


Pfizer Releases an Interim Report on their COVID Therapeutic (Brief Review)
What does the preliminary data indicate?

Surprise, surprise, but right on the heels of Molnupiravir receiving approval for use in the UK, Pfizer reported phenomenal interim data according to their Phase 2/3 trials of their protease inhibitor named PAXLOVID.

If you want to find my previous breakdown of Merck’s clinical trials, you can check it out here. It seems like some of the same issues have arisen in this study (deaths in the placebo group??), so I won’t reiterate them. Instead, I’ll note some differences between Merck’s and Pfizer’s trials here. I’ll also examine PAXLOVID’s mechanism of action and indicate how this compares to Ivermectin as it is considered a highly controversial drug.
Pfizer’s Clinical Data
The name of Pfizer’s Phase II/III trial is EPIC-SR (Evaluation of Protease Inhibition for COVID-19 in Standard-Risk Patients) and EPIC-PEP (Evaluation of Protease Inhibition for COVID-19 in Post-Exposure Prophylaxis) – it’s a mouthful, but they’re essentially examining PAXLOVID’s effectiveness in treating COVID in the former while examining its prophylactic nature in the latter.
Here’s information about the study taken from Pfizer’s Press Release (emphasis mine):
The primary analysis of the interim data set evaluated data from 1219 adults who were enrolled by September 29, 2021. At the time of the decision to stop recruiting patients, enrollment was at 70% of the 3,000 planned patients from clinical trial sites across North and South America, Europe, Africa, and Asia, with 45% of patients located in the United States. Enrolled individuals had a laboratory-confirmed diagnosis of SARS-CoV-2 infection within a five-day period with mild to moderate symptoms and were required to have at least one characteristic or underlying medical condition associated with an increased risk of developing severe illness from COVID-19. Each patient was randomized (1:1) to receive PAXLOVID™ or placebo orally every 12 hours for five days.
Once again, this is an interim report, and so not all of the data is accounted for just yet. Luckily, this study has more participants (almost 500 more participants when comparing interim data) compared to Merck’s, so it’s a better level of data.
Let’s see some more of it (emphasis mine):
The scheduled interim analysis showed an 89% reduction in risk of COVID-19-related hospitalization or death from any cause compared to placebo in patients treated within three days of symptom onset (primary endpoint); 0.8% of patients who received PAXLOVID™ were hospitalized through Day 28 following randomization (3/389 hospitalized with no deaths), compared to 7.0% of patients who received placebo and were hospitalized or died (27/385 hospitalized with 7 subsequent deaths). The statistical significance of these results was high (p<0.0001). Similar reductions in COVID-19-related hospitalization or death were observed in patients treated within five days of symptom onset; 1.0% of patients who received PAXLOVID™ were hospitalized through Day 28 following randomization (6/607 hospitalized, with no deaths), compared to 6.7% of patients who received a placebo (41/612 hospitalized with 10 subsequent deaths), with high statistical significance (p<0.0001). In the overall study population through Day 28, no deaths were reported in patients who received PAXLOVID™ as compared to 10 (1.6%) deaths in patients who received placebo.
I won’t comment on the concerning deaths (look at my Merck newsletter for that), and will instead compare the effectiveness. From what is presented, this is actually phenomenal data, far better than Molnupiravir’s which was reported to only cut hospitalizations/deaths in half compared to PAXLOVID’s 89% reduction. Reminder to take this data with a grain of salt; no demographic data was released, and until all of the data is released we won’t be able to fully compare the results. Nonetheless, this seems very good, and unlike Molnupiravir there shouldn’t be any concerns about mutagenicity.
Hopefully more data will be released about these trials, but this does sound like very good preliminary results, although Pfizer didn’t seem to indicate the possible cost of these doses.
As is well known now, PAXLOVID’s mechanism of action targets the main protease of SARS-COV2. I previously noted that many drugs are able to act as protease inhibitors, and so what makes PAXLOVID unique compared to other proteases?
Mechanism of Action
Most protease inhibitors function through electrostatic interactions and tend to be fairly weak compared to covalent interactions. A good way to imagine these interactions is to imagine Velcro where the accumulation of sticking points strengthens the binding ability of the Velcro pieces, akin to a drug binding to the main protease. And just like Velcro, these interactions are reversible and may not last for very long.
As I previously indicated, PAXLOVID has several electrostatic interactions, but it also seems to have one covalent interaction, one that provides it with greater binding capabilities.
PAXLOVID contains a nitrile group (-CN) that is located nearby the Cysteine 145 residue of SARS-COV2’s main protease. Instead of engaging in interactions such as hydrogen bonding, the Sulfur atom of the Cysteine residue is able to bond to the Carbon of PAXLOVID’s -CN group and form a covalent bond.
Here’s the mechanism elucidated by Zhao et. al. 2021 (No, this is a different Zhao from the one I’ve continuously cited):
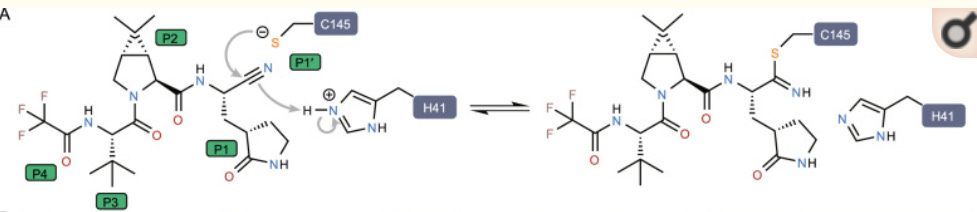
And here’s a brief overview for those who are interested in the mechanism:
This suggests that the thiol group of catalytic C145 attacks the electrophilic nitrile group at P1′ site of PF-07321332, resulting in the formation of a thioimidate adduct (Fig. (Fig.1A).1A). This result is also supported by tandem mass spectrometry analysis, which revealed the presence of a mass shift of 500 Dalton (Fig. (Fig.1J).1J). The reversibility of the covalent bond was supported by the dual conformations of the catalytic cysteine based on the electron density map, with the thiol group of cysteine not directly bonded to nitrile group of the inhibitor in the alternative conformation (Fig. (Fig.1E).1E).
To reiterate the main protease’s function, when proteins get translated they undergo proteolysis (breaking up proteins) where the long strand of newly formed amino acids gets chopped up into smaller units. In the case of the main protease, the active amino acid residues are the Cysteine 145 and Histidine 41 residues of the main protease (the blue blocks in the figure).
By targeting these amino acid residues a drug is able to elicit inhibition of the protease’s function. By doing so, protein subunits cannot be created to reform the viral particle and thus the virus is unable to propagate.
What’s absolutely unique to PAXLOVID is that the formation of that covalent bond renders the main protease useless, and unlike an electrostatic interaction these covalent interactions are far stronger and far more difficult to remove (note that even though this reaction is reversible, it likely lasts much longer than electrostatic interactions).
This is a unique mechanism of action, and it would indicate why this drug is far more effective than other protease inhibitors. This is promising, but we should still wait and see more information on possible adverse reactions and for the full report from the clinical trials.
But does that discredit other possibilities?
What about Ivermectin??
Ivermectin has been considered as a possible protease inhibitor, and I have indicated as much last time. However, Ivermectin does not have the same reversible covalent interaction that PAXLOVID does, meaning it should hypothetically be less effective against SARS-COV2. Nonetheless, if it still shows some efficacy that may be good enough; early treatment with a drug that has had a long history of use may be far more appealing than a new, highly experimental therapeutic that hasn’t had the same level of rigorous testing.
No, I am not saying to take Ivermectin, but we can examine whether there may be some evidence of a similar mechanism of action.
In an in vitro assay conducted by Mody et. al. 2021, researchers examined the activity of different protease inhibitors against SARS-COV2’s main protease. As we can see from the results, Ivermectin showed extremely high inhibition.
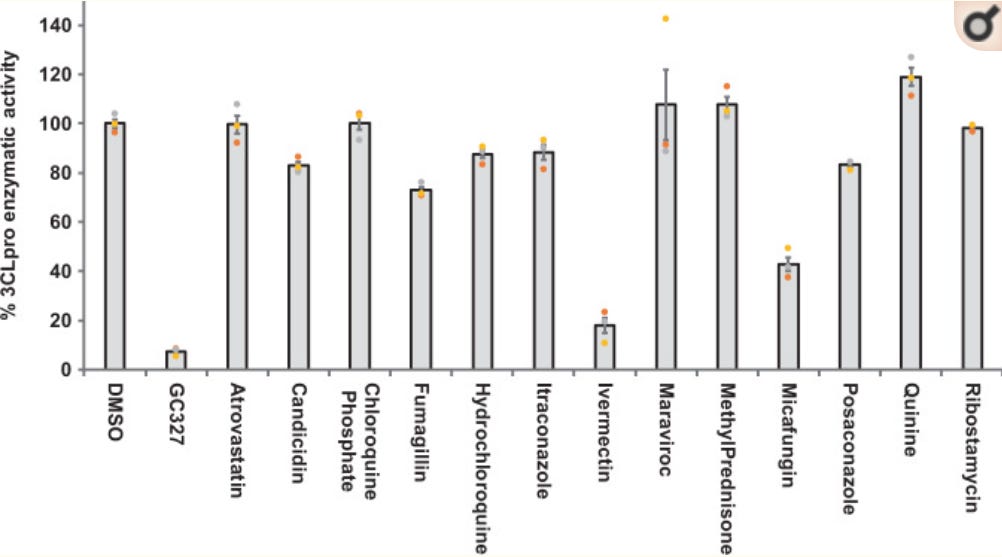
Remember, in vitro assays don’t translate directly into human trials, but they indicate something very promising, especially when compared to several other possible drugs.
Unfortunately, the clinical data is a little spotty for Ivermectin.
A meta-analysis conducted by Cruciani et. al. 2021 indicated little evidence of Ivermectin’s effectiveness as a prophylaxis.

So the evidence around Ivermectin’s use is highly controversial, but even then many doctors have attested to its effectiveness, and most likely highlights the importance of timing and dosing of the therapeutics.
So is PAXLOVID comparable to Ivermectin? Well, there is still a missing link that may help tie up some loose ends here.
Ritonavir: The P450 Enzyme Inhibitor
Many of Ivermectin’s detractors have argued that Ivermectin has a very low half life, and thus is not useful as a prophylactic.
PAXLOVID is being administered with a drug called Ritonavir, a cytochrome P450 enzyme inhibitor (CYP450). CYP450 is a liver enzyme responsible for metabolizing many of the compounds that we ingest, especially drugs. By inhibiting this enzyme, you can hinder the metabolization of a therapeutic and thus increase the serum concentration of the drug (in this case, PAXLOVID). So this indicates that a dose dependent response may be important to fight off SARS-COV2 when using protease inhibitors.
Strangely enough, Ritonavir targets the isozyme CYP450 3A4, the same enzyme that metabolizes Ivermectin.
Theoretically, that means that Ritonavir could be paired with Ivermectin to increase its serum concentrations, and possibly increasing it’s effectiveness.
But what about concern with overdosing and adverse reactions? Ivermectin has been targeted for having a decent number of adverse reactions.
Well, it seems like that concern may be a little overblown, as there is some evidence that Ivermectin may have a safer profile than previously indicated.
What’s even more amazing is that there are generic forms of Ritonavir, meaning that they may be widely available.
Once again, this is not an endorsement to use Ivermectin either alone or with Ritonavir. Instead, it points out that there may be something comparable to what Pfizer is offering, and something that should at least be looked into. If clinical trials prove this to be ineffective, we can consider that Ivermectin may not be a good candidate against SARS-COV2.
One important thing to highlight is that the administration of a P450 inhibitor may inhibit the metabolism of other drugs, so its use may be considered a contraindicator if someone is on a drug that may also be metabolized by CYP450. As more reports come out about PAXLOVID we should see indications highlighting this concern.
As it stands, PAXLOVID seems like a very promising therapeutic that may not have the same toxicity concerns as Molnupiravir. Nonetheless, we should wait and see what the rest of the study suggests about its effectiveness.
It also indicates that other protease inhibitors may want to be paired with CYP450 inhibitors and tested accordingly to examine possible therapeutics. It would be interesting to see something similar with Ivermectin, although the controversy surrounding this drug may make that very difficult.
So all of this at least seems promising, but I will wait and see what other data comes out.
Thank you for reading my newsletter. If you enjoy my articles please consider becoming a free subscriber in order to receive notifications.
And share with others who may find these newsletters interesting.
Also, please consider becoming a paid member. The research and work put into these articles takes many hours and being a paid subscriber allows me to continue to do this full time.
Citations
Pfizer’s Novel COVID-19 Oral Antiviral Treatment Candidate Reduced Risk of Hospitalization or Death by 89% in Interim Analysis of Phase 2/3 EPIC-HR Study. Taken from https://www.pfizer.com/news/press-release/press-release-detail/pfizers-novel-covid-19-oral-antiviral-treatment-candidate
Zhao et. al. 2021. Crystal structure of SARS-CoV-2 main protease in complex with protease inhibitor PF-07321332. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8533666/
Mody et. al. 2021. Identification of 3-chymotrypsin like protease (3CLPro) inhibitors as potential anti-SARS-CoV-2 agents. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7817688/
Cruciani et. al. 2021. Ivermectin for Prophylaxis and Treatment of COVID-19: A Systematic Review and Meta-Analysis. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8470309/
Also, if anyone wants to have any fun, try reading this Snopes article. It's quite frustrating when journalists don't do a decent amount of research before looking at the topic.
https://www.snopes.com/fact-check/pfizermectin-covid-drug/