
Media reports on the long-known fact that COVID deaths and hospitalizations have been overcounted
As many begin to argue that the pandemic is no longer a public health emergency, many are admitting that the fears over COVID may have been overblown.

Let me start of by stating that I consider COVID to be a very serious disease for select individuals, such as those who are elderly or those who are immunocompromised or ill.
There are many people who have succumbed to the disease, and long COVID is also a serious issue that is strangely being waived off as not being real in skeptic circles.
However, what’s been apparently since the early onset of the pandemic was the fact that many deaths, hospitalizations, and numbers of long COVID patients were being egregiously miscounted, leading to the widespread idea of “with” vs “from” COVID.
Today Time released an article detailing the winddown of COVID as a public health emergency, and yet the article buries the lede as much of the article is spent detailing this widely known fact of overreporting.

Time notes the following in their article:
For over a year, it has been apparent that many hospitalizations officially classified as being due to COVID-19 are instead of patients without COVID symptoms who are admitted for other reasons but also happen to test positive. Since nearly everyone is still routinely swabbed upon hospital admission (although the largest infection control organization has recommended against doing so), many patients with other conditions also receive a positive test result, especially during the ongoing Omicron surges—thereby overstating the number of hospitalizations tabulated as caused by COVID-19. UCLA researchers who examined Los Angeles County Public Hospital data discovered that over two-thirds of official COVID-19 hospitalizations since January 2022 were actually “with” rather than “for” the disease.
Many would argue that the numbers have been inaccurate since early on with the same reasons outlined above; that anyone who came into a hospital who tested positive with COVID were considered as technically being hospitalized for COVID.
And this isn’t a consequence of Omicron, but the inability of hospitals and the CDC to report accurate information, as many healthcare facilities may have been temporally incentivized to overcount numbers if these numbers are associated with funding in some way.
Dr. Leana Wen, who has been known to be a zealot for the CDC’s guidelines and vaccines even wrote a piece in The Washington Post detailing the overcounting.

Note that this “are” should refer to all deaths and hospitalizations from the very start of the pandemic, as it seems to just gloss over the fact that this issue has been ongoing.
Dr. Wen herself doesn’t tread any new territory, essentially rehashing the same issue of any person entering a hospital and given a COVID test being counted as a COVID hospitalization, although I would argue that the idea that this overcounting may not be derived from anything nefarious is itself an assumption with not much evidence.
Interestingly, Dr. Wen highlights Dr. Shira Doren, who sought to get more accurate measure son hospitalizations and death with COVID vs from COVID by using both positive tests and the use of dexamethasone, a corticosteroid commonly used for COVID as a proxy measure to confirm a COVID hospitalized patient.
In doing so, Massachusette’s COVID data showed a huge disparity between these with and from groups.
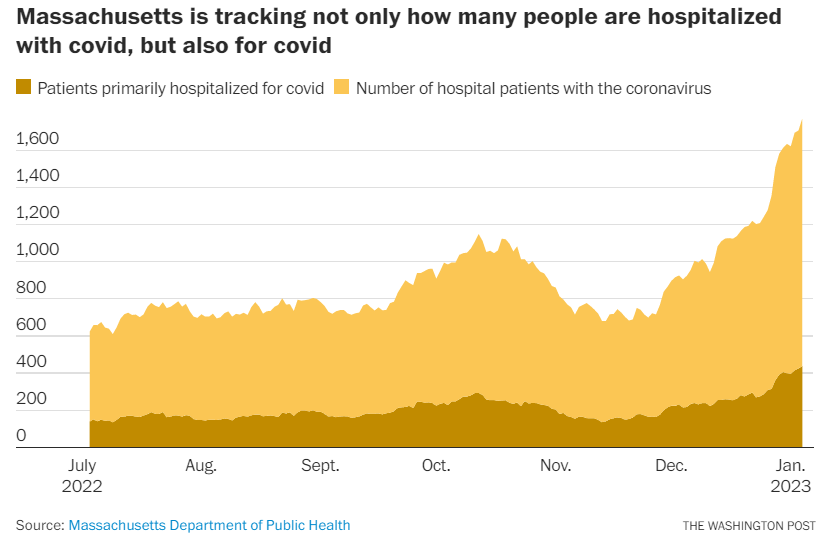
The data is unfortunately missing earlier timepoints, and it also still confirms COVID hospitalizations with proxies via the use of dexamethasone on patients, as patients may rely on dexamethasone for other reasons.
Nonetheless, it points to how inaccurate most of the COVID data has been. Imagine what the numbers could be for every state, which we again may not have accurate information on.
As for long COVID, studies have been heavily flawed in their reporting of long COVID because many of these reports relied on self-reports through telephone calls or online surveys. It’s been known early on that numbers on long COVID have been absolutely abysmal because most places did not have access to widespread testing, and so it was difficult for many clinicians to treat something without any indication of past experience.
To that, Time actually notes this criticism as well:
In addition to overcounted numbers of COVID hospitalizations and deaths, another reason for maintaining a public health emergency is the purportedly massive wave of ongoing long COVID. Yet almost all long COVID reports are based on tabulations of the number of persons who self-report lingering symptoms post-infection, rather than controlled studies that carefully compare the prevalence of persistent symptoms in persons who have been infected to those who have not.
As stated previously, I’m dubious of the claims that long COVID doesn’t exist, but I would argue that the numbers have been incorrect due to an inability to properly diagnose long COVID patients and to connect symptoms of long COVID to a previous infection until just recently.
But most importantly, all of these inaccurate data were used to lull us into a state of emergency; enforcing lockdowns, masking, and vaccine mandates all relied on data about hospitalizations and deaths.
Remember, those who strayed were “trying to kill grandma”, and yet the CDC and many hospitals couldn’t even accurate record grandma’s illnesses properly!
Time ends its piece with a rather apt remark, noting that these exaggerated numbers would mean that calls for mandates and vaccination of children may (i.e. were) be uncalled for and only serve to instill an air of fear:
The inadvertent exaggeration of COVID-19 deaths and long COVID leads not only to misplaced policy decisions, such as new mask mandates and booster recommendations for 6-month-old babies, but also to a needlessly enduring climate of fear, particularly in bluer regions (such as my hometown of San Francisco, where mask wearing remains commonplace, even outdoors). After three long years, it is past time to base public health pronouncements and policies on solid scientific evidence rather than well-meaning but often misleading assumptions.
The policies over COVID should have always been about proper science and data, but instead we were left with bad data and horrible policies which relied on such bad data.
The press can’t gloss over their role in pushing this climate of fear themselves, and the CDC should certainly be held in contempt for their use of poor data.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

"And this isn’t a consequence of Omicron, but the inability of hospitals and the CDC to report accurate information, as many healthcare facilities may have been temporally incentivized to overcount numbers if these numbers are associated with funding in some way"
----
I.e. Deliberately lie
As you know they need the EUAs for the boosters, which require keeping the "emergency" going. It keeps the vaccine manufacturers well protected from liability. Also, Paxlovid and Mulnopiravir are under EUA's and there is no need to disturb the money train that is greasing the right palms.