
Another IgG class switching study
Some more evidence of increasing IgG4 antibody levels, with some additional remarks on IgG2, IgA, and comparisons of methodology.

Edit: The word snuff has been changed for sniff, which changes the meaning a lot (no one is being snuffed!). Thanks to Faith for pointing that out.
To give my previous microbiome post some room to breathe I was going to release a post on the American Academy of Pediatrics new guidelines for childhood obesity.
However, the AAP doesn’t appear to take too kindly to people taking excerpts, so I scrapped that for now.
But that’s an aside. Yesterday Igor pointed out a hot off the computer article on another IgG4 study (as well as Unglossed and Naked Emperor at the time of this posting):

More news is good news, at least in the way of getting more information about this class switching and the severity of it.
The study in question was published in Frontiers in Immunology just yesterday, from Buhre, et al.1:

Unlike the Irrgang, et al.2 study published in Science this study took a look at factors such as IgA antibodies in both saliva and blood of patients, as well as galactosylation and sialylation, which are modifications to the Fc stalk of IgG antibodies.
We will return to the IgA portion later on, but the Fc stalk modifications will not be the focal point of this article (just noting it as something the researchers looked at).
But rather, as the title would suggest this appears to be another indication that IgG4 responses are occurring with these mRNA vaccines.
This study looked at various combinations of vaccinations, such as those who got only Moderna (n=25), those who only got Pfizer (n=48), those who got adenoviral vector from AstraZeneca (n=14), those who received heterologous vaccination (mixing of adenoviral and mRNA; n=12 for A+B, n=44 for A+M), and those who were previously infected and received vaccines of any kind as well (n=14; note some only received one dose while others received 2).
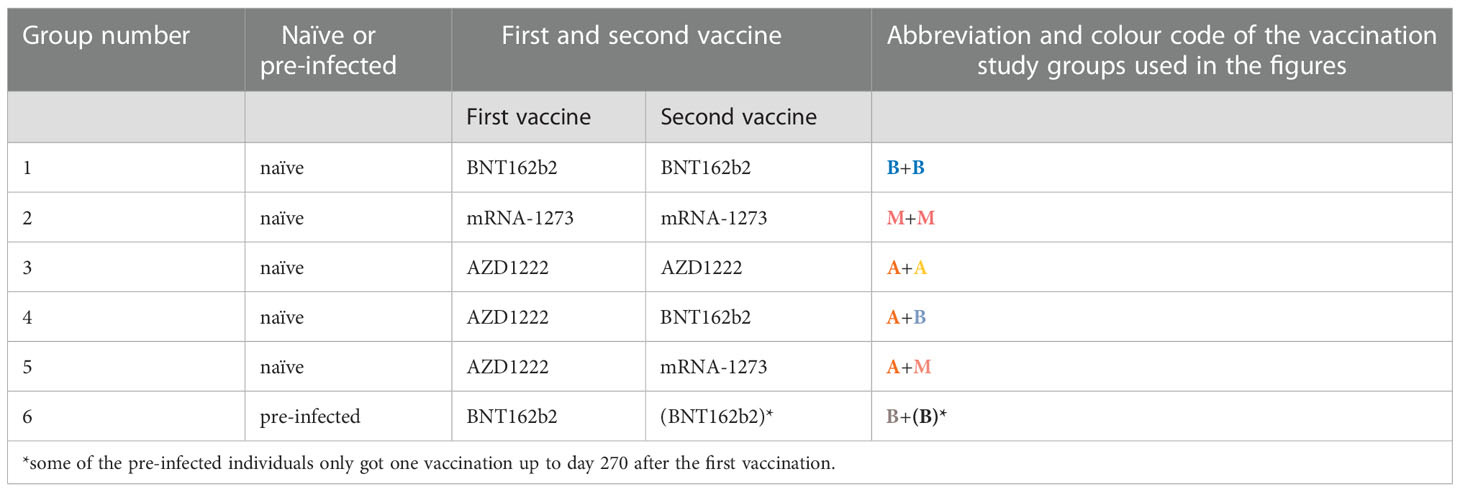
Note that boosters were not included in this study, and so it leaves us at a disadvantage in comparing the two datasets as it appears that IgG4 subclass switching is contingent upon repeat exposures. Also, the purely adenoviral vaccine group was small compared to the others and so differences in sampling size should be factored into the assessment.
The pertinent Figure that everyone is grabbing is the one below:
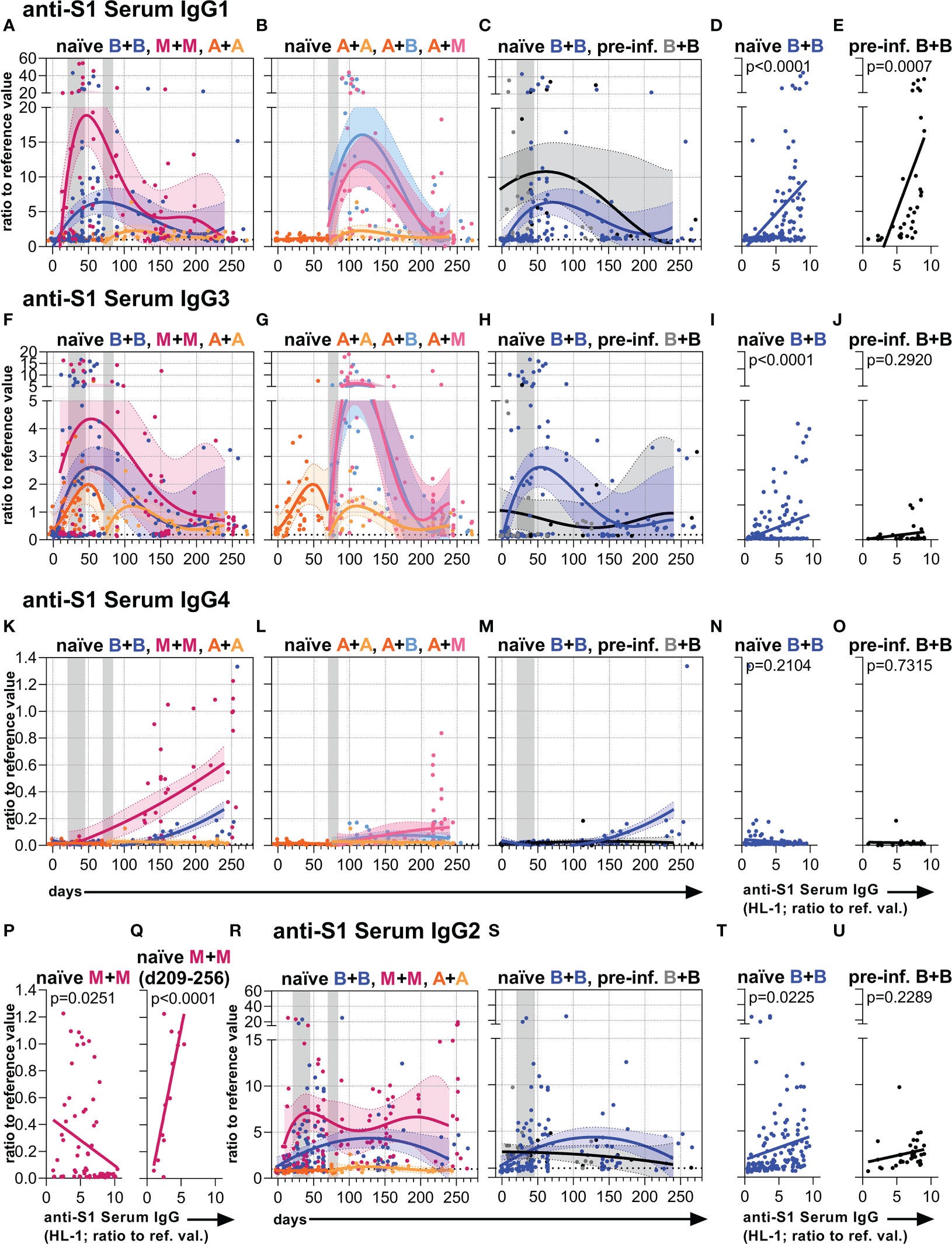
The Figure is organized by both IgG subclasses and vaccine types. Each row corresponds to one IgG subclass, with IgG1 noted at the top followed by IgG3, IgG4, and then ending with IgG2.
The first column shows the antibody responses for those given homologous vaccinations (they received two-doses of the same vaccine). The second column shows the response in heterologous vaccinees, with the homologous adenoviral vector vaccinees likely serving as a comparison. The third column compares those previously infected and received Pfizer with those who were not infected and received two-doses of Pfizer.
As can be seen given the curves, those who received the mRNA vaccines had the highest IgG1 and IgG3 responses that taper off near the end of the 270 Day timepoint (Figs. 2a, 2b, 2c for IgG1; Figs. 2f, 2g, 2h for IgG3).
But of course, the star of the show here is the IgG4 subclass, and if you look above you’ll note that it appears that the mRNA vaccines are leading to increasing IgG4 levels post-vaccination, and more importantly the effect seems greater among those given Moderna compared to Pfizer.

This is important since it tells us that there is possibly a dose-dependent response to the mRNA vaccines, such that higher doses are likely to lead to greater IgG4 class switching.
What’s also important to note is that this effect doesn’t appear to occur with those given the adenoviral vaccines, and even those given the Pfizer vaccines after infection don’t appear to have this issue, but remember to take into account the smaller sample size in the latter cohorts.
Again, the evidence here isn’t entirely comparable as the Irrgang, et al. study looked at those who experienced breakthrough infections in both 2-dose and boosted participants. Also, the Irrgang, et al. breakthrough cohort also comprises those who received a Moderna vaccine for their booster while the 2-dose cohort only received Pfizer, adding another confounder (Table S4).

In any case, the supposed breakthrough cases from Irrgang, et al. would suggest that the predisposition for class shifting may occur far early on within the development and maturation of memory B cells. That is to say, it’s possible that something within the mRNA vaccines may be inducing class shifting very early on during the response, although more research would be needed to sniff out exactly what mechanisms would be inducing such a shift, as it could just come down to high-spike being the key factor.
Overall, the evidence here does seem to add to the growing body about IgG4. However, this study only looked at those up to 2 doses of vaccines. Given the use of ELISA in this study it’s hard to argue what exactly the IgG4 would mean with respect to possible issues, as the actual percentage here is not known, nor is the percentage needed to induce dangerous pathologies.
It’s all relative
So IgG4 is being detected and appears to increase in the proceeding months post-vaccination. That raises some serious questions about what’s going on.
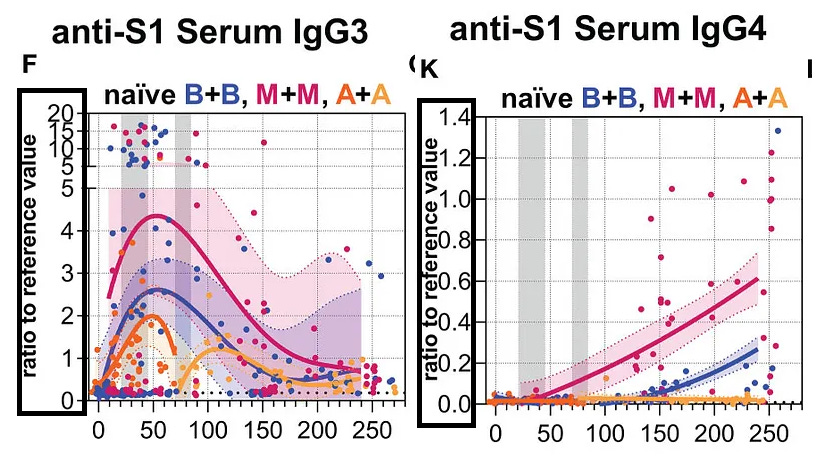
However, note that the scaling of the IgG assays are different.
Here’s a comparison of serum IgG3 for the mRNA vaccines and the corresponding IgG4 results:
The researchers in the Frontiers article used an ELISA (enzyme-linked immunosorbent assay) platform.
Although a bit technical, ELISA takes a membrane (usually a plate with wells) studded with proteins or some molecule, in this case the spike protein, and adds diluted serum to the membranes and has the IgG antibodies stick. A few more steps happen before results are given, but the important factor here is that in order to determine the amount of antibodies that stuck a reference control is looked at.
In this case, the fluorescence of the sample wells need to be compared to a control well to provide some relative measure of antibody quantity.
That’s where the “ratio of reference value” remarks above come sin. Put in laymen’s terms, values above 1 suggest a greater fluorescence intensity relative to the control, while values lower than 1 suggest a lower level than the control. I use fluorescence here as it depends on what control is used, and if it is a set number of antibodies then the inference would suggest a comparison of antibodies in samples to antibodies in the control.
So here, although the IgG4 graph is increasing over time the number of IgG4 antibodies still fall below the control number (again, depending on what the control was measuring).
This is all to say that you should be careful in looking at graphs or figures and suddenly inferring something based on the curves or lines alone. It’s easy to see the above figures side-by-side and assume that IgG4 levels may be outpacing IgG3 without looking at the scales and be reminded that the results are relative to the controls, and also should take into account the difference in scaling here.
What to do about IgG2
If we take a look at the results from Fig 2 you’ll note something interesting.
In the current discussion all of the IgG subclasses have been discussed except for IgG2, which has strangely been left out.
IgG2 is a pre-IgG4 antibody showing reduced effector function similar to the end-stage IgG4 antibodies, but not quite there yet.
Remember that the class switching goes IgG3 → IgG1 → IgG2 → IgG4.
Why IgG2 doesn’t get talked about much is something I’m unsure about. It could stem from the fact that the Irrgang, et al. study sort of downplayed its significance even though they noted a relatively high number of IgG2 antibodies across the timepoints (their text waffles around with the actual numbers).

This can also be noted within the Buhre, et al. study as well.

Again, note here the relativity of the ratios. In this case the IgG2 ratios appear higher than the other antibodies aside from IgG1, and so it raises questions as to why such a high level of IgG2 is being produced.
It’s important to remember that all of these curves are artificial, and constructed based on the samples. Sometimes it may be easier to look at the data as bars (note that the same graphs can be found for the other subclasses within the Supplementary Material):

Regardless of how you look at it, it does appear to be a high presence of IgG2 antibodies.
Now, this may suggest that the memory B-cells may be on their way to the final destination of IgG4, however as IgG2 antibodies have reduced effector function one may argue that the presence of these antibodies themselves are also a serious issue.
Previously, I’ve noted that IgG4-RD can be rather ambiguous, as in several cases there doesn’t appear to be detectable levels of circulating IgG4 within a patient.
However, some evidence suggests that IgG2 levels may be elevated in supposed cases of IgG4-RD3 where the levels of IgG4 appear normal.
So maybe we should be looking for IgG2-RD? But that's for others to speculate as I would need more evidence to make a remark.
Surprisingly, there’s an article from 2020 suggesting that COVID vaccine development should attempt to create IgG2 antibodies4, as the reduced activation of the complementary system and cascading events would mean less inflammation.
In any case, the current evidence would suggest that all of the subclasses and their behaviors should be looked at, as each play a critical role in our immune systems.
Again, it’s not just the events, but the process that matters.
IgA is worth examining for adverse reactions
Interestingly, the researchers in this study looked at both salivary and serum levels of IgA post-vaccination.
IgA is a class of antibody normally found within the mucous membranes and serum of individuals, and serves as a big player in protecting the body as it is one of the first antibodies to be released during the early stages of an infection.
It’s been suggested that IgA is a critical antibody class to stimulate, and previous arguments suggested that the vaccines only stimulate the production of IgG.
Surprisingly, the evidence here suggests IgA production, as noted within the serum of the participants:
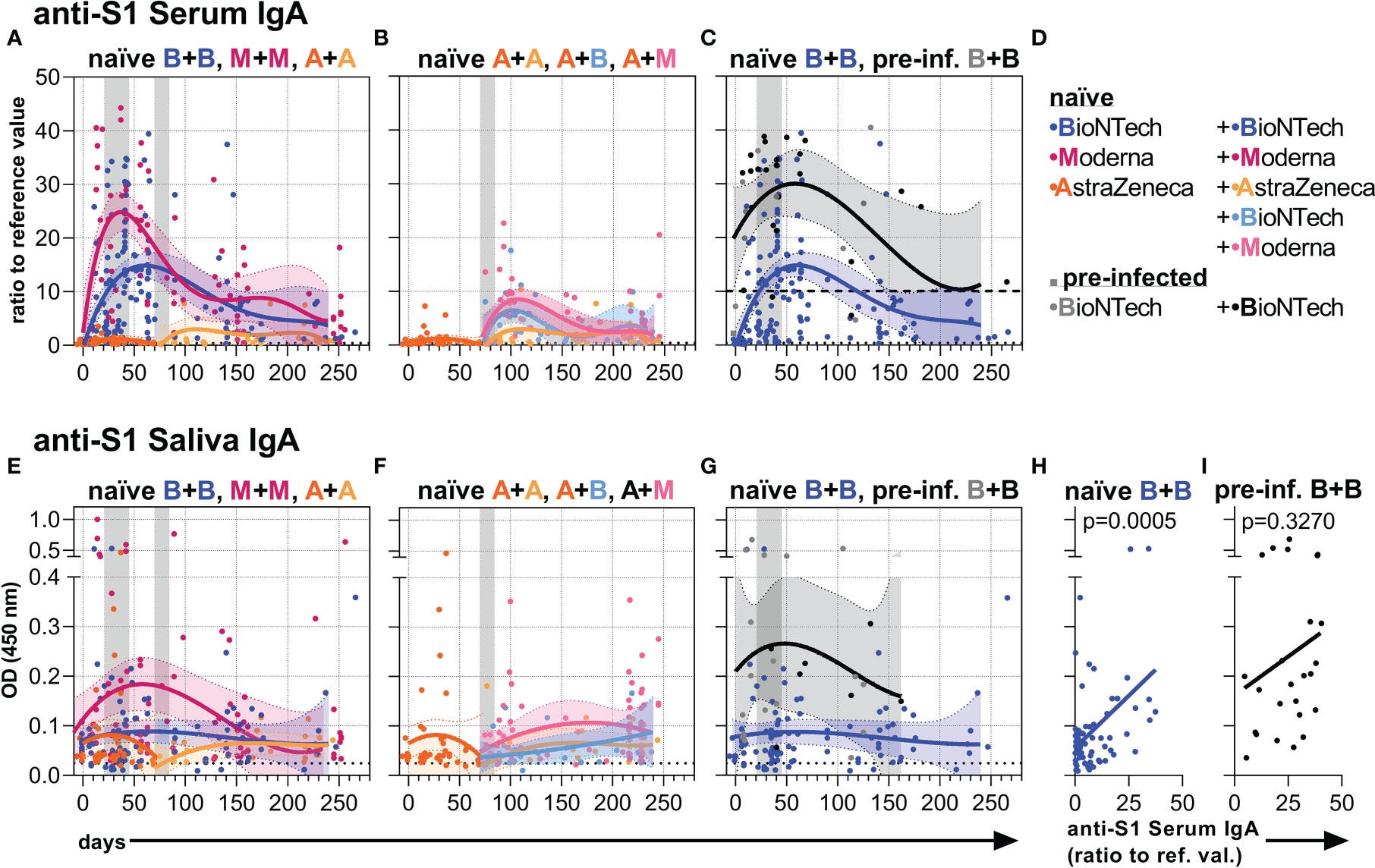
Similar to the IgG class of antibodies IgA antibody levels were dependent upon the vaccine vector, as Moderna’s showed the highest levels and with mRNA showing higher levels relative to the adenoviral vector. Of course, in those who were previously infected the IgA levels were far higher post vaccination and actually remained elevated relative to vaccine-only individuals who showed a quick decline to relatively lower levels.
Although salivary IgA levels were relatively low, this may seem like some sort of positive, right?
In some regards it would be. Some have suggested that reduced production of IgA may be related to SARS-COV2 severity.5
However, upon looking up the information there’s apparently a disease associated with IgA called IgA nephropathy, or Berger’s disease.
In this kidney disease IgA apparently accumulates within the glomeruli of nephrons causing inflammation, localized damage, and obstruction of the kidneys’ ability to filter urine.
The general cause of IgA nephropathy is unknown, and may stem from genetic factors as well as previous infections. In several cases it may go unrecognized until an individual notices blood in the urine, which may signify severe kidney disease.
IgA nephropathy has been noted with SARS-COV2 infections6,7, but several reports have noted IgA nephropathy as an adverse reaction post-vaccination as well.8,9,10
As it has been suggested that IgA tends to be one of the highest serum antibodies, this raises some questions as to how much IgA may be produced, and what may predispose someone to IgA nephropathy whether from the virus or from the vaccines.
This, again, indicates the complexity of the situations and why all avenues should be examined when considering adverse reactions.
On differences in methodology
The following section is a bit more on the technical side, but I think it’s worth mentioning that not only results should be compared, but methods should as well.
Given that these two studies are some of the only studies out there examining IgG4, or really examining all of the subclasses, it’s worth looking at how they differ in their methodology.
Note that the scaling between the two studies are different, with the ELISA platform from Buhre, et al. showing a ratio while the Irrgang, et al. study shows a concentration in ug/mL.
The Irrgang, et al. study utilizes flow cytometry, which is a platform that takes up a cells, presses them through a fine capillary and a laser is shot onto the cells as they pass through. The laser helps analyze and quantify the makeup of cells. With respect to this method, the cells utilized are studded with SARS-COV2 spike proteins, washed with diluted patient sera so antibodies bind, and then are placed into the instrument for analysis. A lot more goes on, but this is a very basic description for now.
Apparently the flow cytometry platform utilized by Irrgang, et al. was developed in-house11 in another study.12
Surprisingly, when the researchers compared their results to a manufactured ELISA platform their results suggest a higher level of sensitivity for IgG:

And the researchers note the following:
Overall, this demonstrates a high sensitivity of our cytometric antibody assay in a direct comparison to commercially available detection kits (Table (Table1).1). The lower detection limit was also confirmed by serial dilutions of selected positive samples. While 1–10,000 dilutions were still measured as seropositive by our flow cytometric assay, the two other kits revealed a negative result suggesting a higher analytical sensitivity of the flow cytometric test (data not shown).
The researchers note that they compared their in-house assay to a standard one (EUROIMMUN ELISA):
Commercially available ELISA for the detection of anti-SARS-CoV-2 IgG (anti-S1-specific, EuroImmun, Cat #EI 2606-9601 G) and IgA (EuroImmun, Cat #EI 2606-9601 A) were performed according to the manufacturer’s protocols.
This is important, because the kit used by Buhre, et al. is…:
Enzyme-linked Immunosorbent Assays (ELISA) were used to detect always anti-S1 (the extracellular part of S containing the RBD) Abs. The EUROIMMUN SARS-CoV-2 S1 IgG (EUROIMMUN, Lübeck, Germany; #EI 2606-9601-2 G), the EUROIMMUN SARS-CoV-2 S1 IgA (#EI 2606-9601-2 A), and the EUROIMMUN SARS-CoV-2-NCP IgG (#EI 2606-9601-2 G) ELISA were performed according to manufacturer’s instructions […]
This isn’t quite the bombshell point, as Buhre, et al. notes they used an in-house process developed in another study, and therefore it may be improper to compare the ERUOIMMUN kits to the in-house processes.
But regardless, it’s important to highlight that different methods can provide different results. Although both the Buhre, et al. and the Irrgang, et al. study compare IgG subclass antibodies, they both use different methods with the Irrgang, et al. one likely being more sensitive.
Interestingly, it was noted in the Lapuente, et al. paper that the EUROIMMUN kit may actually be more sensitive in its detection of IgA compared to IgG:
Detection of SARS-CoV-2-specific IgA was previously reported as more sensitive than detection of IgG in the EuroImmun ELISA kits [14].
As to the sensitivity of IgG, it’s important to note that flow cytometry assay used by both Lapuente, et al. and Irrgang, et al. test for the full spike while the EUROIMMUN ELISA kits and the in-house method used by Buhre, et al. only utilize the S1 subunit.
Because of this, it’s possible that the Irrgang, et al. study may be picking up antibodies specific to the S2 subunit, as well as antibodies from other coronaviruses that are cross-reactive to the S2 subunit of SARS-COV2.
Lapuente, et al. notes the following:
This higher sensitivity to detect S-specific IgG might be due to the different viral antigens used in the assays. Our flow cytometric assay exploits full-length S protein in its natural conformation and with the respective post-translational modifications due to the expression in mammalian cells. This enables detection of the full spectrum of S-specific antibodies directed against conformational epitopes and glycosylated sites as well, some immunogenic sites possibly missing in truncated, recombinant S1-only proteins as used in the EuroImmun ELISA.
Essentially, different tests have different sensitivities, meaning they may pick up more antibodies than other assays. That may reflect in a higher-than-normal reporting of certain results. That also comes with the fact that the flow cytometry assay used measures full spike while the ELISA assay only measure the S1 subunit.
This also calls into question which antigens are being targeted by the antibodies. One may suggest that the use of a full spike in an assay is better since this is what is presented in both the vaccine and the virus. On the other hand, if all of the IgG4 antibodies are targeting the S2 subunit is there less to be worried about (relatively speaking)?
It’s important to remember that it’s not just about the results, but how the results are obtained that should be looked into.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Graf, Tobias. (2023). mRNA vaccines against SARS- CoV-2 induce comparably low long-term IgG Fc galactosylation and sialylation levels but increasing long-term IgG4 responses compared to an adenovirus-based vaccine OPEN ACCESS EDITED BY. Frontiers in Immunology. 13. 1020844. 10.3389/fimmu.2022.1020844.
Irrgang, P., Gerling, J., Kocher, K., Lapuente, D., Steininger, P., Habenicht, K., Wytopil, M., Beileke, S., Schäfer, S., Zhong, J., Ssebyatika, G., Krey, T., Falcone, V., Schülein, C., Peter, A. S., Nganou-Makamdop, K., Hengel, H., Held, J., Bogdan, C., Überla, K., … Tenbusch, M. (2022). Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Science immunology, eade2798. Advance online publication. https://doi.org/10.1126/sciimmunol.ade2798
Lecuit, M., Aucouturier, P., Abbas, A., Cadranel, J., Silvain, C., Berthelot, J. M., Fauchais, A. L., Loubet, P., Bachmeyer, C., Montravers, F., Dossier, A., Nunes, H., Cervera, P., & Coppo, P. (2022). Overexpression of IgG2 in patients resembling IgG4-related disease with normal IgG4. Scandinavian journal of immunology, 95(3), e13126. https://doi.org/10.1111/sji.13126
Andualem, H., Kiros, M., Getu, S., & Hailemichael, W. (2020). Immunoglobulin G2 Antibody as a Potential Target for COVID-19 Vaccine. ImmunoTargets and therapy, 9, 143–149. https://doi.org/10.2147/ITT.S274746
Quinti, I., Mortari, E. P., Fernandez Salinas, A., Milito, C., & Carsetti, R. (2021). IgA Antibodies and IgA Deficiency in SARS-CoV-2 Infection. Frontiers in cellular and infection microbiology, 11, 655896. https://doi.org/10.3389/fcimb.2021.655896
Elgardt, I., Carmi, O., & Levy, Y. (2022). IgA Nephropathy (Henoch-Schönlein Purpura) Associated with Recent COVID-19 Infection. The Israel Medical Association journal : IMAJ, 24(11), 697–698.
Farooq H, Aemaz Ur Rehman M, Asmar A, et al. The pathogenesis of COVID-19-induced IgA nephropathy and IgA vasculitis: A systematic review. Journal of Taibah University Medical Sciences. 2022 Feb;17(1):1-13. DOI: 10.1016/j.jtumed.2021.08.012. PMID: 34602936; PMCID: PMC8479423.
Ma, Y., & Xu, G. (2022). New-Onset IgA nephropathy Following COVID-19 Vaccination. QJM : monthly journal of the Association of Physicians, hcac185. Advance online publication. https://doi.org/10.1093/qjmed/hcac185
Yokote, S., Ueda, H., Shimizu, A., Okabe, M., Yamamoto, K., Tsuboi, N., & Yokoo, T. (2022). IgA nephropathy with glomerular capillary IgA deposition following SARS-CoV-2 mRNA vaccination: a report of three cases. CEN case reports, 11(4), 499–505. https://doi.org/10.1007/s13730-022-00707-0
Tseng, Po-Hung MDa; Chuang, Shu-Han MDb; Pan, Yueh MDa,c,d; Shih, Hung-Jen MD, PhDa,e; Chang, Chin-Pao MDa; Huang, Sheng-Hsien MDa,*. Gross hematuria and IgA nephropathy flare-up following the first dose of Moderna vaccine: A case report. Medicine 101(52):p e32524, December 30, 2022. | DOI: 10.1097/MD.0000000000032524
Some labs produce their own in-house methods and testing procedures. In-house is different than using manufacturer kits which may provide a standard method of analysis, but is not good for adapting to new or specific methods. Therefore, some labs may try to create their own methods that are tailored to what they want, although such methods would then have to be validated.
Lapuente, D., Maier, C., Irrgang, P., Hübner, J., Peter, A. S., Hoffmann, M., Ensser, A., Ziegler, K., Winkler, T. H., Birkholz, T., Kremer, A. E., Steininger, P., Korn, K., Neipel, F., Überla, K., & Tenbusch, M. (2021). Rapid response flow cytometric assay for the detection of antibody responses to SARS-CoV-2. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology, 40(4), 751–759. https://doi.org/10.1007/s10096-020-04072-7
Thanks for this great post. It is so valuable to have people like you who know so much about the details of studies, the methodologies used, etc. 👍🏽💕
The differing methodologies stuff is a bit over my head but suggests that the effects are very real, when 2 different teams and methods find the same kind of result?