


Bad Science Journalism- Niacin and the risk of MACE
Apparently many studies with poor methodologies have been coming from the Cleveland Clinic...

In reporting on the problematic xylitol study last week I was reminded of a study that came out a few months ago in which there were reports that Niacin, a B vitamin commonly found in fortified foods and available as a supplement and prescription was also related to increased risk of MACE leading to similar headlines as the xylitol study as can be seen below:



If this is ringing all too familiar note that the niacin study1 is derived from a research endeavor conducted by the Cleveland Clinic headed by researcher Stanley L. Hazen whose name appears across all of these metabolomic studies.



Many similar names can be found across all these studies suggesting that these studies are derived from the same team. However, Hazen is argued to be the lead researcher, and in fact his Cleveland Clinic profile notes that his focus is on metabolomics research and finding out what factors are associated with increased risk of cardiovascular disease:
A renowned physician scientist, Dr. Hazen has made pioneering discoveries in new understandings of mechanisms contributing to cardiovascular and inflammatory disease research. He is credited with numerous seminal discoveries linking gut microbial pathways to cardiovascular disease pathogenesis, as well as enumerating the role of myeloperoxidase and other inflammatory and oxidative pathways in cardiovascular disease. Dr. Hazen is among the top 0.1% cited researchers in the world with over 140,000 citations. He has published over 475 peer-reviewed articles in top tier basic and clinical journals alike in the fields of atherosclerosis, lipoprotein metabolism, gut microbiome, inflammation, vascular biology, and other topics related to preventive cardiovascular medicine. His research in multiple areas has impacted clinical practice, and lays the foundation for FDA- and EU-cleared diagnostic tests for cardiovascular disease risk assessment in use worldwide. He is listed as inventor on over 100 patents, and his research has helped to spawn pharmaceutical development of cardiovascular disease drugs in clinical trials.
By all accounts he seems like an accomplished researcher...
The point here isn’t to hammer Hazen on his accomplishments but to note his field of work which appears to be related to metabolomics.
Metabolomics is a newly emerging field, although the concept is something that would appear rather obvious. Metabolomics involves researching metabolites sourced from individuals and seeing how they correlate to various diseases. For instance, in cases of cancer or diabetes certain metabolites may appear elevated and thus may suggest a link between the two variables. In this case much of the Cleveland Clinic’s studies above are an examination of a multitude of metabolites and seeing which ones appear to correlate with future MACE.
However, one of the problems with metabolomics is something that tends to be a general egregious pitfall in scientific research. That is, finding elevated metabolites may not provide any meaningful data aside from correlative findings.
Put another way, one egregious issue in correlative research is the fallacy:
If detected, then pathologize.
Just because certain metabolites appear elevated in diseased states does not mean that the disease itself is the source of the metabolite. In many cases medications related to a disease, diet, and other factors are likely to elevate metabolites at the same time that a chronic disease or illness is occurring.
This creates a challenge as metabolomic findings may not translate well in a clinical setting as targeting of elevated metabolites may not lead to actual clinical benefit. Issues with pre-analytical sample collection, sample analysis, and interpretation all can bias metabolomic findings as well.
For those curious of metabolomics research take a look at a few of the citations below:
Chen, et al.2: Guide to Metabolomics Analysis: A Bioinformatics Workflow
Li, et al.3: Challenges in the Metabolomics-Based Biomarker Validation Pipeline
More poor methodology from the Cleveland Clinic

So far I’ve highlighted pitfalls with two prior studies that seem to have come from Hazen/the Cleveland Clinic’s team, so it shouldn’t be surprising that similar pitfalls appear within the current niacin study as well.
I won’t go over the methodologies again as it would be redundant (refer to prior articles) so we will focus on the issues. In short, researchers did not look at niacin levels from those within a discovery cohort but instead looked for niacin-related metabolites called 2PY and 4PY as it was believed that a metabolite of unknown structure with a mass/charge ratio of ~153 was found and alleged to be a mixture of both 2PY and 4PY.4
When categorizing participants within the discovery cohort into quartiles based upon alleged 2PY and 4PY levels the authors noted a greater rate of MACE among individuals within the 4th quartile relative to those within the 1st quartile:
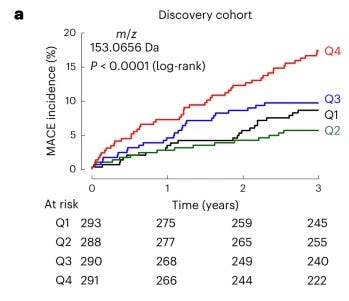
At this point readers will hopefully know that there should be some things going on here that are worth criticizing. For instance, the first question readers should be considering is the demographic makeup of participants within each quartile. Note that within the studies for Xylitol and Erythritol the Q4 group was generally less healthy and had a higher rate of previous cardiovascular events, suggesting that prior medical histories may correlate with future MACE.
Unfortunately, the researchers didn’t provide any demographic data for us to assess in this Niacin study for some reason, and only provided baseline demographic data as broken down between Discovery Cohorts and Validation Cohorts, which begs the question as to what other variables could attribute to such an egregious dichotomy between the Q4 participants and the other quartiles.
And also, similar to the other studies one should ask what level of these alleged niacin metabolites are, and where the niacin may have come from. Again, here the researchers are not clear regarding the niacin metabolite contents of each quartile. They don’t even mention any surveys or examinations of participant dietary niacin sources.
Instead, the only comment provided by the researchers suggests that validation cohort participants were excluded if they were found to have taken prescription niacin supplementation in the past:
For the present studies, in the US validation cohort, individuals with evidence of (prescriptive) niacin use at time of enrollment or within the preceding 30 d were excluded.
So, this again doesn’t tell us how much niacin people were obtaining from diets or supplementation. However, the researchers do mention the lack of reporting dietary niacin as being a limitation:
We also recognize that clinical observational studies by design show only association and not causation; thus, there always exists the possibility of unmodeled confounding that may have impacted our results through factors that are not included in our models (for example, we have no information on dietary niacin intake).
It’s once again another point of frustration given that all these studies have been reported as tying a dietary agent to cardiovascular risk even though the researchers neither examined dietary consumption of these products. The xylitol study is even more egregious as the researchers themselves point out that elevated xylitol levels had to have come from endogenous production of xylitol and not from the diet contradicting all the reports on the xylitol study!
It must be reiterated that if researchers can’t even quantify how much of an allegedly harmful substance participants consumed can they really make any claim tying such substances with cardiovascular damage? And why have so many journalists taken to running with a link that researchers were not able to tie together themselves?
But this is made even worse given that the Discovery Cohort was examined for untargeted metabolomics study. In the case of untargeted metabolomics no definitive metabolite is looked at as being tied to a disease, but instead elevated metabolite levels are screened for correlations. In this case anything that appears to correlate is then tested mechanistically both in vivo and in vitro for possible mechanistic explanations, but remember that such research may not actually lead to anything clinically meaningful.
This is where the comment on confounding variables is critical, because the researchers note several elevated metabolites that appear to correlate with increased risk of MACE:
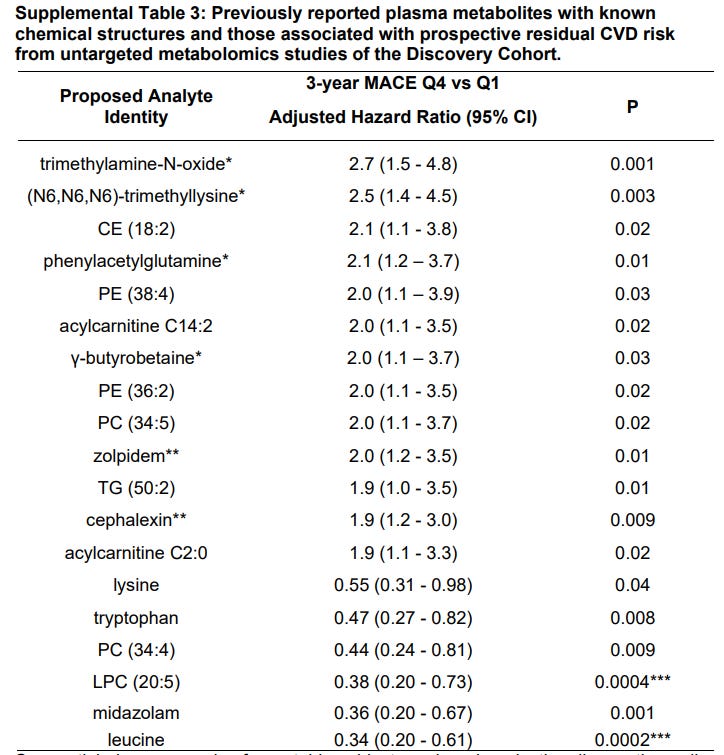
So although the researchers focused on niacin metabolites in particular for this research it’s quite obvious that many other metabolites were also found to correlate with increased risk of MACE. Of course, this should seem rather obvious given that we have two prior studies on non-nutritive sweeteners which allege a link between erythritol and xylitol levels with risk of MACE.
So if many different compounds appear to correlate with increased risk of MACE why aren’t these compounds mentioned, and why is there no explanation provided regarding their relationship to one another?
To be fair, I should state that any compound with an asterisk were alleged to relate to increased risk of MACE as reportedly Hazen’s team in prior studies. In particular, Trimethylamine-N-oxide is argued to be a gut bacteria-related metabolite from choline and betaine, which are generally found in red meat.5 In fact, the prior metabolomics studies were one of the pivotal works in creating the paranoia over red meat and cardiovascular risk.
Interesting that this would be yet another diet-related compound that is being fear mongered over due to work related to the Cleveland Clinic and Hazen’s team…
But what stood out to me were two compounds listed on the above table with two asterisks:
Zolpidem, better known as the sleep aid Ambien
Cephalexin- a common antibiotic
So among this stew of metabolites that appear to correlate with increased risk of MACE we also have two prescription medications that also correlate.
Again, why is this not mentioned by researchers, and how many patients were on these medications? But more importantly at the point that medications are being correlated with future risk of MACE shouldn’t some pause be taken to question whether any of this correlative data leads to anything meaningful?
Note that Cephalexin being an antibiotic would likely mean that any use of the drug would likely be short term, so how exactly can a drug with limited use predict MACE in the years following?
Remember that the researchers never took routine blood samples for metabolomic research- all of the correlative calculations were based on blood samples collected at the time of recruitment.
Like with many studies before such as a fish oil study I covered earlier, remember that plenty can change in a matter of years. Can one readily predict the behaviors and lifestyles of individuals based on a blood sample taken years before, especially when the dietary behaviors of those individuals are not known?
Squeezing out every correlation
In covering this study it should be appear obvious that something strange seems to be afoot.
Here we have several studies which appear to be tying various compounds with increased risk of cardiovascular disease, and yet in every instance it appears that no diligence was taken in recording the actual dietary intake of these compounds or what other variables could lead to increased levels of these implicated compounds.
Taken independently these studies would already be worthy of scrutiny. However, because these studies appear to be coming from one research team in particular something even more concerning should be considered.
Note that across both the non-nutritive sweetener studies, this niacin study, and the prior TMAO study all point to one clinical trial in particular:

Although the clinical trial mentions nearly 10,000 recruited participants what’s interesting is that the Discovery Cohort across all 4 studies are similar as they either mention a total of 1157 or 1162 participants among their Discovery Cohorts.
I should caution that some assumptions are being made here, but given that these research endeavors involved untargeted metabolomics (i.e. researchers didn’t know what they were looking for) and utilized a Discovery Cohort (i.e. a group to find metabolites and correlations) it makes it very likely that the Discovery Cohort used across all 4 studies is likely made up of the same participants.
Or put in another way, it would then suggest that this Discovery Cohort was essentially screened for any possible correlation and anything that seemed to show some sort of correlation was then made into its own study.
This approach actually is not uncommon, although it doesn’t make for good science. You are likely to come across various studies in which one pool of participants are just assessed in any way possible in order to find something that can be made to correlate.
In fact, this is why we tend to get a bunch of nonsensical correlative studies to begin with, as researchers may just try to view a specific dataset in any way possible that can provide them something to publish.
Taken altogether these studies don’t appear to be much more than a fishing expedition to see what type of metabolite may stick correlatively. Bear in mind that if this same Discovery Cohort is used across all 4 studies then each study would inherently contradict each other due to the fact that each separate metabolite would be a confounder for the other.
Unfortunately there seems to be even more going on here but I’ll save it for another post in which I raise some questions regarding why these sorts of studies are being conducted in the first place.
Prior Studies for those interested…
Bad Science Journalism- Xylitol and risk of MACE

The media has taken to propagating more fear porn in the case of sugar substitutes. This time xylitol- a sugar alcohol found naturally in fruits and as an additive artificial sweetener in gum, toothp…
Does Erythritol increase heart attack and stroke risk?

Most of my articles remain free to allow for open access to the information provided. However, given that Substack is the main way I am supporting myself (for the time being) I release occasional posts for paid members to encourage support. Please consider becoming a paid member or supporting me through my
Is fish oil harmful to your heart?

Edit 6.1.2024: Grammatical changes were made in one sentence below. The sentence that was changed now states the following: For one, the researchers didn’t take into account how much fish oil people w…
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Ferrell, M., Wang, Z., Anderson, J.T. et al. A terminal metabolite of niacin promotes vascular inflammation and contributes to cardiovascular disease risk. Nat Med 30, 424–434 (2024). https://doi.org/10.1038/s41591-023-02793-8
Chen, Y., Li, E. M., & Xu, L. Y. (2022). Guide to Metabolomics Analysis: A Bioinformatics Workflow. Metabolites, 12(4), 357. https://doi.org/10.3390/metabo12040357
Li, S., Looby, N., Chandran, V., & Kulasingam, V. (2024). Challenges in the Metabolomics-Based Biomarker Validation Pipeline. Metabolites, 14(4), 200. https://doi.org/10.3390/metabo14040200
Elaboration on this discovery metabolite is outside the scope of this paper. Note that this dives into analytical methods such as mass spectrometry and therefore would take even more time to explain. Thus, for the meantime I have taken to assuming that the researchers were able to find this mixture of 2PY and 4PY.
Li, X. S., Wang, Z., Cajka, T., Buffa, J. A., Nemet, I., Hurd, A. G., Gu, X., Skye, S. M., Roberts, A. B., Wu, Y., Li, L., Shahen, C. J., Wagner, M. A., Hartiala, J. A., Kerby, R. L., Romano, K. A., Han, Y., Obeid, S., Lüscher, T. F., Allayee, H., … Hazen, S. L. (2018). Untargeted metabolomics identifies trimethyllysine, a TMAO-producing nutrient precursor, as a predictor of incident cardiovascular disease risk. JCI insight, 3(6), e99096. https://doi.org/10.1172/jci.insight.99096
I probably missed it, but what is MACE?
It's so strange that the basics of science aren't even followed, like controlling for confounders. I guess that might happen in preliminary studies, but the media spreads their results as if they have more validity than they do. (As you said in this stack). In my twenties and thirties I would follow some of this dietary advice without thinking of going to the original scientific studies! 🤪 It's only in the past 10 years that I recognized how much studies are misrepresented in the media. I look forward to hearing your thoughts on possible reasons behind studying these things, does it have to do with genes? I'm hearing about a shift towards genetic causes of disease, and more genetic solutions. 🤔
I think there's so much we don't understand about this miraculous complex biological system that is our body. It may be hard to design a study well for such a complex system.