to relate to its dampening of reward systems in the brain- use of Naltrexone is argued to reduce food cravings because it reduces the pleasurable, reward feelings one may get from eating.2
Patient data was measured from time of first use of a drug up until any reported incident:
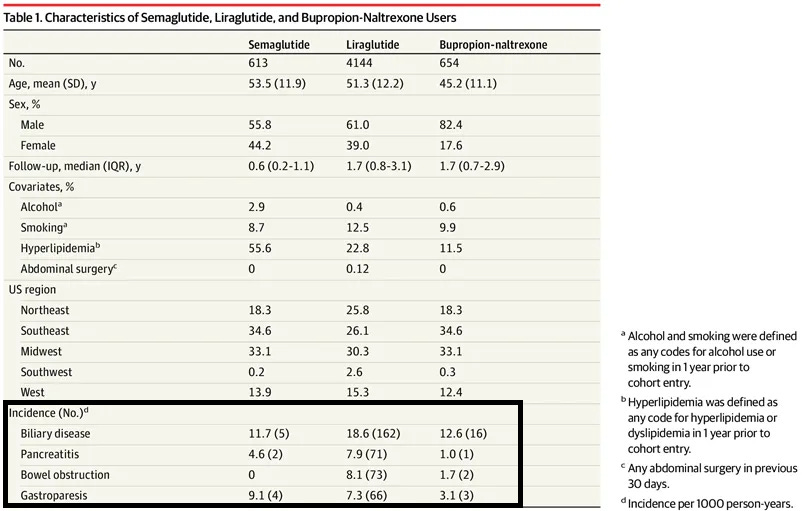
Patients were observed from first prescription of a study drug to first mutually exclusive incidence (defined as first ICD-9 or ICD-10 code) of biliary disease (including cholecystitis, cholelithiasis, and choledocholithiasis), pancreatitis (including gallstone pancreatitis), bowel obstruction, or gastroparesis (defined as use of a code or a promotility agent). They were followed up to the end of the study period (June 2020) or censored during a switch.
Note that matching didn’t appear to occur in this study. Patients within the Bupropion/Naltrexone group were predominately male. Patients within the Semaglutide group also had higher rates of hyperlipidemia, although the researchers conducted a sensitivity analysis excluding this variable in order to see if it played a role in the outcomes.
The final number of patients included 4144 Liraglutide, 613 Semaglutide, and 654 Bupropion/Naltrexone users.
When comparing incident rates based on incidents in patient groups there appeared to be elevated rates of pancreatitis and gastroparesis among GLP-1 RA users. Note that biliary disease appeared to be slightly lower in Semaglutide users when compared to Bupropion/Naltrexone users. There also didn’t appear to be any incidences of bowel obstruction among the Semaglutide group included, with the Liraglutide group showing the highest incidence rate of bowel obstruction:
When comparing hazard ratios, with Buproprion/Naltrexone acting as a comparator reference, there was notably increased risk of an incident with respect to use of GLP-1 RAs relative to Buproprion/Naltrexone even when hyperlipidemia was excluded:

Note that the hazard ratio used above collected GLP-1 RAs together, and so different risks between Semaglutide and Liraglutide will be masked. This is an issue given that Hyperlipidemia occurred in more than half of all Semaglutide patients who had an incident. Bowel obstruction appears to occur predominately within the Liraglutide group as well. Keep in mind that, although both Semaglutide and Liraglutide operate as GLP-1 RAs, minor molecular differences may lead to other, more nuanced differences between the two drugs which need to be considered within the context of adverse reactions.
Note also that the use of Bupropion/Naltrexone as a comparator control means that the hazard ratios calculated are relative to incidence rate of those taking another medication, and therefore doesn’t provide any background comparison for people who may be obese but not taking any medications.
The patient information also doesn’t provide any time from first use of medication to first incident. Because of the possible long-term use of GLP-1 RAs for weight loss there should be a considerable concern over prolonged use of these drugs and increased risk of adverse reactions. There also isn’t any information on dosage (Semaglutide may refer to different doses, with Wegovy having the highest dose of Semaglutide) which we may argue may correlate with increased risk of adverse reactions. Lack of BMI data for patients is also a problem. BMI assumptions appear to have been done based on patient codes that infer an obese BMI. It would be interesting to consider if BMI differences were noticeable across the groups.
Overall, I take this study more as a point of interest. It suggests that there may be more things going on than nebulous announcements that these GLP-1 RAs are “safe and effective”. It warrants further investigations, especially as interest in these drugs continue to grow.
Note that, although the risk of these adverse reactions are considered rare, the risk will likely occur in a larger population the more people take these medications. It warrants understanding who may be at risk, and why it’s necessary to do research into the things we put into our bodies.
Or maybe, it’s another reminder that we should take the old-fashioned way in losing weight before turning to medications.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Sodhi, M., Rezaeianzadeh, R., Kezouh, A., & Etminan, M. (2023). Risk of Gastrointestinal Adverse Events Associated With Glucagon-Like Peptide-1 Receptor Agonists for Weight Loss. JAMA, e2319574. Advance online publication. https://doi.org/10.1001/jama.2023.19574
Tek C. (2016). Naltrexone HCI/bupropion HCI for chronic weight management in obese adults: patient selection and perspectives. Patient preference and adherence, 10, 751–759. https://doi.org/10.2147/PPA.S84778
"Or maybe, it’s another reminder that we should take the old-fashioned way in losing weight before turning to medications."
Thanks for the reminder. The oldest of all is to eat real food (dating back to when there wasn't anything else), if it can still be found. Or maybe I should say while it can be found.
I recently saw a video of doctors discussing drugs like Ozempic. One stated that the patient will have to be on the medication for life if they do not change their lifestyle. If they don't change their lifestyle and go off the medication, they will gain back all the weight loss and then some.
I thought, if they could change their lifestyle then they wouldn't need the medication in the first place. I lost weight effortlessly by cutting grains, sugar, and processed foods. My mood is better, and I sleep better too. Mainly I eat what I'm told I shouldn't eat; meat, eggs, high fat dairy. Low carb veggies and fruits, and fish. I rarely exercised, though I do now. People need to stop listening to the bad advice from the government (who is in bed with big pharma) and doctors that have no nutritional training (I suppose many of them are in bed with big pharma too).