

Bad Science Journalism- Xylitol and risk of MACE
Why headlines suggesting that non-nutritive sweeteners can cause heart attacks or strokes are misleading and based on poor science literacy.

The media has taken to propagating more fear porn in the case of sugar substitutes. This time xylitol- a sugar alcohol found naturally in fruits and as an additive artificial sweetener in gum, toothpaste, and various food products- is the one to be hit by a new wave of media concern due a new study published last week.1

Which has led to headlines such as the ones below:



“Study finds” as some of these headlines go, but what did this study really find?
One of the many reasons I have lambasted mainstream outlets is their lack of investigation and looking into the studies that they are covering. Instead, they repeat the same talking points as one another, leading to the false assumption that a study may find something that may not actually be there- and this is unfortunately a clear case of this occurring.
Key Findings
This recent study comes from the same group of researchers at the Cleveland Clinic who put out a study on erythritol and MACE which I covered last year.
Does Erythritol increase heart attack and stroke risk?

Most of my articles remain free to allow for open access to the information provided. However, given that Substack is the main way I am supporting myself (for the time being) I release occasional posts for paid members to encourage support. Please consider becoming a paid member or supporting me through my
In this case the researchers looked at over 3,000 elderly participants who visited clinics for cardiac evaluations. The cohort was separated into two groups- A Discovery Cohort comprised of 1,157 participants enrolled between 2001 and 2003 as well as a Validation Cohort comprised of 2,149 participants enrolled between the years of 2003 and 2005.
The Discovery Cohort had blood drawn and plasma examined for polyols- in this case the researchers looked for the isotope with the composition of C5H12O5 which was considered to be xylitol, and grouped participants within the Discovery Cohort into tertiles2 based on plasma xylitol levels.
Participants were then evaluated at the 3-year follow-up mark and were examined for any incidents of MACE. This study was also replicated with the Validation Cohort in order to confirm the results of the Discovery Cohort.
Altogether, the authors noted that those who had incidences of MACE within the 3 years appeared to have higher levels of xylitol within their plasma, and this appeared to be the case among both the Discovery Cohort as well as the Validation Cohort.
However, note that some of these results are very sporadic, and quite frankly raise a few questions.
For one, note that the relative levels of what is assumed to be xylitol don’t appear to be magnitudes different between those who experienced MACE and those who didn’t:
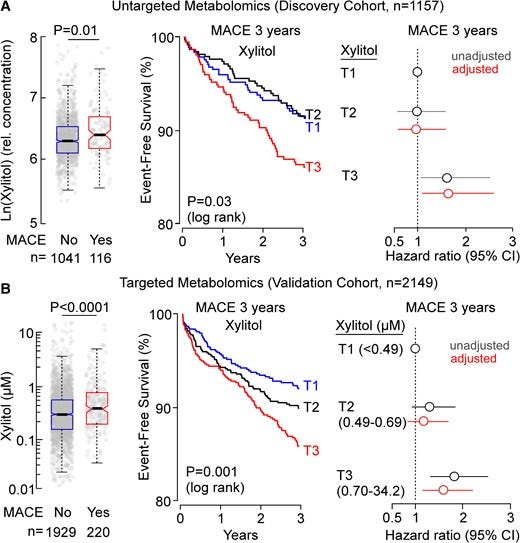
The plots on the left compare xylitol levels among those who didn’t experience MACE within the 3-year period to those who did. The top plot looks at those within the Discovery Cohort while the bottom looks at those within the Validation Cohort.
Note that the units here are not consistent between the Discovery Cohort and the Validation Cohort. The Discovery Cohort appears to use a natural log measure for their concentrations. There’s no indication for how the measures were found for the Validation Cohort, but if assume it also follows a natural log calculation then why is there such a discrepancy between the two cohorts? If different calculations were used why are the units different? Not only does it make it difficult to compare the two plots, but it also raises a question of why a lack of consistency is being used here.
But even among the people who experienced MACE and those who didn’t it doesn’t appear that the average xylitol levels different vastly between the two groups (although there seems to be a huge degree of interpersonal differences among people from both groups). This can also be seen within the tertile cutoff groups that appear for the hazard ratios of the Validation Cohort.
Note that the breakdown of the tertiles are as follows for the Validation Cohort:
T1: [Xylitol] < 0.49
T2: 0.49 < [Xylitol] < 0.69
T3: 0.70 < [Xylitol] < 34.2
So, there’s an apparently huge margin for the T3 group that isn’t seen with the other groups. How many people within the T3 group had extremely high Xylitol plasma concentrations, and would that bias the results of this study?
And what’s rather striking is that, at least within the Discovery Cohort, it appears that those who were within the T3 tertile had far higher rates of previous MACE and other cardiovascular-related events as compared to the other tertiles, especially when it comes to myocardial infarctions and heart failure:

So not only was the range of xylitol within the T3 tertile extremely wide they also had higher rates of prior cardiovascular events.
Remember that the people included in this study were people seeking out some sort of cardiovascular evaluation. Cardiovascular-related events are also more likely following any initial event, and therefore isn’t quite possible that the higher rate of MACE events among those within the T3 tertile related to having a higher previous incident of MACE to begin with, and thus leading these people to seek out evaluations in lieu of prior incidents?
It's also important to consider a reversal of correlation here- people with higher xylitol levels may not be more predisposed to cardiovascular events, but that cardiovascular events may result in some sort of cellular dysfunction that may cause one to have elevated levels of xylitol.
Again, the relative concentration of xylitol between the MACE and non-MACE groups don’t seem particularly different. But also take into account that xylitol is also derived from fruits and vegetables, and we produce xylitol naturally as part of our general metabolism. All to say that xylitol within the body isn’t all too uncommon, but what’s important is understanding what sort of baseline measure of xylitol generally healthy people have, and what influence dietary xylitol consumption can have on these levels.
This brings us to probably the most egregious part of this study as it essentially contradicts every claim being spouted by mainstream outlets.
Where did the Xylitol come from?
In order to assess effects of dietary xylitol on xylitol plasma levels researchers recruited 10 healthy individuals. Unlike the people who made up the Discovery and Validation Cohort these individuals were nearly 30 years younger (mean age 30) and had no prior cardiovascular disease and diabetes.
These individuals were provided water sweetened with 30 grams of xylitol3 and had blood drawn at various timepoints and measured for xylitol plasma levels. Note that 4 participants had their xylitol levels measured over the course of 24 hours while the other 6 individuals only had measures taken at baseline and at 30 minutes post-sweetener consumption.
Within the first 30 minutes of being provided the sweetened water there was a noticeable spike in xylitol within the plasma of individuals- nearly a 1,000 fold increase that is mentioned several times across many news articles.
However, note within a few hours xylitol levels within the body drastically declined among the 4 evaluated participants, and by the post 6-hour mark levels seemed to even out with baseline measures:
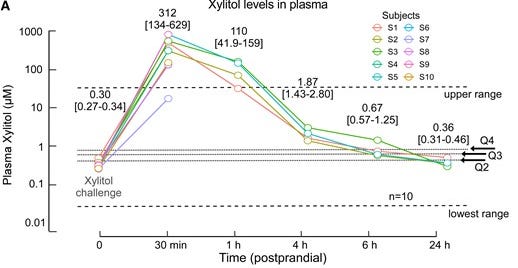
This essentially suggests that although xylitol levels may drastically spike within minutes of ingesting xylitol the levels quickly decline over time.
Now, why exactly is this important?
This is important for the simple fact that the blood drawn from those within the Discovery and Validation Cohorts were done within a fasting state. That is, these participants didn’t have any food more than 12 hours prior to having their blood drawn:
Plasma levels monitored in both the discovery cohort and the validation cohort were following overnight (>12 h) fast.
Although we may have to consider the half-life relevance of xylitol what this essentially means is that the allegedly elevated xylitol level of those within the Discovery and Validation Cohorts cannot have come from consumption of xylitol because most of the xylitol would have cleared their bodies by then.
This is made clear by the portion of the study utilizing the 10 healthy volunteers, and is also emphasized by the authors in which they suggest that elevated xylitol levels in both Cohorts had to have been derived from endogenous production of xylitol and not from food:
The rapid rate of xylitol excretion observed in healthy volunteers with return to near baseline (fasting) levels within hours following ingestion of a significant dietary exposure suggests that the plasma levels observed in our observational (validation) cohort represent variations in endogenous production/levels and not food intake.
And is further expounded upon within the Discussion portion:
One topic that deserves further discussion is the relationship in the large-scale clinical observational studies performed associating plasma levels of xylitol with incident risks of MACE and dietary exposures to xylitol. The present studies, we believe, argue that the observed associations noted in the discovery and validation cohorts reflect endogenous xylitol levels (steady state between endogenous production and excretion) and not recent dietary exposure. First, while a limitation of the present studies is the lack of any information on xylitol dietary exposure in the clinical observational cohorts, given the speed with which we observe xylitol is excreted (i.e. half-life of elimination was ∼15 min, and post-prandial plasma levels in healthy volunteers, despite reaching 1000-fold increases, return to near baseline levels within 6 h; Figure 2A), the fasting (>12 h) plasma levels monitored in the discovery and validation cohorts likely represent endogenous levels of xylitol production. Second, the enrolment of subjects in the validation cohort largely predates the more recent increases in dietary exposure to xylitol in processed foods.
Here the authors go on to note that xylitol is produced through an alternative glucose metabolism pathway via the glucuronic acid pathway. Although it’s not clear what relationship this pathway may have with MACE it’s possible that any elevated xylitol level noted within these participants may reflect some sort of metabolic dysfunction more than anything pertaining to dietary consumption of xylitol. Again, remember that the people included within this study were older and had multiple comorbidities including diabetes and cardiovascular disease.
Therefore, it wouldn’t be surprising to assume that elevated xylitol levels may run downstream of other issues occurring within these people’s body’s and may not be the pathological agent in question.
That’s besides the point for now, as what’s more important is pointing how off the mark the reporting of this study has been among those in the media who seem to be going off of the idea that the incidences of MACE within these individuals have to have been derived from consuming sugar alcohols rather than some other underlying factor.
Note that the researchers never mention how much sugar alcohol these participants consumed to begin with, so we don’t even have any baseline measure for dietary exposure to xylitol. If we can’t even determine if these participants were consuming xylitol to begin with, how can we claim that their allegedly elevated xylitol levels were derived from xylitol-sweetened products?
There’s so much discrepancy between what the study suggests and what is being reported, and yet people seem to ignorantly question why people are losing trust in both the media and among scientists.
There are obviously egregious issues with this study and given the methodology there’s no clear way to tie xylitol consumption with cardiovascular events.
And remember when I said that the xylitol levels of those within the Discovery and Validation cohorts didn’t seem particularly high? Take a look at the graph for the healthy volunteers and focus on the dashed lines marked “upper range”, “lower range”, and “Q2”, “Q3”, and “Q4”.
Those lines are not associated with the healthy volunteers but instead are based on fasting xylitol levels from those within the Validation Cohort. For the different quartiles the lines represent the bottom boundary for the quartile, essentially meaning that around half of the people within the Validation Cohort had xylitol levels below 1 uM.
And so, given this context don’t the baseline measures for both the Validation Cohort as well as the healthy volunteers seem comparable? Aside from outliers a good portion of the Validation Cohort xylitol levels appear to hover around the baseline levels of the volunteers.
This is why it’s important for researchers to be explicit in their work otherwise it can easily confuse readers or lead to misinterpretations of the work.
Nothing but bad journalism
This is unfortunately one of a growing list of studies in which the media fails to accurately report on the findings of a study. It’s an ever-growing sign that journalists lack scientific literacy and critical thinking, rushing to report on whatever they find or basing their articles on whatever misinformation is being spouted by other outlets. It shouldn’t come as a surprise that nearly all the articles reporting on this xylitol study hit the same beats, with the only caveat provided being the banal phrase “correlation does not mean causation”, as if to obfuscate the lack of investigating for some out in case the study is not actually of merit.
It's important to remember- just because researchers publish a study doesn’t mean that the researchers were able to reach the conclusions they are claiming. The study here in no ways can tie consumption of xylitol to incidences of MACE because the people who were being examined weren’t being evaluated for their xylitol consumption. We don’t know how many participants were consuming xylitol products, many of these participants also had prior comorbidities, and the fasting prior to blood collection removes the tie between dietary xylitol and allegedly elevated xylitol levels as it appears that the elevated xylitol levels may be related to some sort of metabolic dysfunction within the body.
The only possible lead provided by the study is the elevated prothrombotic state among healthy individuals after consuming xylitol-sweetened water, but even this finding would only be reflective of an increased risk of MACE in the immediate aftermath of consuming xylitol and not a long-term risk assessment of constant consumption of these products, and unless researchers conduct a study to see if xylitol consumption is immediately followed by increased risk of heart attacks or strokes this association is still a tenuous one.
But let’s suppose we entertain the idea that sugar alcohols may increase the prothrombotic state of our bodies. When considering this hypothesis, it’s best to consider some sort of frame of reference i.e. compared to what?
Given that these sugar alcohols are intended to replace dietary sugar it’s best to see if sugar is associated with some sort of prothrombotic state.
Indeed, it appears that researchers are examining the link between diabetes, fasting glucose levels and the possible increased risk of thrombosis.4,5 As it seems people who are Type II diabetes are at increased risk of venous thrombosis, and there also seems to be a relationship between glucose and biomarkers related to coagulation.
This appears to be reflected in a rather apt study from 2019 in which elevated fasting glucose levels, as well as glucose levels within the postprandial state seem to be associated with increased factors related to coagulation.6
I haven’t evaluated any of this information so keep in mind that this information may be inaccurate. Nonetheless, it’s interesting to see that researchers were examining whether glucose itself may be associated with a prothrombotic state, suggesting that this prothrombotic effect may not be unique to sugar alcohols.
In some ways this makes sense as sugar alcohols are structurally similar to monosaccharides with the only difference being that sugar alcohols lack aldehyde functional groups and therefore can’t arrange itself into a ring form (sugar alcohols remain linear). Therefore, it’s possible that the prothrombotic nature of sugar alcohols may rely on similar pathways as that of typically found monosaccharides such as glucose and fructose.
So within a broader context many sweeteners whether natural or artificial may be associated with increased risk of a prothrombotic state. In which case the best option may be to reduce sweet items irrespective of the source.
But that is an aside for another time.

If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Marco Witkowski, Ina Nemet, Xinmin S Li, Jennifer Wilcox, Marc Ferrell, Hassan Alamri, Nilaksh Gupta, Zeneng Wang, Wai Hong Wilson Tang, Stanley L Hazen, Xylitol is prothrombotic and associated with cardiovascular risk, European Heart Journal, 2024;, ehae244, https://doi.org/10.1093/eurheartj/ehae244
Tertiles referring to separating groups into thirds unlike the typical quartiles which is fourths.
The authors suggest that this level of xylitol is equivalent to what one may find in a pint of xylitol-sweetened ice cream, baked goods, or several pieces of xylitol-sweetened candies.
Lemkes, B. A., Hermanides, J., Devries, J. H., Holleman, F., Meijers, J. C., & Hoekstra, J. B. (2010). Hyperglycemia: a prothrombotic factor?. Journal of thrombosis and haemostasis : JTH, 8(8), 1663–1669. https://doi.org/10.1111/j.1538-7836.2010.03910.x
Grant, P.J. (2007), Diabetes mellitus as a prothrombotic condition. Journal of Internal Medicine, 262: 157-172. https://doi.org/10.1111/j.1365-2796.2007.01824.x
van der Toorn, F. A., de Mutsert, R., Lijfering, W. M., Rosendaal, F. R., & van Hylckama Vlieg, A. (2019). Glucose metabolism affects coagulation factors: The NEO study. Journal of thrombosis and haemostasis : JTH, 17(11), 1886–1897. https://doi.org/10.1111/jth.14573
My assumption from this sudden tantrum about Xylitol is that Pig Pharma/Medical Iatrogenic Complex (MIC) has decided to give it the Ivermectin treatment. Xylitol is well known in dentistry as an effective anti-bacterial/viral and a small family producer has done some studies showing that a nasal spray with Xylitol can be effective in reducing SARS-Cov2 viral load in nasal tissues. But of course, when they started marketing the actually safe and effective treatment/preventive, FDA came down hard. I don't know the outcome of their fight with FDA, but all this BS falls right into the same line. As an additional "kill the messenger" argument, Cleveland Clinic, based on a quick internet browse, appears to still be shilling for mRNA vexxes. For me, that's enough to eliminate any credibility they ever had on any and every topic.
While you show this wasn't even considering actual dietary intake, even if those with heart issues were eating a lot of xylitol it could be precisely because they were avoiding sugar due to having heart issues.
In other news, umbrellas are linked to rain showers...