


Clarifying the UK’s COVID-19 Vaccine Surveillance Report- and Immunity in General (Context)
Before resorting to Paranoia, make sure to Understand the Evidence

Recently this report by the UK has been circulating around among many people skeptical about the vaccines. Most of the attention was brought to this section:

This has caused a lot of concern that these vaccines are not only not working, but that they are going to cause vaccinated people to become extremely susceptible to spike protein mutations.
There’s a bit to go through here, but we need to make we argue from a rationale perspective and provide context.
Nucleocapsid Protein
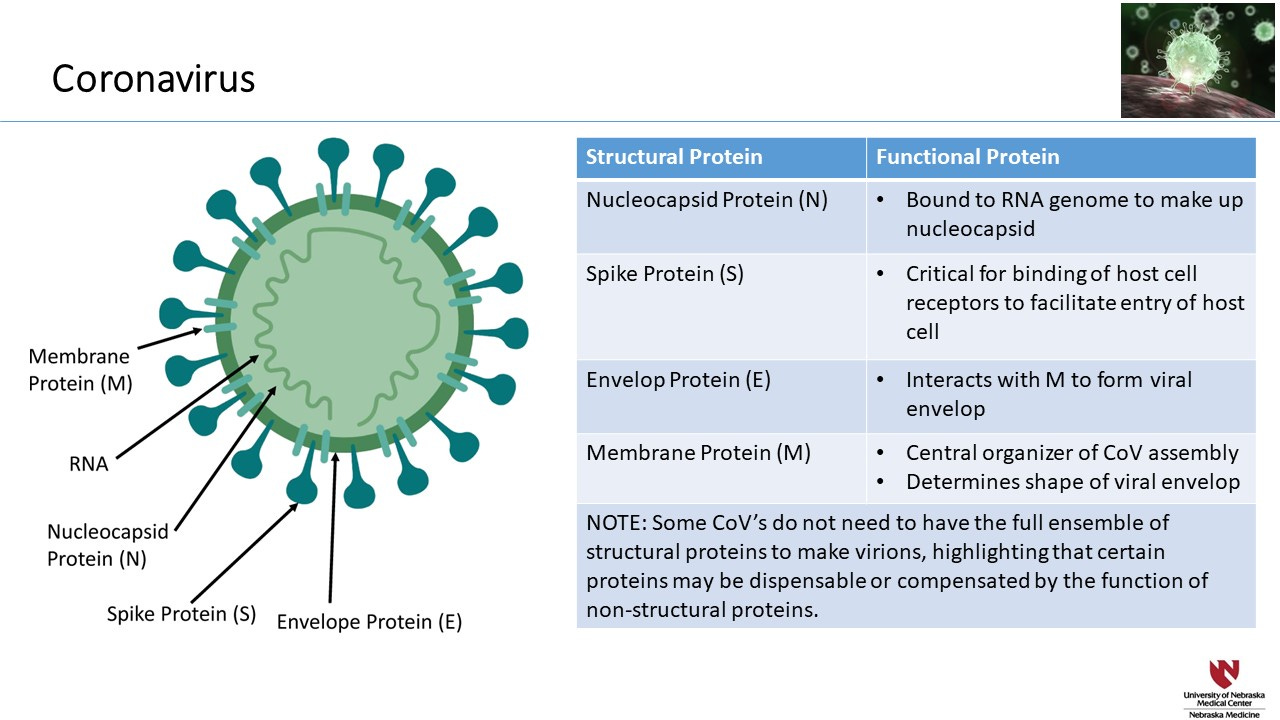
The Nucleocapsid protein is the protein responsible for coiling up SARS-COV2’s RNA genome. It functions similar to the histone proteins within the nuclei of our cells that wind our DNA up tightly. This is important, because it allows our (and the virus’) genome to become compact and fit in a tighter space while also providing protection to the genome. There is also evidence that it may be responsible for regulating immune responses.
To further illustrate this point, here’s an excerpt from Surjit et. al. 2008. Although it refers to SARS-COV’s N Protein they both function similarly:
Being the capsid protein, the primary function of the N-protein is to package the genomic RNA in a protective covering. In order to achieve this structure, the N-protein must be equipped with two different characteristic properties such as: (i) being able to recognize the genomic RNA and associate with it; (ii) self-associate into an oligomer to form the capsid. The N-protein of SARS-CoV has been experimentally proven to possess these properties in vitro, as discussed below.
Note that the word “capsid” refers to a protein that coats the virus particle. Therefore, a “Nucleocapsid” would be a protein that coats the nucleic acids i.e. the viral genome, so even though it’s labeled as a coating protein it cannot be interchanged with the actual virus capsid that coats and protects the viral particle.
Unfortunately, this creates a conundrum; the nucleocapsid is sequestered within the virus, meaning that it will not be able to be recognized, and thus targeted by the immune system directly.
The reason why people who acquire natural immunity gain antibodies against the N protein is because the irregularity that occurs with viral replication (compared to normal cellular replication) will cause a cascade of cellular events where our cells recognize that something is not right and illicit an immune response.
So if viral replication may be a requirement to notice certain proteins we can understand why vaccinated individuals may not be able to produce antibodies to the N protein.
Vaccinated individuals are able to illicit a response to the spike protein because the spike protein is located on the outside of the viral particle and is also needed to bind to the ACEII receptor. An antibody response to the spike protein should be able to prevent viral binding and therefore viral replication would be hindered.
So the vaccine should be able to do its job. The issue is that by doing its job it prevents the adaptive immune system from learning other aspects of the virus, creating an “all eggs in one basket” case. If spike mutations reduce antibody binding affinity they may be able to elude the immune system and cause infection. But remember that there is more to the story, and one that should provide some needed context.
Where You Test & Where You Collect Samples Matter
Note that antibody titers are measured by examining antibodies in the blood-this is why it’s called seroprevalence (prevalence of the antibodies in the blood). This is important, because it highlights one of the biggest issues of this entire pandemic.
We have indicated that, during an infection, vaccinated individuals will illicit an immune response against the virus but will not be able to “learn” more parts of the virus while those with naturally immunity will learn every bit of the virus and respond accordingly, based on information from blood samples.
The big issue here is that blood samples indicate the function of the systemic immune system (i.e. the body’s immune system) but this does not include the immune system of the mucosal system.
As I have alluded to in my previous Substack posts, and in particular my paid members only post, the mucosal immune system- specifically the nasal passage- does not gain adaptive immunity from vaccination. Since these vaccines are given intramuscularly they cannot provide the same immune function to the nasal passage where the initial infection occurs.
And we can get a brief hint of this from Shakya et. al. 2016:
The delivery of vaccines across mucosal surfaces has the potential to stimulate synthesis of pathogen-specific mucosal immune responses [2–4], but the conventional systemic delivery of vaccines against infectious diseases using a needle and syringe is unable to induce a strong mucosal immune response. Mucosal immune responses are important because the pathogen-specific antibodies that are stimulated by mucosal vaccination get secreted into the mucus where they can neutralize the pathogens even before they can cause infection.
So how do we make sense of all this?
Adding Context
During the initial stages of the infection the nasal passage is the first target. Here, people who have not had a previous infection and those who have been vaccinated will be on the same footing; their mucosal immune system will be naïve to the infection and will take some time to mount an immune response.
As the infection progresses and makes its way to other parts of the body the immune system of those who are vaccinated will be able to respond immediately, while those unvaccinated will still need time before an adaptive immune response occurs.
Because vaccinated individuals are trained to target the spike protein, their T and B cells can clear out the virus before large viral replication can occur. Unfortunately, this also means that it doesn’t provide the immune system of the vaccinated the ability to learn and create an immune system to other parts of the virus, while someone who is unvaccinated will have to deal with the larger levels of viral replication by creating a broader adaptive immune response.
The end result is that those who are vaccinated should hypothetically be able to clear systemic infection before an unvaccinated, previously uninfected person. However, because both should have started with naïve mucosal immune systems, both should hypothetically now have broadscale immunity within their nasal passage against the virus.
This highlights something extremely important; previous infection, whether vaccinated or not, should illicit strong, broad immunity within the nasal passage where the initial stages of the infection occur, meaning that both groups should be able to fight off future infections a the most important part of the infection.
The dichotomy between the systemic immune system and the mucosal immune system is one of the most overlooked parts of this whole pandemic and indicates why the entire testing procedure has been absolutely botched.
I previously indicated that even people who have been fully vaccinated had very low Ct Counts when tested using RT-PCR procedures. This would indicate that they have very high viral loads within their nasal passage, but this fits with the notion that the mucosal memory of vaccinated people would not be able to mount an adaptive immune response to target the virus within their noses. However, if the infection tries to make its way deeper into the body the system adaptive immune response should be able to target the virus, which is why people who are vaccinated have reduced symptom duration.
By not interpreting what a high viral load in vaccinated individuals mean when they get their noses swabbed, we’re missing out on the nuances between viral infection and testing procedures.
We’re using nasal swabs to indicate infection when this only indicates what’s happening in the nasal passage, while we are also using seroprevalence (antibodies in the systemic immune system) to indicate someone’s immune status. Not only are these not interchangeable, but it also indicates that we have clearly misinterpreted the way we examine all of this information!
The immune system is complex- far more complex than we give it credit for- and when we look at the way we have approached testing and vaccines we completely overlook the dynamics that take place during an infection.
What does the UK Report Mean, and does it Matter in Context?
So yes, the report does indicate that systemic immunity in vaccinated individuals will have difficulty in learning other parts of the virus during an infection (note that it doesn’t indicate how much lower N antibody titers are), but there’s so much more than what is being presented that needs to be taken into account.
Mutations in the spike protein may be a concern if it eludes systemic infection in vaccinated individuals, but even if previous infection does not produce systemic antibodies against proteins like the N protein, the mucosal memory should have broader adaptive immunity and prevent later infections from taking hold since this area remains relatively unaffected by IM vaccination.
PCR and Antigen tests tell us what’s happening locally (in the nose). They do not tell us what’s happening within the body.
Likewise, antibody measures work the same way; they don’t tell us what’s happening in the nose during the initial stages of infection, and interpretation of both should take this into account.
Hypothetically, people who have been infected, irrespective of vaccination status, should have robust mucosal immunity and should be better protected against future infections as well as reduced viral transmission.
Also hypothetically, people who have been vaccinated should be able to prevent systemic viral spread more quickly than unvaccinated, previously uninfected people because their systemic adaptive immune systems have already been trained to do so.
Systemic immunity should be treated differently than mucosal immunity, and both should be taken into account when contextualizing testing, infection, and vaccination data.
The discussion around COVID should always highlight the complexities and nuances of the entirety of the situation. This is where the largest faults of the pandemic response arise from; generalized, one size fits all responses have done us absolutely no good during this pandemic. It removes any notion of nuanced approaches to therapies, testing, or even preventative measures.
It is this parochial, simplistic nature that has invaded the science and medical community and is now used as a bludgeoning tool to target dissenters who want more diverse, nuanced discourse about this pandemic. Questioning the science, and questioning the evidence are the epitome of scientific rigor, and if we are to truly deal with this virus we need to understand the information and contextualize it as best we can.
But we also need to make sure we understand what information is being presented to us, and come at it with the idea of interpreting and contextualizing the information. It’s the ability to piece the information together, the ability to engage in sensemaking that should drive us when we examine the data. If it doesn’t make sense, we need to argue why this may not make sense by using rational, sensemaking processes before we resort to histrionics.
The goal should not be to examine information in a bubble, but to build upon previous knowledge, use it to examine new information, and rationalize how to connect both to one another, especially before we resort to paranoia and histrionics.
Note: I have used systemic immunity to differentiate it from mucosal immunity, even though systemic may be used in other contexts to refer to the entire body.
Thank you for reading my newsletter. If you enjoy my articles please consider becoming a free subscriber in order to receive notifications.
And share with others who may find these newsletters interesting.
Also, please consider becoming a paid member. The research and work put into these articles takes many hours and being a paid subscriber allows me to continue to do this full time.
In-Text Citations:
U.K. Health Security Agency. COVID-19 vaccine surveillance report Week 42. Taken from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1027511/Vaccine-surveillance-report-week-42.pdf
Surjit et. al. 2008. The SARS-CoV nucleocapsid protein: A protein with multifarious activities. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7106238/
Shakya et. al. 2016. Mucosal Vaccine Delivery: Current State and a Pediatric Perspective. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5381653/
Apparently the Pfizer vaccine at least does induce mucosal antibodies, whether the mucosa will exhibit OAS-like behavior or not independent of the systemic immune system? who knows; https://www.frontiersin.org/articles/10.3389/fimmu.2021.744887/full
Great read, thanks. How would an individual measure mucosal Ab / immunity? I’m previously infected (Apr 20). Vax Aug 21. N Ab through blood draw was measured as nil in Sep. S1 Abs were very high. I’m familiar with N Ab rapid decline studies and 20% non N responders. Thanks in advance.