


Novo Nordisk comes under fire after study alleges monthly Ozempic costs under $5 to produce
A study published in JAMA raises questions regarding the actual cost to produce these highly expensive medications.

It’s well known that drugs such as Ozempic and other GLP-1 RAs have been criticized for their exorbitant prices, with some doses costing upwards of nearly $1,000 dollars in some cases.
However, a study published on Wednesday in JAMA1 has now stirred up even greater scrutiny of possibly price gouging by these manufacturers as it appears to allege that some of these GLP-1 RAs, as well as diabetes medications may only cost several dollars to produce which juxtaposes their upwards cost of hundreds of dollars.

This has raised serious alarms regarding the actual price of these medications, and has even led to calls to reduce the price of these drugs as Senator Bernie Sanders has done in lieu of this study.

Bernie Sanders seems to be arguing that the price of the drug should be no more than what Canadians pay out of pocket, which is almost around 1/3 the cost that Americans are being charged.
All this raises serious questions regarding how much these drugs cost to produce and how much people should be charged.
As of now the market on GLP-1 RAs has been monopolized by only a handful of companies- and by companies that have also monopolized the diabetes medication industry, meaning that not many options are available for patients, and unfortunately have allowed companies to pressure people into forking out much of their hard-earned money.
“The True Cost of Ozempic”
Following the release of this study the head researcher Melissa Barber was interviewed by CNBC:
It’s a good starting point for people who haven’t read the study yet, but what drew my attention was the title on the chyron: “THE TRUE COST OF OZEMPIC”.
This is because the study itself doesn’t provide a truly accurate depiction for what the cost of these medications are to produce, but are instead estimates.
The study considers many variables when estimating the cost of a product, all they way down to the storage unit used, additives needed to create the product, and even the cost to fill:

API is an acronym for active pharmaceutical ingredient and refers to the compound that is intended to produce some effect within the body. For example, the API in Ozempic would be Semaglutide. This is where most of the cost of these products are coming from.
However, note that each variable listed above comes with its own estimate, meaning that assumptions have to be made for the actual cost of many of these items. Given that API is where the bulk of costs are to be derived from the cost per unit of other variables may be minimal, but it’s nonetheless important to note one of the limitations of this study.
That is, multiple assumptions need to be made regarding the cost to source some of these units and so readers should be aware that this may mean the values used may not be accurate.
As to API, Barber, et al. used data collected from export/import information regarding these drugs, as well as information from manufacturers whenever it can be sourced:
We extracted customs data from a commercial trade database (Panjiva) that systematically archives shipment-level import/export records for numerous countries (eTable 4). For medicines where no export/import data were available, we estimated API prices through direct solicitation of price quotes from 11 API manufacturers, and inference based on review of methods of synthesis and other information available in academic and trade literature. API manufacturers were identified through internet search, online purchasing platforms (Pharmacompass and Pharmaoffer), supplier listings in cross-country price data collected, and inclusion in an IQVIA report on biosimilar global suppliers.1
Barber, et al. notes that this methodology is used extensively to assume costs of various products.
However, one trouble I have is interpreting whether listed export/import prices are relative to the actual cost to manufacture the API, or whether other variables should be considered such as lower export prices for larger shipments, or whether the export/import prices are related to the price for shipping alone.
This may, in part, explain why Semaglutide costs are relative low as compared to other GLP-1 RAs. The popularity of these drugs may allow for larger shipments and thus lower export/import costs:

And is somewhat noticed in a graph which maps shipping sizes of Semaglutide along with API costs from the past few years, although the data on this graph only shows one data point for a 1kg shipment so it’s hard to make out the significance of this graph. That being said, note that this graph at least suggests that some of the export/import data collected may be for shipments far smaller than 1kg, which again raises a question if smaller shipments may be hit with larger fees/tariffs:

There’s also a question regarding how well export/import data correlates to actual quotes from manufacturers.
Be mindful that these comments are made from my own naïve perspective, and given that this sort of methodology is used extensively it may be considered an appropriate way to estimate costs.
There are additional things to point out- note that when provided both manufacturer quotes as well as export/import data the researchers went with the smaller number in their calculations:
Where both price quotes received from manufacturers and exim data were available, we assumed the lower price for the purposes of calculating a sustainable cost-based price.
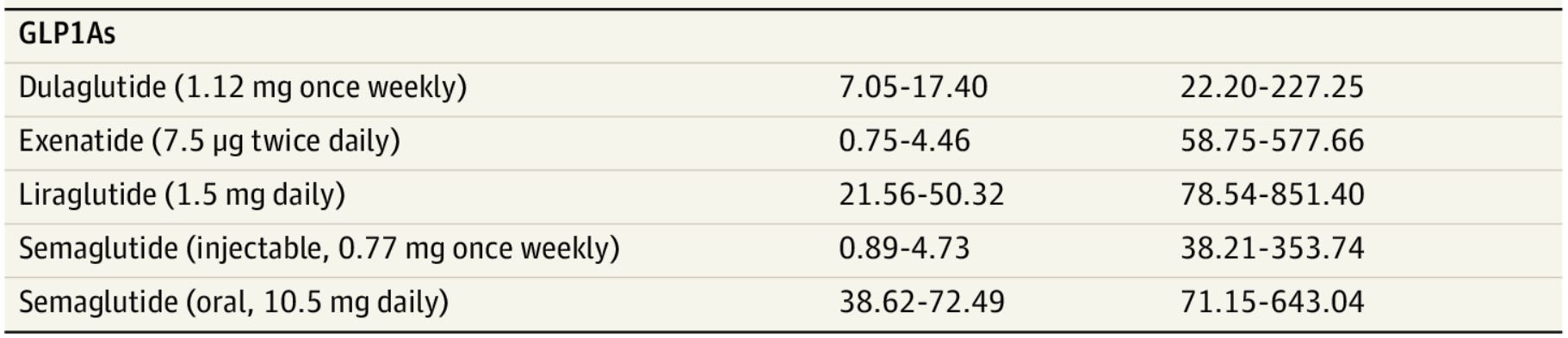
This actually doesn’t mean much within the context of GLP-1 RA calculations as it would mean that Liraglutide would be the only calculation that would be biased by the lower number (i.e. the researchers likely went with the 500k figure rather than the 573k figure in their calculations). However, this may also suggest that there are likely discrepancies between manufacturer quotes and export/import data.
The point of highlighting this information is to point out that the JAMA study doesn’t quite provide an accurate detail for what the production costs of these medications are, but rather are estimates built upon estimates.
This may seem like a semantic argument, but it’s important to point this out, especially when mainstream outlets display inaccurate words such as “true cost”, which may mislead viewers into thinking that Semaglutide should only cost around $5 for consumers. Bernie Sanders seems to have run with this figure even given the limitations in the estimates, and is an example of why politicians should due their due diligence in understanding the context of this number before disseminating misinformation.
So although it’s certainly true that a huge degree of price gouging is at play, it doesn’t mean that studies such as this one are true measures for the cost of manufacturing- only the manufacturers have those numbers and we know they certainly won’t release that information!
Also, note that the “price to produce/manufacture” is not indicative of “costs to consumers”. As Barber notes in her interview the model isn’t intended to take into account factors such as financial recouping for R&D, which likely would increase the price of the drugs.
There are additional factors that go into considering how much a drug should cost.
But what should be pointed out, and something that readers should be made aware of, is the fact that there is an obvious tiered system at play that dictates the prices of these drugs.
Note that the US carries the largest ticket price for many diabetes medications including insulin and GLP-1 RAs:

And part of this appears to stem from the fact that relatively wealthier countries are likely paying a premium for the same API that less-wealthy nations are receiving, as noted in this note regarding Exenatide’s pricing:
For exenatide, all observed API was shipped by the same company, with prices ranging 542,500 US$/kg to 1,007,140 US$/kg, with more costly API destined for high income countries in Western Europe and lower-priced API observed sold to less wealthy countries. The most recent shipment was twice as expensive as shipments observed to less wealthy destinations, resulting in the linear prediction model showing a sharp increase in price. Given that the product description and company are identical, we assume that this is a tiered price model, and use the lower level (542,500 US$/kg) as the API price.
Not only does this suggest that the estimated cost for Exenatide would be higher for Americans, but it also suggests that prices are likely higher for Americans across the board due to being a wealthier nation.
This isn’t all too surprising as many people are aware of this huge price discrepancy for the US relative to other countries- it’s just more evidence that Americans are for reason being forced to pay a premium on medications.
It’s somewhere in the middle
Here we are faced with two inherent truths:
People, and Americans in particular, are being price gouged for their medications.
This JAMA piece may not be an accurate representation of what consumers should expect to pay for GLP-1 RAs. To be fair, the study isn’t intended to show that, but it hasn’t stopped people from running away with that sentiment. Factors such as cost for R&D and the shipping of finished products vs API were not factored into the calculations.
As Barber puts it in her interview the true cost for consumers likely falls somewhere in the middle of what Barber and her colleagues have estimated and what people are actually paying.
And irrespective of what that number is it will certainly be far lower than the current price for these medications.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Barber MJ, Gotham D, Bygrave H, Cepuch C. Estimated Sustainable Cost-Based Prices for Diabetes Medicines. JAMA Netw Open. 2024;7(3):e243474. doi:10.1001/jamanetworkopen.2024.3474
I would not take it even for $5 per month
This JAMA "study" will fuel screaming headlines about the cost of drugs, but it mainly addresses the tiniest tip of the iceberg. Modern Discontent brings up R & D, one of the biggest contributors to drug cost, that is ignored when considering only cost of physical production, as well as the fact that U.S. consumers and tax payers have subsidized the cost of drugs "sold" to other countries for decades.
Ideally profits from current drugs would drive R & D for new drugs.
Even huger economic elephants are the funding of the FDA regulation and its revolving door relationship with Pharma. This is probably the majority of the cost of doing pharma business. These companies are effectively and collectively running their bloated subsidiary called the FDA.
Lastly, inundating the U.S. population with drug advertising has to be adding another 20% or more to the cost of pharma business.