


Fecal Microbiota Transplants and Gut Dysbiosis
A scientific examination of whether there is merit to the phrase "Eat Sh!t!"

When writing my posts on the microbiome and ways of helping to support/improve it, I had to leave a lot of topics out due to the huge scope of the assessment. However, at the time I forgot that I was asked if I would look into Fecal Transplants and whether they are efficacious (apologies for not remember who asked this question!). Unfortunately, I completely forgot about that comment and so what better way to start the weekend than to start with a little poop talk? Yes, the information here may appear rather crass and should probably not be read while eating, but remember that science can sometimes be messy. So avoid if faint of heart or stay if interested. Either way, enjoy your Friday!
Also, note that this is intended to be a very broad, very general overview. The studies cited were not fully analyzed and likely come with critical context and limitations. Please be aware and assess the information for yourself.
*Title and in-text words were changed from microbial to microbiota for FMT.
In times when a patient suffers organ failure the best protocol may be to provide an organ transplant. It’s a rather common surgical procedure, even if organ donors may be limited and prognosis after donation may not be the best in the following years.
If we consider our microbiome being its own entity, in its own state of ebb and flow, and likely to suffer severe alterations in microbial composition (dysbiosis), then in some regards it would make sense to believe that one would be able to transplant new microbes to colonize our guts and bodies. We do that every time we eat/drink fermented foods, take probiotics, or even inhale air from the surrounding environment.
But strangely enough the idea of transplanting microbes, coined fecal microbiota transplants (FMT), has been around for centuries, even if the concept of a microbiome and beneficial bacteria gained prominence in recent decades.
A brief history of Fecal Transplants*
*This may be a section worth avoiding for those who are eating. Just be forewarned!
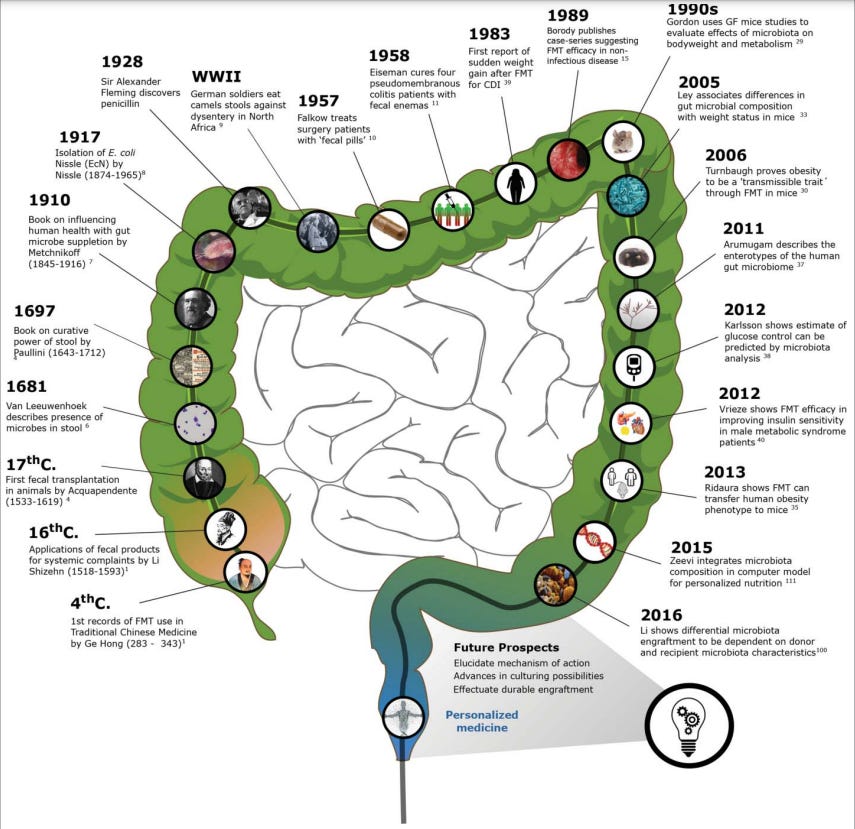
The practice of fecal transplants has been around for many centuries, with some of the earliest recordings coming from China during the 4th Century in which special “soups” were provided to people with diarrhea and food poisoning.
Groot, et al.1 provides a historical account of these recordings:
The first records of fecal transplantation date back to 4th century China, where “yellow soup” was applied in cases of severe food poisoning and diarrhea.1 Subsequent records reverently speak of “golden syrup.”2 By the 16th century, the Chinese had developed a variety of feces-derived products for gastrointestinal complaints as well as systemic symptoms such as fever and pain.1 Meanwhile, Bedouin groups were said to have consumed the stools of their camels as a remedy for bacterial dysentery.3 Italian anatomist and surgeon Acquapendente (1537–1619) further extended this to a concept he coined “transfaunation,” the transfer of gastrointestinal content from a healthy to a sick animal, which has since been applied extensively in the field of veterinary medicine.4 Interestingly, many animal species are found to naturally practice coprophagia, leading to a greater diversity of microorganisms in their intestines, enabling them to digest a greater number of food sources.5
Well, talk about a euphemism!
The practice of fecal transplants would later make their way to Europe in the following centuries, but more on that can be read in the review from Groot, et al.
The biggest turning point in fecal transplant research appears to have come about during the 1950s, which was also around the same time that antibiotic use became widespread.
Although antibiotics have helped treat many bacteria-related diseases and have helped increased global survivability, the use of such antibiotics led to an increase of pseudomembranous colitis2, which is a severe inflammation of the inner lining of the upper colon.
Although the presentation of pseudomembranous colitis was assumed to be from a bacterial infection (with some assuming it was related to a Staphylococcus aureus infection and was labeled Staphylococcus pseudomembranous colitis at the time) treatment was generally met with antibiotics but with mixed results.
As doctors began to see more cases of colitis with not much help, a group of doctors led by Dr. Ben Eiseman decided to take the feces from well individuals, created an enema solution, and provide them to 4 colitis patients leading to full recovery of the patients.
It’s hard to figure out how aware of beneficial bacteria Eiseman and his colleagues were at the time, as Groot, et al. notes that the team was cognizant of good/bad gut bacteria to some degree.3 Unfortunately, the actual published work from Eiseman, et al.4 from 1958 detailing this procedure doesn’t seem accessible, and so it’s hard to corroborate this assumption.
Regardless, this procedure conducted by Eiseman and his colleagues would become the first modern form of fecal transplantation, and the field only grew from there.
In the proceeding years this procedure of using fecal enema was mimicked by other doctors with nearly universal positive results. However, the field of fecal transplants and microbiome research met a strange lull for several decades, only gaining a resurgence around the 1980s.
Cases of colitis would eventually be attributed to the bacteria Clostridium difficile, which remains a consequence of secondary bacterial infection post-antibiotic use even up to this day.
As more weight has been put towards beneficial bacteria, especially with efforts to elucidate the microbiome the field has begun to expand and currently research is looking into different methods of fecal transplant as a way of treating many diseases.
Modern Fecal Transplant Procedures
As of now different methods of fecal transplant procedures are available.
The most common is one in which bacteria sourced from a healthy individual is mixed in a saline solution and sprayed into the colons of patients via a colonoscopy.
Johns Hopkins University has a cute, little video highlighting this procedure:
FMT can also be conducted via the upper GI tract via endoscopic procedure or even through lyophilized oral capsules. Results between different methods have varied, with patient compliance and price generally playing a factory in the given procedure as well. It’s even been argued that FMT that utilizes both the upper GI tract and the lower GI tract may be the best approach.
Wang, et al.5 provides an overview of some of these delivery methods, although the review may be good for those who want a general overview on FMT:
The current administration of fecal material by means include upper GI route (via esophagogastroduodenoscopy (EGD), nasogastric, nasojejunal, or nasoduodenal tube), lower GI route (via colonoscopy or retention enema), and oral capsule. In general, FMT via the upper GI route can be administered in patients with an inflamed colon; however, the discomfort sensation during tube placement, risks of aspiration, and inability to evaluate the colon mucosa or to collect mucosa tissue samples are weak points. FMT via colonoscopy has superiority in recolonizing the entire colon with favorable bacteria, and bowel cleaning can probably reduce the number of residual organisms and spores to visualize the entire colon, but it is a relatively risky, expensive, and invasive procedure. FMT via retention enema is more affordable and less invasive than colonoscopy, but the donor fecal material cannot be delivered to the entire colon and is limited to the distal colon. Although the efficacy of retention enema had been once doubted, Orenstein and Dubberke et al. have proven it more efficient and safe than placebo in phase I and phase II recurrent CDI clinical trials.64, 65 Oral capsule for FMT administration has the advantages of less invasion and high patient acceptability, but the expense and large capsule burden are its disadvantages.52, 66
FMT as a Therapy
So far the literature has been in agreement that FMT use for the treatment of C. difficile has met with great success, with most cases having very few side effects aside from the initial discomfort and bloating as the gut environment becomes recolonized and shuffles out the C. difficile.
However, the uptake of this approach is still not widespread. The FDA has not approved of any specific procedure. Some have also argued that antibiotic use of vancomycin may be comparable to FMT, and that this procedure should be reserved for those in which chronic C. difficile infections occur or when antibiotics don’t appear to be effective.6
Aside from C. difficile infections researchers are looking into using FMT to treat other diseases such as irritable bowel disease, ulcerative colitis, sepsis, and even in the management of gut dysbiosis in those with cancer or other diseases.
However, given that underlying mechanisms are responsible for the gut dysbiosis in these individuals questions must be raised as to whether FMT would actually be beneficial for other diseases.
This can be seen in irritable bowel disease (IBD). It appears that FMT in those with IBS has been met with mixed results, with some studies noting no drastic difference between IBD and non-IBD C. difficile patients7 and may be beneficial. However, a meta-analysis on IBD noted mixed results, suggesting that the underlying mechanism of IBD may be influencing the gut homeostasis.8
Remember that in those with leaky gut bacteremia is a real concern, and the use of FMT may actually lead bacteria to travel from the gut into the bloodstream. However, this effect may also occur in those who take probiotics as well, and was mentioned previously when discussing probiotics for hospitalized patients. This concern was raised in a review from Keskey, et al.9 on FMT for sepsis patients.
In cases of obese individuals results have been mixed. One trial from Yu, et al.10 in which obese and some insulin-resistant participants were provided FMT capsules from healthy, lean donors for 6 weeks, an engraftment of donor microbes was noticed, although metabolism and insulin sensitivity didn’t appear to improve in these participants. This may be due to low dosage and the duration of treatment, as the researchers note a pilot study in which FMT was delivered endoscopically led to insulin sensitivity in a small group of patients.
As of now research continues to look into other avenues of FMT for treating other diseases, although so far results appear to suggest that FMT may be best saved for treating C. difficile infections.
The FMT Super-Donor
Our microbiomes are the sum of their parts, being influenced by lifestyle habits such as diet, exercise, and sleep, as we as other genetic factors.
Therefore, it comes as no surprise that researchers are searching for an optimized FMT donor.
Such individuals have been described Super-donors in the literature, referring to donors whose “samples” have led to high FMT outcomes.11

As of now the search for this supposed super-donor is in its early stages, just as the field of FMT is in its early stages.
But if one were to consider the significance of the microbiome, it’s worth considering if we should consider ourselves to be our own super-donors.
A bit cheesy, but keep in mind that our microbiome is critical to our overall health. Thus, it would be in our best interest to at least try to optimize our microbiome to the best of our ability. That includes foregoing a lot of modern foods and habits that have debilitated our gut microbes, and may actually be leading to the extinction of key microbes; a phenomenon labeled as an invisible extinction.
Thus, how we treat our microbiomes will have a great effect on our overall health. In a similar way that we have banked sperm, eggs, and sources of DNA we may begin to widely bank our own feces in case a debilitating disease or course of antibiotics leaves us with a dysbiotic gut. It’s possible that in the near future such a resource will gain prominence, but for now consider doing what you can to help maintain the microbiome you already have.
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

de Groot, P. F., Frissen, M. N., de Clercq, N. C., & Nieuwdorp, M. (2017). Fecal microbiota transplantation in metabolic syndrome: History, present and future. Gut microbes, 8(3), 253–267. https://doi.org/10.1080/19490976.2017.1293224
Salen P, Stankewicz HA. Pseudomembranous Colitis. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470319/
Some pieces of literature have suggested that the term used at the time was “microflora”, although that doesn’t tell us much about what was known about beneficial bacteria. This could be due to the fact that this idea was considered rather novel, and coming about at a time when antibiotic use gained prevalence may not have sit well with the medical narrative at the time, which may have considered bacteria to inherently be pathogenic.
EISEMAN, B., SILEN, W., BASCOM, G. S., & KAUVAR, A. J. (1958). Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery, 44(5), 854–859.
Wang, J. W., Kuo, C. H., Kuo, F. C., Wang, Y. K., Hsu, W. H., Yu, F. J., Hu, H. M., Hsu, P. I., Wang, J. Y., & Wu, D. C. (2019). Fecal microbiota transplantation: Review and update. Journal of the Formosan Medical Association = Taiwan yi zhi, 118 Suppl 1, S23–S31. https://doi.org/10.1016/j.jfma.2018.08.011
Tan, X., & Johnson, S. (2019). Fecal microbiota transplantation (FMT) for C. difficile infection, just say 'No'. Anaerobe, 60, 102092. https://doi.org/10.1016/j.anaerobe.2019.102092
Hirten, R. P., Grinspan, A., Fu, S. C., Luo, Y., Suarez-Farinas, M., Rowland, J., Contijoch, E. J., Mogno, I., Yang, N., Luong, T., Labrias, P. R., Peter, I., Cho, J. H., Sands, B. E., Colombel, J. F., Faith, J. J., & Clemente, J. C. (2019). Microbial Engraftment and Efficacy of Fecal Microbiota Transplant for Clostridium Difficile in Patients With and Without Inflammatory Bowel Disease. Inflammatory bowel diseases, 25(6), 969–979. https://doi.org/10.1093/ibd/izy398
Myneedu, K., Deoker, A., Schmulson, M. J., & Bashashati, M. (2019). Fecal microbiota transplantation in irritable bowel syndrome: A systematic review and meta-analysis. United European gastroenterology journal, 7(8), 1033–1041. https://doi.org/10.1177/2050640619866990
Keskey, R., Cone, J. T., DeFazio, J. R., & Alverdy, J. C. (2020). The use of fecal microbiota transplant in sepsis. Translational research : the journal of laboratory and clinical medicine, 226, 12–25. https://doi.org/10.1016/j.trsl.2020.07.002
Yu, E. W., Gao, L., Stastka, P., Cheney, M. C., Mahabamunuge, J., Torres Soto, M., Ford, C. B., Bryant, J. A., Henn, M. R., & Hohmann, E. L. (2020). Fecal microbiota transplantation for the improvement of metabolism in obesity: The FMT-TRIM double-blind placebo-controlled pilot trial. PLoS medicine, 17(3), e1003051. https://doi.org/10.1371/journal.pmed.1003051
Wilson, B. C., Vatanen, T., Cutfield, W. S., & O'Sullivan, J. M. (2019). The Super-Donor Phenomenon in Fecal Microbiota Transplantation. Frontiers in cellular and infection microbiology, 9, 2. https://doi.org/10.3389/fcimb.2019.00002
When on antibiotics for the first time in 20 years maybe 2 years ago (wisdom teeth extraction), I also researched a bit about that stuff. I was taking a wild mix of bacteria in high dose, timed centered in between the antibio bomb hits, kinda like repairing a tank factory in Command & Conquer while it is being attacked (but in a manner that it wouldn't be instantly deactivated by the pills).
But from what I found, taking healthy gut biome samples _before_ the antibiotics treatment starts, and after it, planting it back, yields far superior results, more quickly, to get back to as it was before, as the biome seems to be highly indiviaual with regards to what kinds of bacteria, and the ratios, are good for someone. E.g. some people will more likely develop MS if one bacterium is present alot, while it's not doing anything bad in others. (so I didn't buy the supplement that had that in it, just in case, lol)
Don't have the references at hand. But it's a bummer that that sort of stuff is not only not offered regularly for this, it's not even on the radar of any doctor here, it's not an established procedure.
While everyone thought a man discovered penicillin, it was a woman behind it..
“In 1941 , lab assistant Mary Hunt offered up a couple of over ripe melons covered in a robust golden mould and the lab went ballistic.
The mould turned out to be Penicillium chrysogeum, which yielded 200 times the amount of penicillin that Flemming described.”