


PAXLOVID for Long COVID
A new study from the US Department of Veteran Affairs suggests that PAXLOVID may reduce long COVID symptoms (with many caveats).

Correction: As Brian Mowrey has pointed out in the comments section the language for one of the sentences below (noted with a *) was confusing and actually contradictory. Rather than say that the number of no long COVID patients in the PAXLOVID group was 2% lower, it should have said 2% higher to infer that fewer people within the PAXLOVID group had long COVID compared to the non-treatment group.
Thanks for Brian for pointing that out! Please check out his Substack if you haven’t done so already!
A few days ago a pre-print1 came out suggesting that PAXLOVID may help to reduce the symptoms of post acute sequelae of COVID (PASC) better known as long COVID.

Of course, such results have been met with widespread media attention.

In the arsenal of COVID treatments, long COVID has been an enigma as there doesn’t appear to be any treatments that are fully effective.
The mechanisms of long COVID are also ambiguous, as some studies infer possible persistent viral infection while some may lean towards immune dysregulation being the key factor.
In any case, one would think that a study looking at long COVID would be great for those who suffer long COVID, and of course Pfizer’s therapeutic will be the one to be put in the spotlight.
This study used health records from the US Department of Veteran Affairs database for people who tested positive for COVID in between March 1, 2022 and June 30, 2022.
As this information is taken from the VA, note that many of the participants leaned older (~65) and had at least one risk factor for severe COVID such as age, cardiovascular disease, obesity, cancer, etc.
There were far more people included in the non-treatment group compared to the treatment group, almost at a ratio of 5:1 non-treatment: treatment, although percentage-wise the makeup between the two groups appear to be similar.
The treatment group was provided PAXLOVID within 5 days of their positive test and were given a 5 day course of PAXLOVID, typical of the use of PAXLOVID.
As it relates to prior infection and vaccination status, a large portion of the participants either had two doses or a booster. The researchers also note that some of the participants had prior SARS-COV2 infections as well. However, there’s no indication as to the vaccination status of those who had prior infections (i.e. how many vaccines did they have and when relative to infection).

Now, when it comes to the results I will give some props to the researchers. Rather than report their results as a relative risk reduction (RRR) they actually report their results as an absolute risk reduction (ARR) which provides better real-world comparisons:
In this study, we provide 2 estimates of risk: a) hazard ratio (HR) of nirmatrelvir in comparison to the control group and b) absolute risk reduction (ARR) in percentage at 90 days; the latter represents the event rate reduction in nirmatrelvir group compared to the control group at 90 days.
For those who want to know the difference I wrote a piece comparing RRR and ARR, with some real-world evidence with the Pfizer vaccines in a prior post:

This makes for a very interesting assessment, as the results may not appear as spectacular as has been reported.
For instance, when comparing the risk of PASC, death, and hospitalization at 90 days2 between the two groups you’ll notice that the effect size is rather small:
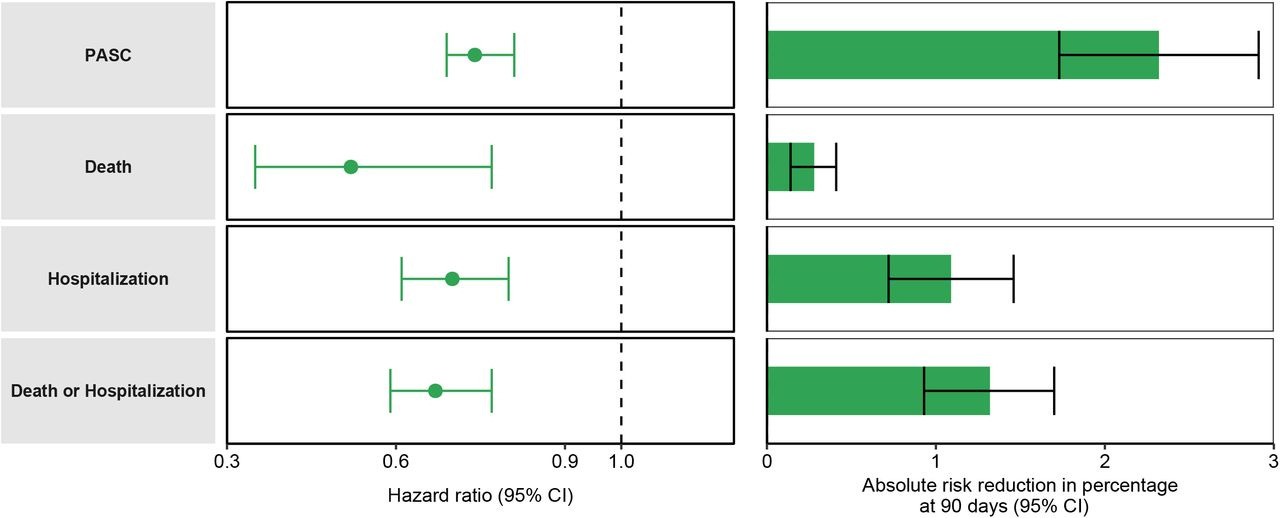
Note that the bars on the right are measures of ARR at 90 days, and if you look at the bottom you’ll notice that the ARR for PASC is slightly above 2%.
*That means that, in those who were provided PAXLOVID, the number of those who had no LONG COVID-symptoms at 90 days was 2% higher than the no-treatment group.
As a comparison, around 9.5% of those in the non-treatment group were recorded to have had at least one PASC while around 7% of those in the PAXLOVID group had at least one recorded PASC.

This is generally why studies may not want to report ARR compared to RRR. It doesn’t seem as flashy or remarkable with such low values, and it’s easy to misconstrue data that may make a treatment appear more effective than it should, which can be seen from this excerpt from the Discussion section which first notes the RRR but then provides the ARR in a convoluted way (emphasis mine):
Nirmatrelvir was associated with 26% less risk of PASC, 48% less risk of post-acute death, and 30% less risk of post-acute hospitalization; the magnitude of risk reduction on the absolute scale is also substantial amounting to 2.32, 0.28, and 1.09 less cases of PASC, post-acute death, and post-acute hospitalization for every 100 treated persons between 30 to 90 days of infection.
Keep in mind that participants were considered to have had long COVID if they presented with at least 1 of 12 prespecified post acute sequalae:
Outcomes examined in this study included PASC – defined as having at least one sequela from a set of sequelae based on prior evidence1,2,7-21.
So the divide here is whether a participant had any symptom of PASC vs those who didn’t. This, unfortunately makes the assessment of this study all the more confusing.
For instance, what exactly would be the typical number of sequelae, which participants had how many PASC, and rather than looking at the number of people with no PASC after taking PAXLOVID how many people may have experienced fewer symptoms in the treatment group relative to the non-treatment group?
This doesn’t even take into account the number of PASC for those who were vaccinated, boosted, or unvaccinated, or even those with prior infection that were a part of the other groups.
And that leads into the problem with the following results, which looked at individual sequelae and found that those given PAXLOVID had statistically significant reduction in 10 of 12 sequelae:
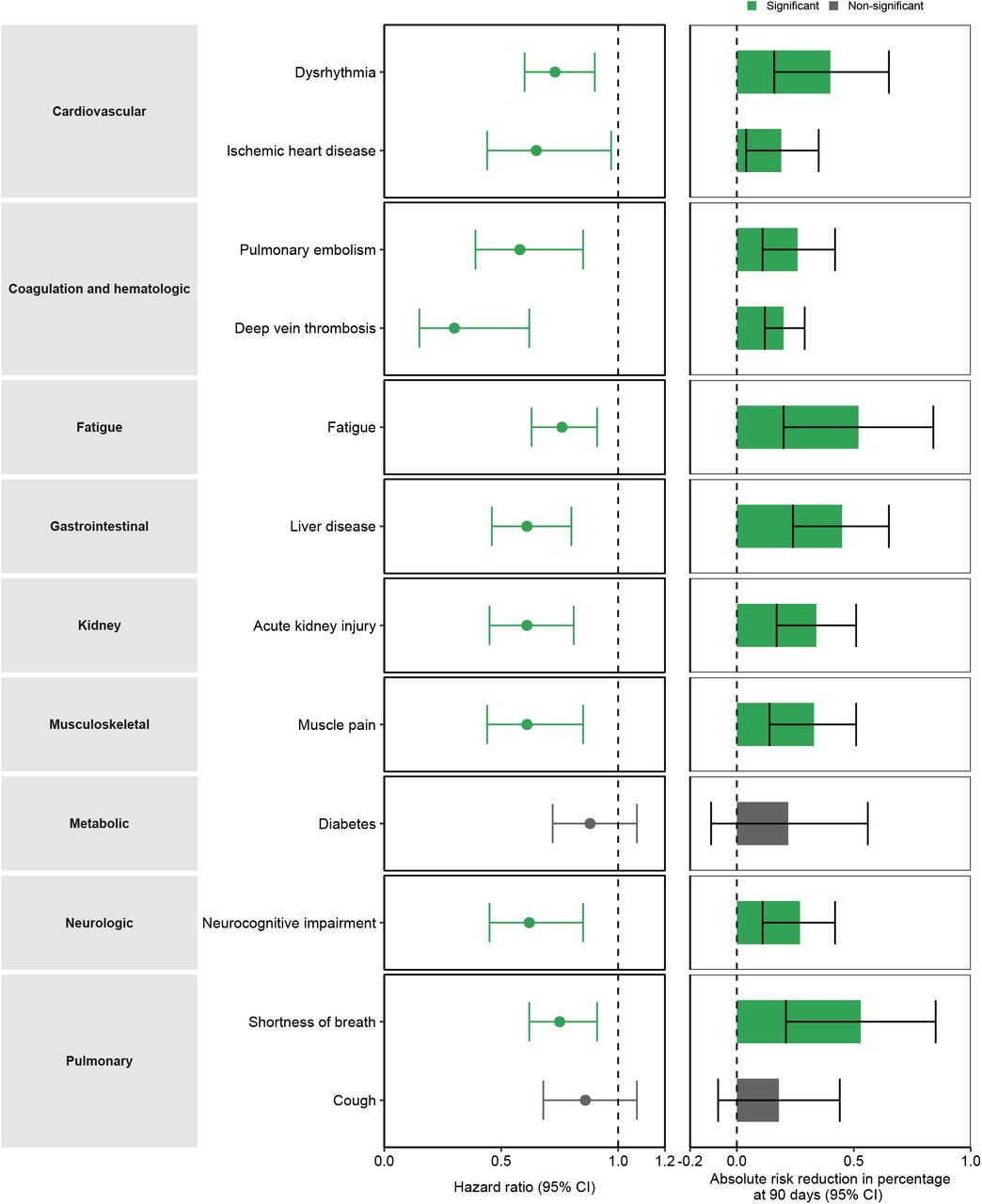
Note again that the ARR here is very low— all of them are under the 1% ARR value.
Again, the problem here is that there’s no indication as to how many PASC one individual had. It’s hard to assume that several people had either only one PASC or all 12.3
So how exactly do we interpret these results, or how much weight should we give it?
The problem is that long COVID is so ill-defined and there doesn’t appear to be a general consensus on how to measure it, as many of the approaches tend to be highly subjective.4
There’s also the fact that there’s no clinical evidence of this sort which looked at early treatment and the prevention of long COVID.
This brings up the important phrase: compared to what?
Although the ARR values here are low, we don’t have any evidence as to the effects of early treatment on long COVID in general, and so there’s no comparison to suggest whether these effect sizes are greater than other early treatments, worse, or if these effects are truly significant in a real-world setting.5
This study is full of ambiguities for a group of symptoms that, themselves, are very ambiguous.
Interestingly, one can make the argument that this would at least point to further evidence of the significance of early treatment. Not only may early treatment help reduce symptoms of COVID and lead to quicker recover/ no hospitalization, but that early treatment may also reduce the risk of experiencing long COVID symptoms.
As it stands, many treatment options for long COVID tend to occur after the diagnosis of long COVID and attempts to attenuate such symptoms. However, it may be more fitting to prevent the symptoms of long COVID in general by providing early treatment.6
Again, the literature is unfortunately lacking any information that can help in elucidating these assumptions.
One does have to wonder whether many of the early treatment options that were demonized such as Hydroxychloroquine or Ivermectin may have had some effect in reducing long COVID, but without any evidence and the halting of such research we’re left in the dark with respect to early treatment data.
In short, this study may not be all it’s cracked up to be because there’s really no way of measuring the extent to which these findings are significant. It’s one study in a sea of nothingness, and really highlights how there’s much about COVID that is still yet to be determined, including the phenomenon of long COVID.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Nirmatrelvir and the Risk of Post-Acute Sequelae of COVID-19
Yan Xie, Taeyoung Choi, Ziyad Al-Aly
medRxiv 2022.11.03.22281783; doi: https://doi.org/10.1101/2022.11.03.22281783
Note that a participant is considered to have PASC if they had symptoms 30 days after their positive test and persists for the following months up to the 90 day measurement period.
Since the Supplemental material does include percentages one can find a numerical value, however that doesn’t help provide any evidence to the number of PASC one has or how it is being counted here.
Many articles suggest that long COVID is defined as persistent symptoms past the 4 week since the acute/initial onset of the symptoms. However, how one measures “persistent symptoms” is highly subjective already, and one has to battle with figuring out whether the symptoms were from COVID or with COVID.
The number to treat for PAXLOVID in preventing PASC is 1 in 43.
This is also alluded to in the Discussion section, which notes that even though the evidence here was modest for long COVID reduction the pairing of both acute treatment and prevention of long COVID may be something worth considering as a reason for providing early treatment:
Although the magnitude of risk reduction of post-acute outcomes reported here is more modest than the reported effect during the acute phase (5 to 6% less hospitalization or death per 100 treated persons during the first 30 days of infection), the clinical decision to initiate treatment with nirmatrelvir should consider its overall effectiveness in reducing burden of death and disease in both the acute and post-acute phase of COVID-19.
You must understand that 'Long Covid' is a mechanism being employed to deflect liability. It is pseudo-theory in that it explains everything, anything, and nothing - all at the same time.
A “COVID illness” is due to:
1) Ordinary illnesses being relabeled as COVID due to the invalid PCR test.
2) Being healthy being relabeled as asymptomatic COVID due to the invalid PCR test.
3) Illness from severe air pollution (in China and Italy) being relabeled as COVID due to the invalid PCR test.
4) Fear and stress and isolation making you sick and being relabeled as COVID due to the invalid PCR test.
5) Lack of vitamin D due to reduced sun exposure making you sick and being relabeled as COVID due to the invalid PCR test.
6) Toxic masks and toxic nasal-swab PCR tests making you sick. The 2019+ quadrivalent flu shots likely had toxins added to them in some areas. We’re also being exposed to toxins via food/water/EMF etc. non-stop.
7) “COVID deaths” are due to remdesivir, ventilators, sedatives and the clot shots.
TPTB used 24/7 propaganda to hypnotize the masses into believing a global “pandemic” was real and that hospitals were overwhelmed with “cases” when in fact most hospitals were near-empty in 2020 due to the lockdowns. The only real pandemic is a pandemic of the vaccinated.
It’s imperative that people stop ceding ground to fascists by reifying the Big Lie that "Covid" is a unique disease and that it is responsible for a global pandemic.
This only fortifies the narrative by implying that any extra-ordinary response was ever necessary, that a single one of their “public health” diktats was legitimate.
This has never had anything to do with what is nothing more than a computer-generated genome falsely attributed to a novel pathogen. It is a global conspiracy by the world's transnational ruling class which was planned out and war-gamed at the WEF, the central bankers summit in Jackson Hole, and at Event 201.
It’s all right there for anyone to look up and see for themselves. It is about radically transforming every aspect of society in response to the final crisis of capitalism, which was no long profitable or sustainable, transitioning to the new digital financial system, implementing the technologies of the so-called 4th Industrial Revolution, and exterminating and sterilizing broad swathes of the “useless eaters” and now-surplus labor/population, who in old crises would be sent off to war, which is too risky today with weapons of mass destruction that could blow up the world a hundred times over.
Today they’re accomplishing the same thing through the bio-medical weapons of mass destruction of “covid” measures (isolation, medical malpractice, sedation, ventilation, manufactured unemployment, neglect, austerity, etc.) and poison injections.
The lockdowns, mandatory muzzles, anti-social distancing, and the other measures that did nothing to protect or improve public health were all designed to deliberately break the global economy (and crush competition, especially small businesses) as well as break our minds and the social fabric, in order to “build back better”, according to the diabolical and dystopian visions of the psychopaths waging this class war, which is essentially a billionaires utopia, in which they own the planet like a techno-feudal fiefdom, and oversee the drastically reduced population of digitally branded humanity like cattle in a super-surveilled technocracy.
All talk of so-called "Covid" is a meaningless distraction and quite besides the (existentially urgent) point when you understand that the virus/disease they’re allegedly designed to protect against doesn’t exist in the first place and, additionally, what their real, above-mentioned purpose(s) is.
"That means that, in those who were provided..." seems to have an extra "no."
It's good at least that Pax doesn't turn out to drive higher post-acute diagnoses due to hypothetical paradoxical effects on virus-host homeostasis, such as rebounds. Definitely not impressive as far as protecting against LC, given that neuro issues are barely moved and the issues with big moves basically just sound like severe cases (which we already know Pax is good at mitigating). At the same time, this isn't a surprising outcome given that LC doesn't seem as common after Omi (suggested here in a survey-based study https://www.medrxiv.org/content/10.1101/2022.10.12.22280990v2)