


The Melatonin Scare
Another supplement, another way to stoke fear in the consumer.

A few weeks ago the CDC released a nearly decade long study1 looking into melatonin use in children and overdose rates.
At this point you may be thinking a few of the following:
How many children are taking melatonin?
You can overdose on melatonin?
Is this really a serious issue?
Not to spoil the ending, but if you were thinking the 3rd point (likely the 2nd as well) you’re likely in the same camp as most of us.
I was considering looking into this matter but was conflicted only because it seemed somewhat pointless.
However, as media outlets continued to cover this and even had people in my personal life comment on this matter, I thought it best to take a look and actually detail what this report includes.
Melatonin Overview

Melatonin is one of the most utilized hormones in our bodies with a diverse array of physiological effects. Our body makes a lot of it in-house (endogenous), but in recent years it’s also become widely available as a supplement (exogenous), usually taken orally.
If you never thought of melatonin as a hormone, remember that hormones aren’t just molecules to make someone huge and muscular, or something that deals with sex maturation. Hormones are signaling molecules, which means that they tell other cells and organs in the body to initiate or prevent various biochemical pathways.
Melatonin is mainly produced in the pineal gland and is usually associated with aiding in our sleep/wake cycle (termed circadian rhythm), and most supplements market melatonin as a sleep aid. We usually produce high levels of melatonin at night and when there is low sunlight, so it makes sense that it’s implicated in aiding with sleep (Tordjman, et. al.2):
Melatonin regulates circadian rhythms such as the sleep-wake rhythm, neuroendocrine rhythms or body temperature cycles through its action on MT1 and MT2 receptors [23, 42-49]. Ingestion of melatonin induces fatigue, sleepiness and a diminution of sleep latency [26]. Disturbed circadian rhythms are associated with sleep disorders and impaired health [50]. For example, children with multiple developmental, neuro-psychiatric and health difficulties often show melatonin deficiency [51]. When circadian rhythms are restored, behavior, mood, development, intellectual function, health, and even seizure control may improve [50, 52]. It should be noted that according to several studies, circadian rhythms are important for typical (normal) neurodevelopment and their absence suppresses neurogenesis in animal models [53-56].
But that’s not all that melatonin is capable of. When looking at the structure you may not be surprised to find out that melatonin is considered an antioxidant, mostly derived from the aromatic nature of its rings (Reiter, et. al.3):
The direct free radical scavenging activity of melatonin has been known for almost 25 years.79 A subsequent report of this process also identified a novel melatonin metabolite, cyclic-3-hydroxymelatonin (c3OHM), which is formed when melatonin scavenges two free radicals; in this report, we also deduced the pathway by which c3OHM is formed.80 This discovery was followed shortly by a series of studies, conducted both in vitro81, 82 and in vivo,83-87 which documented the ability of melatonin to quell oxidative damage to molecules, cells and tissues, including human cells.88, 89 Since then, there have been numerous reports confirming the ability of melatonin to directly scavenge oxygen-centered radicals and toxic reactive oxygen species (ROS)90-95 and to diminish oxidative mutilation to key cellular macromolecules.96-102
It’s also capable of eliciting other antioxidant mechanisms within the body. So not only can melatonin act directly to scavenge for free radicals, but it can also call on other biochemical pathways to do the same as well:
Within 2 years after its discovery as a direct free radical scavenger, melatonin was found to stimulate antioxidative enzymes including glutathione peroxidase and glutathione reductase.106-111 Furthermore, melatonin upregulates the synthesis of glutathione,112-114 a highly effective intrinsic antioxidant, and synergizes with classic free radical scavengers to improve the reductive potential of tissues and fluids.115, 116 These indirect antioxidant functions of melatonin further leveraged this molecule as being a key endogenous factor in limiting free radical damage. Finally, melatonin was found to neutralize nitrogen-based toxicants, that is, nitric oxide and the peroxynitrite anion, both of which promote nitrosative damage,117, 118 and to suppress the pro-oxidative enzyme, nitric oxide synthase.119, 120
Now, not only can melatonin act as a hormone itself, but it can also act on reproductive organs as well (Tordjman, et. al.):
Finally, melatonin has physiological effects on reproduction and sexual maturation in mammals through down-regulation of gonadotropin-releasing hormone (GnRH) gene expression in a cyclical pattern over a 24-hour period [91-93]. The rhythmic release of GnRH controls luteinizing hormone (LH) and follicule-stimulating hormone (FSH) secretion. The daily profile of melatonin secretion conveys internal information used for both circadian and seasonal temporal organization [67]. The melatonin rhythmic pattern entrains the reproductive rhythm via the influence of photoperiod on LH pulsatile secretion and therefore mediates the seasonal fluctuations of reproduction clearly observed in animals (seasonal breading as species-specific seasons for reproduction) and moderately observed in humans [94-96].
Here are a few other possible physiological effects of melatonin:
blood pressure regulation
cardiovascular regulation
immune system regulation
“master clock” regulator for the body’s organs and systems
role in energy expenditure and possibly BMI
Role in bone mass
So in short melatonin has a huge number of uses. Research continues to look deeper into what else melatonin can do. It makes sense why such a cheap, highly accessible molecule may continue to be heavily researched as well as. It may also explain why there may be incentives to, well, de-incentivize the use of melatonin in the public.
Increasing melatonin use
A few years ago it was relative rare to see any ads about melatonin, but now it’s hard to find any supplement shelves without a section dedicated to melatonin alone.
With the disturbances of modern day life our sleep continues to be disturbed. I doubt that there’s many of us who don’t go to sleep without having a podcast on at night anymore. As such, more and more people are turning to melatonin as a way of getting a good night’s rest.
In the US the use of melatonin as a supplement has almost doubled in the past years. However, given the timing of this survey we should expect the figures to be much higher. Here’s an excerpt from the Sleep Foundation:
In recent years, synthetic melatonin supplements marketed to treat a variety of sleep disorders have become ubiquitous. From 2007 to 2012, melatonin use in the U.S. doubled1 and it now ranks as one of the nation’s most popular supplements. Its popularity stems in part from its image as a natural alternative to traditional sleep medications, which are known for side effects.
And as stated in the CDC article, pediatric melatonin use rose over 500% from the years 2012 to 2021.
It’s interesting that pediatric use of melatonin has rose dramatically over the past few years, mostly because children produce a high level of melatonin themselves and may not require exogenous supplementation.
Also, considering that melatonin plays a role in the signaling of other hormones, one concern is that children who supplement with melatonin may alter their reproductive hormone levels (from the Sleep Foundation):
There are reasons for parents to be cautious about the patchy data on melatonin in kids. It appears that children may be particularly vulnerable to the possible effects of this supplement on reproductive hormones. Melatonin has been associated with19 puberty delays, irregular menstruation, and overproduction of the hormone prolactin. It is important to note, however, that research on this topic is conflicting20, and experts agree that the topic is understudied.
As the article stated, the evidence isn’t clear on this matter and the field isn’t extensively studied, although considerations would need to be made in discussing the role of exogenous vs endogenous melatonin.
Melatonin during COVID
At the onset of the pandemic melatonin use has drastically increased, and it would make sense if a large portion of pediatric melatonin use is derived from the coming of the pandemic. And it makes sense, since uncertainty in the future, loss of jobs, and the unknowns of a new virus is likely to keep many up at night.
At the same time, researchers began looking extensively into melatonin as a possible therapeutic agent to fight against COVID. Type in “melatonin and COVID” into any search bar, even if the algorithm works against you, and you are likely to come across plenty of studies and literature reviews.
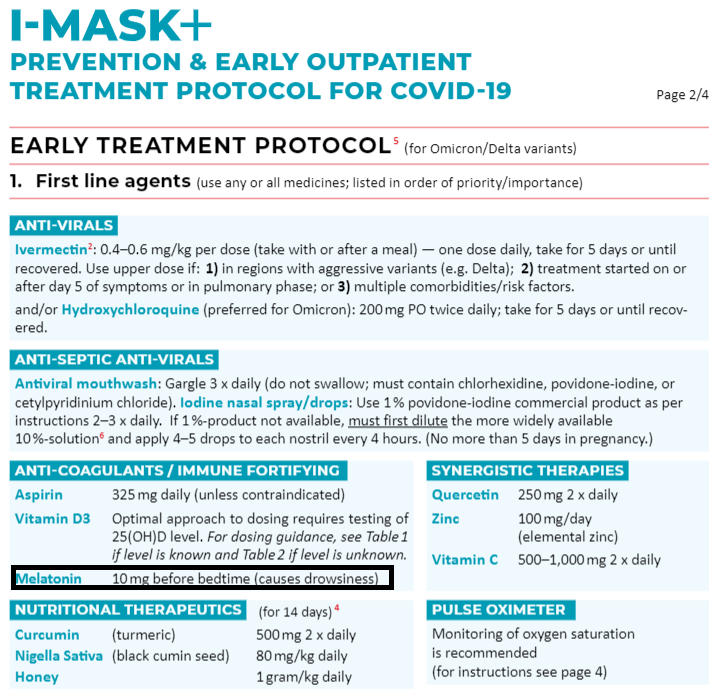
The FLCCC itself recommends the use of melatonin in many of its protocols:
So could there be some relationship between melatonin’s use during COVID and the sudden report warning of overdosing? I’m not sure, since it’s not like it’s happened before…

Is it possible to overdose on melatonin?
First off, I don’t want people thinking that this section is a key into downing melatonin tablets, but if we are to be concerned about melatonin overdose occurring we should at least figure out how likely it is to occur.
Most melatonin supplements come in 3mg-5mg tablets, although there may be 10mg tablets available. Generally, short-term used has been considered extremely safe although use for several months hasn’t been extensively examined.
When looking at dangerous doses you can usually look at the LD50, which is a number that indicates how much of a compound must be given before half the animals in a study die from toxicity. I say animal because we can’t conduct LD50 studies in humans- I don’t think the FDA would take too kindly at researchers intentionally killing off half of study group.
If we look at LD50 measures for oral melatonin supplementation, we can see that for mice that measure is around 1250 mg/kg and for rats its greater than 3200 mg/kg (measures taken from melatonin’s Pubchem profile).
Roughly, that translates to about 500-1500 mg/lb of body weight. If we consider a bottle of 100 tablets with 3mg of melatonin each, well… we may run into a bit of a problem with intentional overdosing.
Now, does that mean that people should down an entire bottle of melatonin? Absolutely not, and I implore people to absolutely not try that! Also, keep in mind that symptoms of overdose are likely to occur before the…final symptom of an overdose so to speak. The LD50 in animals also doesn’t translate directly into humans, and even children for that matter.
In general, this just tells us that it’d be pretty difficult to overdose. So how do we explain the supposed overdosing in children?
The CDC findings
This report from the CDC came out in early June and looked at reports to poison control in between the years of 2012-2021. Different demographic measures were collected of those children, including the age. Apparently the cutoff for this study was the age of 19.
Overall, an overwhelming number of calls to poison control occurred due to unintentional ingestion in children under the age of 5, and around 88% of the children were managed at the site of the overdose. In fact, around 82% of the children were asymptomatic (they did not show signs of overdose):
During 2012–2021, a total of 260,435 pediatric melatonin ingestions were reported to poison control centers, representing 2.25% of all pediatric ingestions reported during the same period. The majority of ingestions were unintentional (94.3%), involved males aged ≤5 years, occurred in the home (99.0%), and were managed on-site (88.3%) (Table). Most children (82.8%) were asymptomatic. Among those with reported symptoms, most involved the gastrointestinal, cardiovascular, or central nervous systems.
For those children (and young adults) who arrived at a healthcare facility a majority of the cases did not require additional treatment, although a few required hospitalizations:
Among 27,795 patients who received care at a health care facility, 19,892 (71.6%) were discharged, 4,097 (14.7%) were hospitalized, and 287 (1.0%) required intensive care. Among all melatonin ingestions, 4,555 (1.6%) resulted in more serious outcomes. Five children required mechanical ventilation, and two died.
Be careful with these percentages. Remember that they correspond to percentages of the nearly 28,800 children who entered into a healthcare facility, not the total number of calls to poison control (over 260k).
The most important part of this study was the deaths. In this nearly decade long study only 2 children appeared to have died from melatonin overdose. Those in the media appear to have used these 2 deaths as some call to arms against melatonin, and although 2 deaths of children are tragic having a case fatality rate of 1 every 5 years is hardly something to get worked up over.
You also run into a lot of problems when you realize that these deaths occurred in infants 3 months and 13 months old- I’m pretty sure infants have no way of supplementing melatonin themselves. But if you look at the comments you’ll see one of these may have been intentional:
Both deaths occurred in children aged <2 years (3 months and 13 months) and occurred in the home. One ingestion involved intentional medication misuse; the reason for the other is unknown.
So in this struggle to alert the public about supposed pediatric melatonin overdose, few in the media appear to have covered that, for all intents and purposes, a large majority of these children did well AND that two of these deaths were not done at the hands of the children themselves (take this NPR headline as an example).
As to those who require hospitalization, that gets into factors such as the actual amount of melatonin, age, pharmacokinetics and the like in trying to figure out what happened.
But in general, there doesn’t appear to be a need to have an outcry to the level that many in the press has done. So what may be going on?
Making a mountain out of a melatonin hill
In their Discussion section the CDC remarks that a large number of melatonin use has come in the wake of COVID:
The largest annual increase in pediatric melatonin ingestions coincided with the onset of the COVID-19 pandemic. Unintentional ingestions were the primary drivers of this increase. This might be related to increased accessibility of melatonin during the pandemic, as children spent more time at home because of stay-at-home orders and school closures. Further, reports of increasing sleep disturbances during the pandemic might have led to increased availability of melatonin in the home (9). This pandemic-related increase in accessibility and availability might have contributed to increased exposures in children.
At a time when many people are told not to do their own research, or to try at home remedies and instead relegate themselves to twiddling their fingers until they require a ventilator, we may look at an excerpt like the one above and immediately assume that there may be ulterior motives at play here.
I don’t quite want to make that argument, but I also understand why people may feel that way, considering what happened to NAC and the timing of this study, as well as the number of research coming out harking the benefits of melatonin use (like the FLCCC has done).
The study alone may not warrant a need to investigate pediatric melatonin use, and the deaths certainly shouldn’t be looked at as anything aside from possible cases of infanticide (unless someone wants to explain how infants gave themselves supplements).
So why make such a stink about something that appears to be nothing but a nothing burger? Is this just to provide gossip for the layperson to ask each other, “OMG did you hear about that melatonin study?”
It’s not likely that they read the study themselves, and it’s likely that any news outlet that covered this study did so by obfuscating some of the information- you can tell when an article picks and chooses when to use numbers and when to use percentages.
All in all, this just appears to be another way to target individuals from finding information themselves and choosing to take their health in their own hands without the oversight of the CDC, NIH, or FDA. It’s a way for these alphabet institutions to disguise their need to control things under the guise of governmental paternalism. This is all done for your sake, not necessarily as something to look at and assess the information yourself.
As of now I don’t think much has happened aside from the typical snide remarks in the comments section or just talk around various parent circles, but that may not be all that happens down the line, and it’s important that we watch out for such changes.
When considering your own health, understand what the supplements you take do, and whether they may be necessary. For many children, the use of melatonin may not be necessary and there may be questions about long-term effects from exogenous melatonin. For adults, small doses have been considered relatively safe although more evidence may be needed to fully elucidate melatonin supplementation.
Keep these concerns in mind when balancing fear mongering.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Lelak K, Vohra V, Neuman MI, Toce MS, Sethuraman U. Pediatric Melatonin Ingestions — United States, 2012–2021. MMWR Morb Mortal Wkly Rep 2022;71:725–729. DOI: http://dx.doi.org/10.15585/mmwr.mm7122a1external icon
Tordjman, S., Chokron, S., Delorme, R., Charrier, A., Bellissant, E., Jaafari, N., & Fougerou, C. (2017). Melatonin: Pharmacology, Functions and Therapeutic Benefits. Current neuropharmacology, 15(3), 434–443. https://doi.org/10.2174/1570159X14666161228122115
Reiter, R. J., Mayo, J. C., Tan, D. X., Sainz, R. M., Alatorre-Jimenez, M., & Qin, L. (2016). Melatonin as an antioxidant: under promises but over delivers. Journal of pineal research, 61(3), 253–278. https://doi.org/10.1111/jpi.12360
Yes, it takes very little effort to search for melatonin levels by age and find out that the vast majority of children shouldn’t need melatonin supplementation anyways. We older folks OTOH...I’ve taken 3mg most nights for a few years and sleep better without any known ill-effects from the supplement.
And here is a link to some very interesting research on, among other things, melatonin and covid.
https://www.evolutamente.it/author/doris/
A three-month old child would still have a tongue thrust reflex which aids in nursing/taking a bottle as well as prevents accidental ingestion of solids. Of course, there would be absolutely no fine motor control to actually allow such a young infant to pinch a pill and/or place it in its mouth - they are still working on getting some neck muscles. I really hope someone is in jail after that. But yeah, it doesn't seem like something to be horribly concerned about ... yet the media finds another way to stoke fear in the hearts of mothers all across the country. 🤦🏻♀️