

Leqembi is likely to see full, traditional FDA approval. But can anyone explain what it actually does?
Part I: An examination of the Study 301 clinical trial.

On Friday an FDA advisory committee called the Peripheral and Central Nervous System Drugs Advisory Committee (PCNS) voted unanimously on the clinical efficacy of Biogen/Eisai’s immunotherapy Leqembi (Lecanemab), which is an IgG1 monoclonal antibody intended to target plaque and misfolded proteins found within the brain of Alzheimer’s patients.
When I posted a Notes with respect to this meeting, I incorrectly stated that the unanimous vote means that Leqembi is going to be fully approved through traditional means. Rather, the advisory committee, usually comprised of scientists and practicing clinicians (aside from one advocate that tends to be included as an adviser) are supposed to serve as unbiased individuals who provide the FDA insight into a drug’s approval. Thus, irrespective of what the advisory committee concludes, the FDA has final say on a drug’s approval, although I would find it rather difficult to see any indication of the FDA not giving approval over a unanimous conclusion of efficacy, as even the mixed response by an accelerated approval committee over Molnupiravir still led to the drug’s approved use for COVID.
Also, note that “unbiased” is being used loosely here, as one adviser was removed right before the meeting due to conflicts of interest, so it’s quite possible some advisers on these committees may have a stake in the drugs seeking approval.
In any case, the meeting comes at a time in which Biogen/Eisai have already been been plagued with a myriad of criticisms.
As I’ve reported many times, Biogen/Eisai’s first immunotherapy to see accelerated approval was Adulhelm (Aducanumab), which was met with a host of criticisms over the drugs efficacy, as well as concerning side effects and cost.




So what exactly can be gleaned from this all-day FDA meeting?
If one is daring to sit through the entire meeting, there’s a link below for the entire 7 hours.
In short, not only did I find the information provided not very compelling, but it raises a ton of questions with respect to these immunotherapies, including the rather egregious issue of figuring out what this drug is actually supposed to do.
To provide a bit of context, I’ll just remark that neither Eisai, the FDA, and testimonials by people or loved ones on Leqembi appear to provide clear, consistent clinical efficacy of those on Leqembi.
Although this article was intentionally going to dive into these remarks in particular, I found it necessary to describe some of the findings from the Phase 3 clinical trial first. However, this discussion took up a good portion, so this article will be broken into separate parts.
Results from the Phase 3 Clinical Trial
For those who want the slide presentation of the meeting only, the FDA has released Eisai’s slides, which I will draw from when referencing the clinical trial. This section breaks down parts of Study 301.
The approval committee was based largely on the results of Biogen/Eisai’s phase 3 clinical trial titled Study 301, also referred to as the Clarity AD study. The study was published in NEJM, although I don’t have access to the study, so I can’t examine the clinical trial in full detail aside from what’s provided in the slideshow presentation, but I’ll digress.
Study 301 was a double-blind, RCT with equal matching between treatment groups and placebo across all demographics, including patients who were carriers (both heterozygous and homozygous) for the APoE4 gene (Slide 16).

This is in contrast to the Study 201 results which showed uneven matching, with the placebo group being comprised largely of carriers relative to the highest dose (10 mg/kg biweekly) group, which was comprised predominately of non-carriers among the CORE portion of the study.
I have remarked a bit on Study 201 as well for those interested:

Primary endpoints for this clinical trial, as well as all Alzheimer’s related immunotherapies, are based on statistically significant differences in Clinical Dementia Rating- Sum of Boxes (CDR-SB) between placebo and treatment groups at the 18-month endpoint.
CDR-SB is a scoring measure which looks at 6 domains relating to cognition and function, and provides a score between 0-18 (broken down into 0-3 for each domain), with 0 being the best possible score and 18 being the worst.
Those who are defined as having mild-cognitive impairments (MCI) or mild forms of dementia (MD) generally receive a CDR-SB score within the range of 0.5-6. Note that the average CDR-SB score for patients included in Study 301 are slightly above a CDR-SB score of 3 among both placebo and treatment groups.
For additional context, note that any increase in a domain from 0 to 0.5 is considered a move towards impairment, and a move from 0.5 to 1 is a move towards dependency.
Lastly, note that the dosage used in the treatment group was for the highest dose from Study 201 of 10mg/kg biweekly over the course of 18 months.
Primary endpoints: CDR-SB comparison scores
Although the slideshow provides a breakdown of both primary and key secondary endpoints (Slide 19) I find that Slide 20 shows a good progression of the disease between both groups:
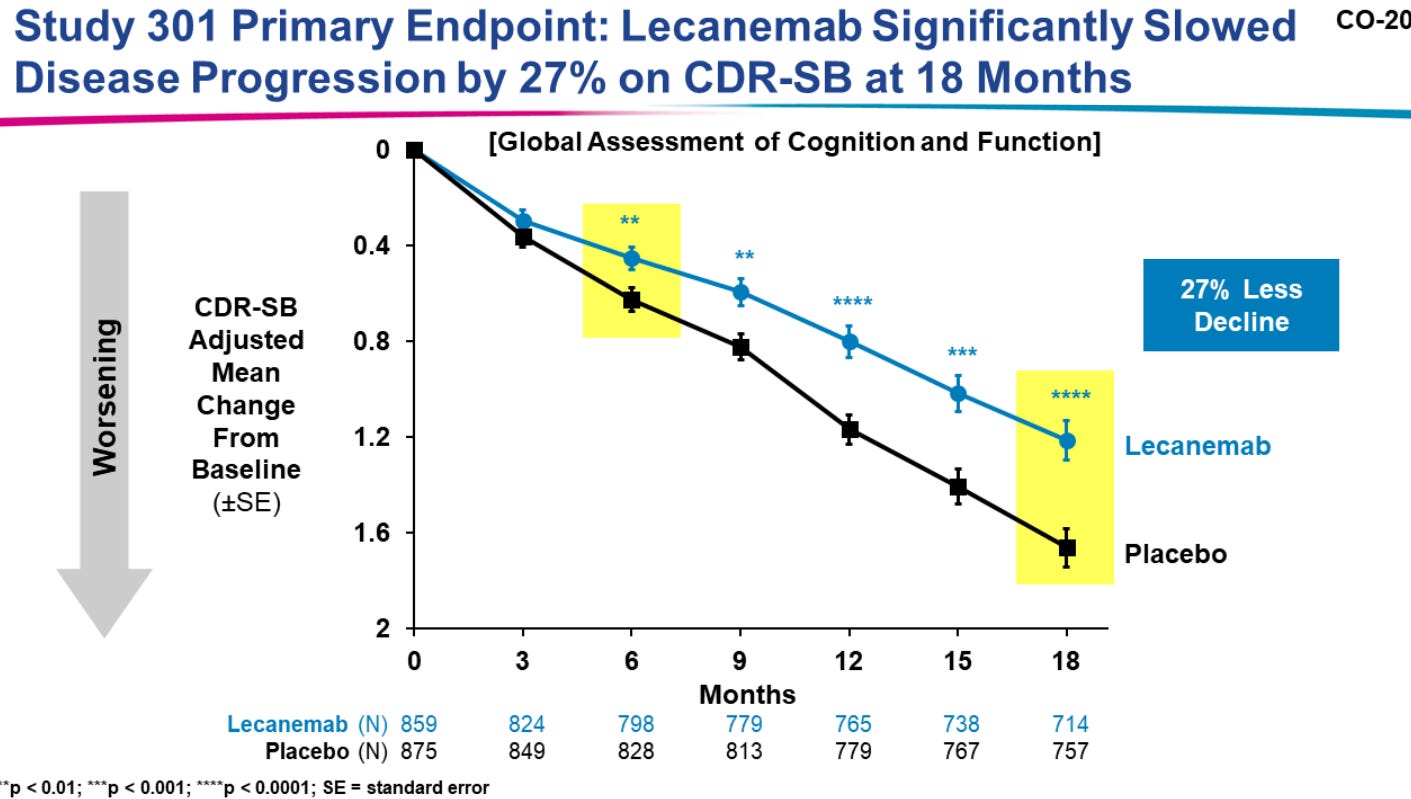
Remember that the primary endpoint here is based on differences in CDR-SB scores between the treatment group and placebo group. The way to interpret this graph is to remember that Month 0 is related to the CDR-SB mean score for both the placebo and Leqembi group, and not an actual CDR-SB score of 0. As time progresses, the mean CDR-SB score across both groups increase, suggesting increasing cognitive impairment and worsening of disease progression.
Here, differences between changes in CDR-SB scores between Lecanemab and the placebo group reached statistical significance by the 6-month mark (boxed in yellow above) and continued until the endpoint at 18 months.
This statistical significance relates to a CDR-SB score difference of 0.451 between the two groups (Slide 19), inferring a reduction in cognitive decline by around 27%.
Again, remember that this difference is not a measure of overall cognitive decline, but a measure of cognitive decline among Lecembi recipients relative to the placebo group. Put another way, this score of 0.451 suggests that at the 18-month mark placebo patients had a mean CDR-SB score 0.451 points greater than the Leqembi group, suggesting greater cognitive decline relative to the Leqembi group. Remember that in both groups cognitive decline did progress, as noted by the negatively-sloped lines between both groups. What’s being argued here is that cognitive decline is occurring more slowly in the treatment group, and is a large point of contention for many people skeptical of these results- more on this in a separate most.
Also, keep in mind that there’s no indication of what domains these CDR-SB scores are related to, as they are an aggregate score based on the 6 domains.
When it comes to secondary endpoints, I don’t find these to be worth breaking down in full, although it’s interesting to note that secondary biomarkers of amyloid plaque (Slide 25) and tau proteins (Slide 26) appeared to drastically decline in the Leqembi group.
What’s important to consider is the relevancy of these biomarkers to the pathology of dementia. Remember that there are conflicting considerations with respect to the amyloid hypothesis of dementia, in that many scientists aren’t convinced that these misfolded proteins are directly responsible for cognitive decline. Rather, it’s possible that senescence or decreased cellular function may not be able to control for plaque formation, and thus dementia may be associated more with cellular dysfunction rather than the presence of plaques and tangles.
Widespread Adverse Events
What has plagued both Adulhelm, and appears to be the case with Leqembi, is the fact that these immunotherapies are associated with many adverse events, including brain swelling, microhemorrhaging, and abnormal brain imaging.
Amyloid-related imaging abnormalities1 (ARIA) are a common occurrence with these immunotherapies and are related to abnormal imaging findings, usually by way of MRI results.
ARIA is generally classified into two categories:
ARIA-E refers to imaging noting edemas (swelling) in the brain
ARIA-H refer to abnormal imaging noting hemosiderin deposits, an indication of heme breakdown and iron-complex formation, as well as findings of microhemmorrhaging in the brain
The cause of these adverse events are not well-understood. One argument appears to suggest that deposits of these misfolded proteins onto vasculature such as blood vessels within the brain may become disrupted by use of these immunotherapies, and may lead to alterations in vascular integrity that lead to these adverse events. The FDA’s section on ARIA can be found here, as well as on Slide 45 of Eisai’s presentation for those who want addition information on these AEs.
Note here that ARIA is evidently more frequent among those provided Leqembi. More interestingly, ARIA appears to occur more frequently among APoE4 homozygotes (Slides 46 and 48, respectively) in both the placebo and Leqembi group.


This far higher incidence of ARIA among the Leqembi group, in particular among APoE4 carriers (especially homozygotes), raise some questions related to the uneven matching found in Study 201, and whether incidences of adverse events may have been underreported due to the lack of proper matching with respect to carriers.
There doesn’t seem to be an explanation for these findings of adverse events for APoE4 carriers, but it raised some questions by advisers as to whether patient genotypes should be examined prior to treatment with Leqembi, as APoE4 carriers seem to be at far higher risk of these adverse events occurring.
It’s also worth noting that these adverse events appear to occur within the first 3 months of treatment, with both Eisai and the FDA suggesting that these adverse events resolve within 4 months (Slide 47).
It’s again, curious, why these events are occurring so early on in the treatment. Eisai did not collect biomarker data until months 12 and 18 of the study, and so there’s nothing to use as a comparison within the first 3 months. That is, the hypothesis of vascular integrity being disturbed by way of Leqembi may relate in some way to amyloid and tau protein measures within the early months of treatment, such that rapid clearance of these deposits may increase the risk of vascular dysfunction, leading to ARIA upon imaging.
This also raised a concern over whether antithrombotics should be considered as contraindicators for Leqembi. The evidence from Study 301 is limited, although it appears that in the 3 people who experienced cerebral hemmorrhaging in the Leqembi group all 3 were on antithrombotics (one on high-dose aspirin, one on an antiplatelet, and one on warfarin).

Although the findings are limited, the FDA has considered providing a warning with respect to those who take antithrombotic medications and who may be eligible for Leqembi.
This was raised as a point of contention with respect to some of the advisers, who was unsure whether Leqembi should be provided with a warning label or should consider listing antithrombotics as contraindicators. In that regard, the FDA suggested pharmacovigilant assessments to determine whether there is enough evidence to warrant the inclusion of contraindicators.
As it appears, there is apparent evidence of adverse events occurring with the use of these immunotherapies, and for the most part these findings aren’t things that should be dismissed. The fact that the FDA and Eisai appear to infer that ARIA resolves within months seems to underplay the actual severity that microhemorrhages and brain swelling can cause. Keep in mind that this was one of the biggest points of contention for the advisers, and has been a deep concern for people who have been critical of Leqembi including myself.
Thus, these adverse events are not something that can just be easily overlooked, but raise necessary concerns over the harmful effects of these therapies, and whether the actual clinical efficacy of these treatments are worth the risk.
So far, Study 301 does not differ too much from the studies seen with Adulhelm, with the main difference between Study 301 and Study 201 being matched demographics.
However, what’s important here is examining this mean CDR-SB difference of 0.451, because how does one actually interpret a mean score difference such as this one?
This value is considered to be statistically significant, and by all accounts may of the advisers have remarked that there is clear, apparent evidence of clinical efficacy (timestamp for that portion).
As we’ve seen with Adulhelm, and as we see now with Leqembi, this question of clinical efficacy is not one that seems to be able to be defined, and if one cannot clearly define clinical efficacy for a drug can one really warrant the approval of said drug?
The next post will dive into a bit more detail on that manner, taking a look at some of the personal testimonies and rebuttals from the FDA meeting, some evidence from the literature in trying to interpret this value of 0.451, and why there doesn’t appear to be any clear indication of Leqembi’s actual effectiveness.
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Sperling, R. A., Jack, C. R., Jr, Black, S. E., Frosch, M. P., Greenberg, S. M., Hyman, B. T., Scheltens, P., Carrillo, M. C., Thies, W., Bednar, M. M., Black, R. S., Brashear, H. R., Grundman, M., Siemers, E. R., Feldman, H. H., & Schindler, R. J. (2011). Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: recommendations from the Alzheimer's Association Research Roundtable Workgroup. Alzheimer's & dementia : the journal of the Alzheimer's Association, 7(4), 367–385. https://doi.org/10.1016/j.jalz.2011.05.2351
I think we've lost any regulatory function that the FDA had. People need to be very careful now with pharmaceutical drugs. I don't imagine doctors have done the dive that you have. If anyone questions a doctor, your articles are so valuable to print out and hand to them. For some doctors, it will be the only way they will be educated about how low the FDA and CDC have fallen.
Is LEQEMBI news competitive w Casava forthcoming news?