


Growing recognition of long-term COVID vaccination adverse reactions
Part II: A look into POTS.

This post follows the prior post, which looked at the widely circulated Science article recognizing long-term health consequences related to the vaccines. Here, we will further expand upon one of the complications mentioned in the Science article (POTS). Although this article was originally intended to look at autoimmunity, it will be saved for the following post in order to not inundate readers with lengthy posts such as the one from yesterday.

Edit 7.12.2023: Timing and dosage of vaccines have been bolded below to make them more apparent to readers.
POTS Overview
Postural Orthostatic Tachycardia Syndrome, or POTS is a disease which is actually associated with small fiber neuropathy. As the name implies, POTS is an issue in which sudden changes in posture such as sitting upright may cause a sudden spike in heart rate (tachycardia). POTS itself is a rather nebulous description, as the presentation of POTS can be heterogeneous and dependent upon multiple factors. It can sometimes be considered under the umbrella term of orthostatic intolerance in reference to complications that arise when standing or sitting upright. If orthostatic intolerance sounds a bit familiar, it was one of the underlying conditions of the Japanese adolescent who suffered from multi-systemic inflammation following a COVID booster who passed at night (in this case, the term that was used was orthostatic dysregulation which appears interchangeable with intolerance).
POTS manifests predominately in women, and usually around the onset of adolescence or early adulthood, and thus can be rather debilitating if not properly managed or treated.
There are multiple explanations for the manifestation of POTS, including autoimmunity, a hyperadrenergic response, and even neuropathy (detailed a bit further below).
The main presentation of POTS is a heart rate increase of 30 bpm within minutes of standing or placing a head in an upright position. For adolescents, the heart rate considered for POTS is a bit higher- an increase of 40 bpm.
Additional symptoms of POTS can include fatigue, syncope (fainting), GI problems, exercise intolerance, headaches, cognitive impairments, and chest pain (all of this sounds a bit familiar, no?).
Vernino, et al.1 provides an outline for some requirements for POTS diagnosis:
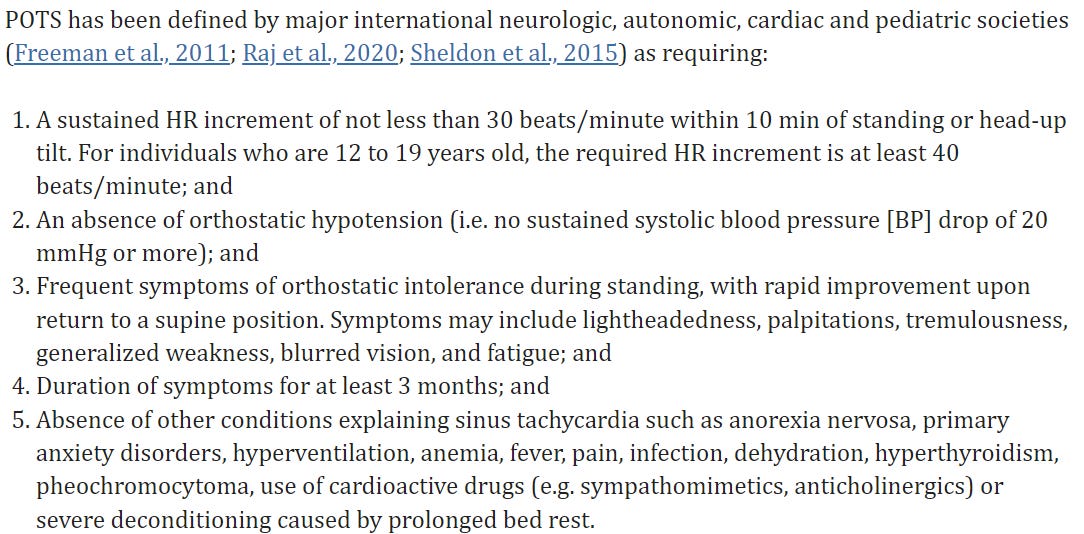
The explanation for POTS is rather interesting. It’s suggested in Zhao, S & Tran, VH.2 that POTS may be a consequence of the body being unable to compensate for biomechanical changes that occur due to gravity. For instance, when standing or sitting upright the body must take into account the new blood flow gradient, usually by way of increasing the volume of blood that gets pumped so that the same rate of blood flow is maintained. However, in those with orthostatic dysfunction the volume that gets pumped is reduced, thus requiring the body to compensate by way of increasing the heart rate and contractility of blood vessels, which usually involves over stimulation of the sympathetic nervous system in order to increase cardiac output with the consequence of increased risk of tachycardia. Clinical examination for those with POTS tend to show regular blood pressure while also noting elevated heartrate.
Given this association, we can see an association with small fiber neuropathy, where damage to nerves necessary to maintain blood vessel constriction may lead to an inability to properly pump blood. In this case, a nerve-related consequence of POTS is referred to as Neuropathic POTS, wherein the loss of nerve function within the lower extremities leads to reduced reuptake of the catecholamine norepinephrine, which is compensated by way of greater sympathetic activation.3 Neuropathic POTS may be recognized by venous blood pooling within the legs.
Long COVID & POTS
Given these overlaps in symptoms, it’s not too difficult to consider the possibility that many Long COVID patients are experiencing various degrees of POTS, especially when considering symptoms of fatigue and exercise intolerance that tend to be discussed in mainstream press.
A review from Ormiston, et al.4 provides additional information on Long COVID and POTS:
POTS and long COVID are both multisystem disorders.11 , 31 , 32 Although our knowledge of the prevalence of POTS in COVID-19 survivors is limited by most studies being retrospective or having small sample sizes, it is estimated that 2%–14% of COVID-19 survivors develop POTS and 9%–61% experience POTS-like symptoms, such as tachycardia and palpitations, within 6–8 months of infection (Figure 1 ).9 , 19 , 33, 34, 35 Additionally, symptoms suggestive of autonomic dysfunction, such as orthostatic intolerance and gastrointestinal dysfunction, as well as features of a hyperadrenergic state and symptoms of MCAS have been observed.9 , 19 , 36 , 37 Although a review by Larsen et al36 suggests that POTS may be the most common form of autonomic dysfunction in patients with long COVID, orthostatic intolerance and other autonomic abnormalities in the absence of POTS should also be considered.38 , 39 In patients with symptoms related to autonomic dysfunction arising in the parainfectious or postinfectious period of COVID-19 (n = 27), 63% of patients had abnormalities on autonomic function testing, most commonly orthostatic intolerance, and 22% of patients fulfilled criteria for POTS.39 However, the majority of patients experiencing orthostatic symptoms had normal autonomic testing results.
As Ormiston, et al. go on to describe the rates of POTS diagnoses within the US and Canada appear to have increased since the onset of the pandemic. Although variability in circumstances and other health factors should be considered, it does add further evidence of complications related to post-SARS-COV2 infection.
This is why I criticize claims outright dismissing the prevalence of Long COVID, as it makes it harder to piece together relevant information, and may miss out on necessary context. It also doesn’t help that claims refuting Long COVID tend to rely on surveys that can’t differentiate Long COVID sufferers from non-Long COVID background. Maybe a better association would be the examination of POTS, although this would require clinical observations that need more time and effort than researchers would like to put in.
Nonetheless, this points to another avenue worth considering when comparing adverse reactions from vaccination and symptoms of Long COVID. It’s important to look for convergence wherever possible.
POTS Post-Vaccination
Similar to small fiber neuropathy, several reports have come out with respect to POTS post-vaccination.
A case report from Park, et al.5 describes a 40-year old man who developed intermittent headaches, palpitations, and dyspnea (shortness of breath) a week following his first Moderna vaccine.
A head-up tilt test revealed orthostatic tachycardia where the patients heartrate ranged between 72-110 beats per minute.
Autoantibodies don’t appear to be tested aside from a mention that a serology test for autoimmunity came back negative, which doesn’t describe much about which autoimmune diseases in particular were being examined.
The patient was provided the beta blocker Propranolol for two months which appeared to improve symptoms, with symptoms seeming to fully resolve after 5 months.
The use of beta-blockers is rather interesting given the hyperadrenergic response seen in those with POTS which appear to counteract the lack of norepinephrine response that may be occurring in these individuals. Beta-blockers operate by way of preventing the binding of catecholamines to corresponding adrenergic receptors. It’s curious that the patient would see an alleviation of symptoms if his POTS may be due to an inability to respond to norepinephrine, although the use of this drug may help reduce the extreme compensatory mechanism taking place.
Note that the case report from Schelke, et al. used the beta-blocker Nadolol to aid with tachycardia, suggesting that the use of beta-blockers may be beneficial for some POTS patients (remember that readers should discuss medications with their doctor).
A case report from Reddy, et al.6 notes a 42-year old man who presented to a clinic with sinus tachycardia and presyncope (lightheaded/dizzy) episodes. Sinus tachycardia refers to a condition in which the heart’s natural pacemaker, the sinus node, is overactivated causing rapid heartbeats.
Symptoms appeared within 24 hours of receiving the first dose of the Pfizer/BioNTech vaccine, presenting as fatigue and myalgia for the first few days before the presentation of tachycardia on day 7.
The patient also had a prior history of hypothyroidism and was on routine Vitamin B-12 treatments for a B-12 deficiency.
Clinical investigation did not note anything abnormal, aside from the patient’s heartbeat being elevated at 158 bpm which spontaneously declined to 126 bpm.
The patient was still symptomatic since the report, and was told to manage symptoms with lifestyle changes such as wearing compression socks and increasing sodium intake.
Hermel, et al.7 provides a case of a 46-year old woman who presented to the clinic on October 2021 with lightheadedness, tremors, rapid heart rate, and Raynaud’s Phenomenon, which is constriction of narrow blood vessels within the body’s extremities such as the fingers, toes, ears, and/or nose. This usually occurs when it’s cold outside, and presents with redness within these body parts.
Symptoms began within 2 days of receiving the first dose of Pfizer/BioNTech’s vaccine, where the patient began experiencing dysesthesia, paresthesia, and soreness and numbness within her right arm (the injected arm) as well as rapid heart beats and tremors.
Unlike prior case reports, this patient was previously infected with SARS-COV2 around December 2020.
The outpatient clinic which the patient first went to prescribed oral Dexamethasone (corticosteroid) as well as over-the-counter antihistamine Diphenhydramine (brand name Benadryl) as needed.
Worsening symptoms landed the patient in ER with where she was provided intravenous Dexamethasone and later released.
A visit with her PCP eventually led to a referral to a specialist, in which she was diagnosis with sinus tachycardia with a maximum heart rate of 170 bpm. Tilt-table tests where the patient went from a supine (flat) position to an upright position noted a heart rate increase from 93 to 140, which was also accompanied by presentation of Raynaud’s Phenomenon.
The patient was placed onto a conservative treatment regimen similar to that of Reddy, et al. aside from a prescription for Ivabradine8. Ivabradine blocks the channel responsible for inducing sinus node activation, which leads to a reduction in a patient’s heart rate.
In addition, the patient was interestingly placed onto an integrative treatment regimen, which included dietary supplements such as turmeric, Vitamin C, Vitamin D3, Quercetin, and Resveratrol, among a few of the supplements listed.
At follow-up in June 2022 the patient reported improvements in various symptoms, although Raynaud’s Phenomenon appeared to still present within her hands and feet.
Although all of this may seem like a bog to get through (is that the right phrase?), remember that it’s consilience and convergence of information that we are seeking out. By analyzing individual case reports we can paint a clearer picture of how some of these patients present, as well as viable treatments.
The last two case reports I found are rather interesting ones. In these two cases are adolescent boys who had evidence of POTS. One boy in particular also presented with evidence of myocarditis in conjunction with POTS and raises a serious consideration in the evaluation of mycarditis.
A case from Maharaj, et al.9 reports on a 15-year old South Asian boy who experienced symptoms related to POTS such as episodes of faintness lightheadedness two weeks following a Pfizer/BioNTech booster. In this case the patient also received an HPV vaccine within the months prior, which adds some confounding to this presentation.
The patient was originally very active and played sports. He had no prior history of a COVID infection, and no information is provided as to whether he experienced some of these symptoms following the first two doses of the vaccine.
Clinical tests did not show anything abnormal aside from an inpatient telemetry test which noted evidence of sinus tachycardia. No tilt-table test was performed due to it being unavailable.
The patient was started with an inpatient treatment of the corticosteroid Fludrocortisone as well as Ivabradine, along with higher sodium and fluid intake. Exercise intolerance and fatigue began to decrease, and symptoms of syncope were mostly gone by the time of discharge. The patient was placed on Fludrocortisone at the 1-month follow up and appeared to not show any additional concerning signs, although the full outcome of the patient is not provided.
This case in particular differs from the ones highlighted above, as this is one of the only reported cases of POTS occurring in an adolescent. This is also one of the first cases to report on POTS following the booster, although the HPV vaccine should also be considered within this context as a confounding variable.
This raises a question of why this discrepant presentation occurred. If autoimmunity is argued to be the culprit, it has to be considered within the context of a priming phase followed by memory recall. In the case of this patient, the age may suggest a priming feature caused by the two prior doses, which may have induced an adaptive memory recall event when provided the booster, which led to the presentation of POTS.
This may also raise the question as to whether adult patients, or at least patients who experience POTS after the first dose, may have had some priming event in the past that were triggered by the vaccine.
This is also one of the first reported cases of POTS occurring in a South Asian patient. It’s important to remember that absence of evidence is not evidence of absence, but it raises further consideration of possible ethnic background as being a factor in autoimmunity.
This last case is a very interesting one. It comes from Sanada, et al.10 which report on a 13-year old boy who presented to a clinic with headaches, fatigue, and sleep disturbances following a second dose of the Pfizer/BioNTech vaccine. He presented to the clinic 14 days after symptom onset. Symptoms first appeared on the day of the second dose.
This patient was started on Acetaminophen, Ibuprofen, and Chinese herbs in an attempt to alleviate the symptoms to no avail, and the patient worsened over the following days.
However, it was noted during an active standing test (AST) that the patients heart rate shot up from 65 bpm to 140 bpm, leading to a diagnosis of POTS.
The patient was told to increase fluid and sodium intake, and was also prescribed Midodrine for orthostatic hypotension (note that hypotension is an exclusionary criteria for POTS).
The patient later presented to the clinic at day 33 following the 2nd vaccination where the patient still presented with lightheadedness, fatigue, headaches, and palpitations.
Blood tests noted an increase in creatine kinase as well as troponin 1. Imaging of the heart led to evidence of slight pericardial effusion (fluid accumulation within the pericardial cavity of the heart), leading to a diagnosis of mild myocarditis in this patient.
Please note that “mild” here is not being used to indicate that the myocarditis is, well, mild, but rather to differentiate it from other forms of myocarditis.
The course of events for this patient is rather complicated. Following the myocarditis diagnosis the patient was advised to rest, saline provided via IV was provided to aid with the symptoms of POTs, and the patient was also started on the anticonvulsant Pregabalin (brand name Lyrica) as well as Ramelteon to help him sleep. Unfortunately, aside from a decrease in the headaches, the other symptoms persisted and the patient was placed on IVIG on day 75 following his vaccination, with partial improvement of symptoms including the ability to walk longer distances. Creatine kinase and troponin levels decreased, and pericardial effusion seemed to have dissipated.
However, the patient returned to a tertiary clinic on day 210 post-vaccination. Blood markers appeared normal. A head-up tilt test was conducted, which noted a large spike in heart rate. The quick recovery of blood pressure after standing excluded orthostatic hypotension leading to the diagnosis once again of POTS.
The patient discontinued the Chinese herbs as well as the Pregabalin. Midodrine dosage was increased, and a prescription for Propranolol and the norepinephrine precursor Droxidopa (L-DOPS- usually used for orthostatic hypotension) was provided. The new medications appeared to help the patient function mid-day, although the case report does not note whether the patient made a full recovery.
This last case is a very important case to highlight. Evidence of myocarditis is rather difficult unless a patient undergoes bloodwork and imaging studies to look for evidence of heart inflammation. The overlap of POTS and myocarditis in this adolescent raises critical considerations as to whether some of these myocarditis patients also experience POTS concurrently or preceding a case of myocarditis. In the case of Sanada, et al, it’s hard to determine whether the POTS caused myocarditis or whether they were both a consequence of broader issues related to the vaccines. Such a question may be found in the literature, although several remarks suggest that POTS may be mistaken for heart failure. There’s isn’t quite clear evidence of POTS being causative of myocarditis (at least within the very limited information I have looked at). The review from Zhao, S & Tran, VH. makes mention that no deaths have so far been directly attributed to POTS, and so it’s possible that this patient may have unfortunately experienced both concurrently.
If this were the case, then this is suggestive that either one of these pathologies may mask the other. Given that the test for POTS is rather easy (measure heart rates in people who move from a supine to a standing position), it may be worth considering whether such a test should be provided more widely in order to possibly diagnose POTs.
As this post has gone on too long, the rest of this evaluation will be saved for the next post, which should go a bit deeper into consilience as well as a look back at the hyper-catecholaminergic hypothesis, as well as a look into autoimmunity in all of these vaccine-related complications.
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Vernino, S., Bourne, K. M., Stiles, L. E., Grubb, B. P., Fedorowski, A., Stewart, J. M., Arnold, A. C., Pace, L. A., Axelsson, J., Boris, J. R., Moak, J. P., Goodman, B. P., Chémali, K. R., Chung, T. H., Goldstein, D. S., Diedrich, A., Miglis, M. G., Cortez, M. M., Miller, A. J., Freeman, R., … Raj, S. R. (2021). Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting - Part 1. Autonomic neuroscience : basic & clinical, 235, 102828. https://doi.org/10.1016/j.autneu.2021.102828
Zhao S, Tran VH. Postural Orthostatic Tachycardia Syndrome. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541074/
Jacob, G., Costa, F., Shannon, J. R., Robertson, R. M., Wathen, M., Stein, M., Biaggioni, I., Ertl, A., Black, B., & Robertson, D. (2000). The neuropathic postural tachycardia syndrome. The New England journal of medicine, 343(14), 1008–1014. https://doi.org/10.1056/NEJM200010053431404
Ormiston, C. K., Świątkiewicz, I., & Taub, P. R. (2022). Postural orthostatic tachycardia syndrome as a sequela of COVID-19. Heart rhythm, 19(11), 1880–1889. Advance online publication. https://doi.org/10.1016/j.hrthm.2022.07.014
Park, J., Kim, S., Lee, J., & An, J. Y. (2022). A case of transient POTS following COVID-19 vaccine. Acta neurologica Belgica, 122(4), 1081–1083. https://doi.org/10.1007/s13760-022-02002-2
Reddy, S., Reddy, S., & Arora, M. (2021). A Case of Postural Orthostatic Tachycardia Syndrome Secondary to the Messenger RNA COVID-19 Vaccine. Cureus, 13(5), e14837. https://doi.org/10.7759/cureus.14837
Hermel, M., Sweeney, M., Abud, E., Luskin, K., Criado, J. P., Bonakdar, R., Gray, J., & Ahern, T. (2022). COVID-19 Vaccination Might Induce Postural Orthostatic Tachycardia Syndrome: A Case Report. Vaccines, 10(7), 991. https://doi.org/10.3390/vaccines10070991
Reed M, Kerndt CC, Nicolas D. Ivabradine. [Updated 2023 May 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507783/
Maharaj, N., Swarath, S., Seecheran, R., Seecheran, V., Panday, A., & Seecheran, N. (2023). Suspected COVID-19 mRNA Vaccine-Induced Postural Orthostatic Tachycardia Syndrome. Cureus, 15(1), e34236. https://doi.org/10.7759/cureus.34236
Sanada, Y., Azuma, J., Hirano, Y., Hasegawa, Y., & Yamamoto, T. (2022). Overlapping Myocarditis and Postural Orthostatic Tachycardia Syndrome After COVID-19 Messenger RNA Vaccination: A Case Report. Cureus, 14(11), e31006. https://doi.org/10.7759/cureus.31006