

"Ozempic Patients Need an Off-Ramp"
So why are they not provided one?

The header comes from a recent article published in The Atlantic, and it’s a sentiment that I have brought up multiple times when covering the Ozempic craze. So it’s a bit interesting to see mainstream press covering this topic:

Sadly, the article doesn’t actually engage with the idea that people should be able to get off of these GLP-1 RA medications and instead focuses on the cost of these medications as being difficult for patients to maintain:
To pharmaceutical companies selling the blockbuster drugs—known collectively as GLP-1 drugs, after the natural hormone they mimic—that might be a pretty good proposition. To patients paying more than $1,000 a month out of pocket, not so much. Most Americans simply cannot afford the cost month after month after month.
And strangely ends with this comment near the end of the article:
But tapering off obesity medications entirely, GLP-1 or otherwise, will probably not be possible for most patients. Weight loss tends to trigger a powerful set of compensatory mechanisms in the body, which evolved long ago to protect us from starvation. The more weight we lose, the more the body fights back. The fight never quite goes away, and most patients will likely require some kind of continued intervention just to stay at a lower weight.
Not much of a discussion in providing patients with an off-ramp when it emphasizes that most people may not be able to get off of these medications…
That’s a bit of a shame, because there hardly seems to be any discourse around the idea that these medications should be temporary, so seeing this be mentioned in mainstream outlets could help to persuade readers to consider foregoing these medications when possible. Patients who are using this to lose weight should be allowed other means of maintaining the weight-loss that shouldn’t require pharmaceutical interventions.
This is compounded by the fact that the discussion around these medications seem to forego the fact that we should be producing GLP-1 ourselves, and therefore shouldn’t the focus be on finding out what is going on with GLP-1 within people’s bodies and fixing that problem rather than managing GLP-1 dysfunction with medications?
Why is it that no one seems to be discussing the underlying biological mechanisms when discussing these medications?
Surprisingly, a bit of information has come out from the very same conference that is funded by Novo Nordisk.
One abstract listed1 at The 31st Congress on Obesity included a study in which some participants were tapered off of Semaglutide over the course of weeks and were provided a digital weight management program in tandem. Over half of the participants who agreed to tapering off of Semaglutide were able to stop taking the medication, and by the last available endpoint were able to keep the weight off.
The abstract can be seen below:

This study hasn’t been formally published, and we have to be careful from extrapolating too much from this data. I’ll refrain from entertaining the results until the full study is published. Note that the abstract never mentions the initial doses pre-cessation for the individuals, so it’s possible that some of these individuals who were able to stop taking Semaglutide may have been people taking lower doses to begin with. So be mindful that this study may have more pitfalls than we can discern from this abstract alone.
However, what’s worth noting here is the methodology that took place in this study.
Note that patients were tapered off of Semaglutide- something that doesn’t appear to be common in practice unless a patient is experiencing adverse events as a consequence of losing weight and being more sensitive to Semaglutide’s effects.
But along with the tapering was the online program that was intended to help maintain the weight lost. Now, this study doesn’t mention what the program entails (another reason for some reservation) but once again this is something that seems to be lacking within the discourse.
That is, people may lose weight on these medications but they may not be simultaneously taught how to eat right, exercise, or really engage in any lifestyle choices that would better help to provide a holistic approach to weight-loss and maintenance. Instead, the focus seems to be on the medications, and any dietary changes are a consequence of the medications due to not feeling the need to eat these bad foods.
Obviously, if someone is not made aware of the problem with their initial diet then it would be easy for them to just fall into those very same habits when they come off these medications. If you stopped liking chips while on Ozempic but stop taking these medications you can easily fall into the habit of consuming chips en masse rather than realizing that the chips may have been the problem to begin with. Introspection and understanding what made you obese to begin with is more important than the superficial image of losing weight, but again this doesn’t seem to be the message that is getting across to patients.
It doesn’t help that the idea of “forever-Ozempic” is made worse by comments regarding “Ozempic rebound”- as soon as you stop taking these medications you will gain the weight back.
Most of these comments are based on results from a study2 funded by Novo Nordisk and was part of their clinical trial process.
This study looked at patients who were on the highest-dose Semaglutide available (Wegovy/2.4 mg Semaglutide weekly) for 68 weeks and compared their weight gain relative to those given placebo after coming off the medication.
After coming off of the medications there was clear weight gained back within the Semaglutide group although they didn’t appear to return to their original weight (at least by the end of the 52-week off-treatment period):
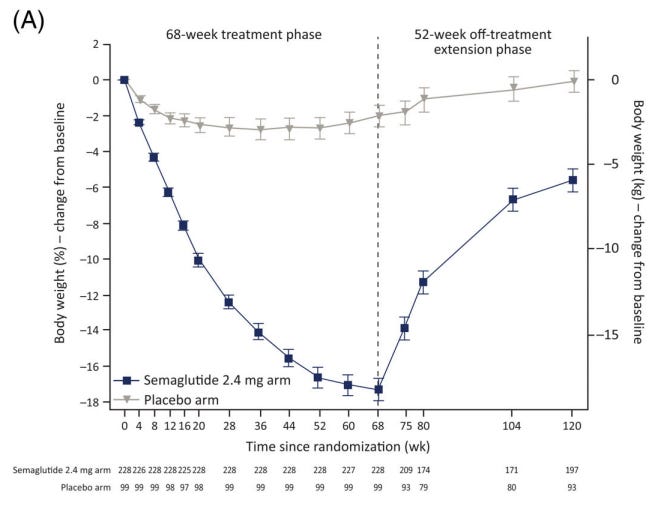
However, note that in this case patients didn’t appear to be tapered off of Semaglutide and instead came off cold-turkey.
Not only that, but patients were not coached on how to alter their lifestyle to help maintain the lost weight.
The study mentions “lifestyle interventions” in conjunction to coming off of Semaglutide, but this is what these so-called “lifestyle interventions” entailed:
The lifestyle intervention consisted of counselling every 4 weeks on diet (500 kcal deficit per day relative to total estimated energy expenditure at randomization) and physical activity (150 minutes per week).
This is hardly much intervention, and is a 500 calorie deficit relative to time of randomization sufficient for all participants? How many calories were participants consuming at the time of the cessation? If their calorie consumption decreased substantially then clearly a 500 calorie deficit may still be more calories than these participants should be consuming in order to maintain their weight.
This is made even worse given the fact that the researchers didn’t appear to keep track of participants’ maintaining these lifestyle interventions (emphasis mine):
No treatments were actively administered or prohibited during the extension. Concomitant treatments or events that might impact weight (obesity pharmacotherapy or bariatric surgery; medications for hypertension, diabetes or reducing lipids; pregnancy) were recorded during the extension phase. Participation in lifestyle interventions that might impact weight were not recorded.
So not only were participants given very limited interventions, but it would seem that researchers didn’t even look to see if people were committed to these lifestyle interventions.
It seems that this study was just doomed to fail from the start, and would we expect anything less from a study funded by the drug manufacturer and comprised of researchers with many conflicts of interest associated with Novo Nordisk?
As these medications continue to become more popular patients need to be provided a meaningful off-ramp. They need to be able to understand that they don’t need to be on these medications forever, but that takes patients knowing why they ended up in that position to begin with. People need to better understand the eating habits and lifestyle choices that made them obese and make sure to avoid those pitfalls in the future. They also need to be aware that these drugs may alter brain chemistry in order to dissuade them from bad foods, and that these feelings may come back after coming off of these drugs. Being prepared and fully knowledgeable on the challenges of coming off these drugs should make people more resilient from gaining the weight back.
Better education requires that people be aware that there is an out, and that they don’t need to become subservient to these medications.

If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Look for “GC4.271” or “Gudbergsen” on page 443 when trying to find the abstract. The abstract listing is hundreds of pages long so it will take forever to find it through scrolling!
Wilding, J. P. H., Batterham, R. L., Davies, M., Van Gaal, L. F., Kandler, K., Konakli, K., Lingvay, I., McGowan, B. M., Oral, T. K., Rosenstock, J., Wadden, T. A., Wharton, S., Yokote, K., Kushner, R. F., & STEP 1 Study Group (2022). Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes, obesity & metabolism, 24(8), 1553–1564. https://doi.org/10.1111/dom.14725
Maybe this link will work https://www.dailymail.co.uk/health/article-13455353/Is-Ozempic-Miracle-jab-slashes-risks-deadly-kidney-disease-affects-three-million-Britons-experts-hail-effect-better-dared-hope.html
I'm sortof looking at this as _________ patients need an off ramp. The same question arises with statins, diabetes medications, etc... I think an pathway out lies in integrative, functional and regenerative medicine approaches which incorporate lifestyle, nutrition, detoxification, examining multiple systems of the body... depending on a persons needs, issues, chronicity, complexity. My (somewhat limited) experience in working with pts on GLP-1's tends to focus on treating overall metabolic/hormonal/inflammatory picture, so that when the meds stop they are able to retain the weight loss achieved.