


Is worsened cognitive performance related to COVID symptom duration?
A new study seems to suggest that those with persistent symptoms of Long COVID continue to show impaired cognitive function akin to "aging 10 years".

tl;dr: The following study was a recent one which raised some interesting questions about how long cognitive impairments may persist for those with Long COVID. Although interesting on the surface, the study doesn’t do much outside of what is already known. The following is for those who may be interested in the outline of the study, or may find some meaningful information.
I don’t have to alert readers to this growing concern that those who are COVID vaccinated appear to show higher levels of cognitive impairments, at least from what people have reported. Many of these stories are anecdotal or rely on suppositions and interpretations from news reports on accidents on tangential circumstances. Nonetheless, the frequency of anecdotes does raise an interesting question of whether there is true cognitive decline related to COVID vaccines.
But in figuring out this association between cognitive decline and COVID vaccinations it’s always important to consider parallels. In this case, it’s important to look at cognitive impairment in those who were infected with SARS-COV2.
Indeed, there are a good deal of reports associating cognitive impairment with active infections, and even Long COVID has been associated with persistent cognitive impairments.
More importantly, a recent study seems to substantiate this claim, suggesting that those who have symptoms of Long COVID continue to show cognitive impairments when given cognition tests, and these impairments seem more pronounced in those with the longest durations of Long COVID.
I came across this study first within this Smithsonian Magazine article:

There’s a bit of clickbait with this title- we’ll look at where this “aging ten years” claim is coming from later on.
Study Design
The study in question was published in The Lancet.1

For clarity on the timeline and how participants were examined, note that recruitment began around the end of March 2020 via the UK’s COVID Symptom Study (CSS), which was a volunteer surveillance program app to examine COVID prevalence, symptom onset, COVID positivity, and vaccination among participants.
These participants were then asked to be invited into the COVID Symptom Study Biobank (CSSB) between the timeframe of October- November 2020, as well as in May 2021. Essentially, the group chosen to participate in this study were narrowed down from people who opted into the CSS and were then invited into CSSB. Thus, when the study refers to “invitation” they are referring to when participants joined CSSB and not CSS, and at the time of invitation their COVID status and duration of symptoms were assessed, as well as during Round 1 and Round 2 of cognitive testing.
An overview of this study methodology can be found in the below excerpt as well, which notes that Round 1 of cognitive testing took place between July-August 2021, and Round 2 taking place between April-June 2022:
Cognitive performance (working memory, attention, reasoning, motor control) was assessed in a prospective cohort study of participants from the United Kingdom COVID Symptom Study Biobank between July 12, 2021 and August 27, 2021 (Round 1), and between April 28, 2022 and June 21, 2022 (Round 2). Participants, recruited from the COVID Symptom Study smartphone app, comprised individuals with and without SARS-CoV-2 infection and varying symptom duration. Effects of COVID-19 exposures on cognitive accuracy and reaction time scores were estimated using multivariable ordinary least squares linear regression models weighted for inverse probability of participation, adjusting for potential confounders and mediators. The role of ongoing symptoms after COVID-19 infection was examined stratifying for self-perceived recovery. Longitudinal analysis assessed change in cognitive performance between rounds.
Given the time of recruitment the symptoms are likely to be related to an infection rather than vaccination, although participants are likely to have been vaccinated between Rounds which is something to consider as a confounding variable for symptom duration.
Unfortunately, as with any study of this sort there’s a lot of subjectivity with the data reported. Demographic data may not be verified, and SARS-COV2 positivity and symptoms are based on self-reports of testing.
There’s also no verification of infection resolution. Remember that the phenomenon of Long COVID, or post-acute sequelae of COVID (PASC) refers to symptoms that persist after the infection has ended, and so unless routine testing was conducted to verify negative status there really is no way of knowing when the infection ended aside from assessments asking patients if they felt “back to normal” by the time of the cognitive tests.
For instance, at Round 1 participants were further stratified based upon how they answered the following prompt to discern recovered and persistent symptoms among participants:
“Thinking about the last or only episode of COVID-19 you have had, have you now recovered and are back to normal?”
This is getting a bit ahead of the other aspects of study design, but just be aware that there was no actual test to determine whether participants were truly negative aside from self-perception, which is one of the biggest issues with Long COVID studies in general as they tend to rely on patients to report symptoms and positivity rather than taking a proactive approach.
In going back to participant groups, the study organized participants into 5 different groups based upon COVID status and reported symptoms at the time of invitation into the CSSB program:
Case Group 1: COVID positive with Asymptomatic COVID
Case Group 2: “Short COVID”, or those who tested positive with symptoms that lasted fewer than 4 weeks.
Case Group 3: “Long COVID”, or those who tested positive with symptoms that persisted longer than 4 weeks.
Control Group 1: “Long non-COVID”, or people who tested negative but reported symptoms which lasted at least 4 weeks.
This group was likely used as a reference to discern other possible infections or diseases from the COVID positive group (i.e. provides a baseline for other infections).
Control Group 2: “Healthy non-COVD” are those who tested negative and reported symptoms that lasted 1-3 days.
Although negative tests were never confirmed, note that it appears participants were asked to report COVID testing whenever they experienced any symptoms, and so any onset of symptoms, whether COVID related or not, appeared to be associated with testing if possible. Therefore, participants were likely to be shuffled between groups based upon their status at the time of Round 1 or Round 2 of cognitive tests.
This just means that readers should be aware of possible patient shuffling, and that there may be a delineation between the two cognitive tests since the composition of the two groups may differ.
For demographic data refer to Table 1 of the study, but for now note that the study participants skewed older (around 60% of participants within the 50-70 age range), female (79.5%), and white (96.1%).
Cognitive Decline and the “aged 10 years” comment
Cognitive testing was conducted using the Cognitron platform. Cognitron is open to everyone so you can take some of the tests for yourself. The study suggests that the platform or similar can provide measures on various cognitive impairments:
… cognitive batteries using the same platform have previously been shown to be sensitive to cognitive impairment in early Alzheimer's disease, cognitive decline in individuals with mild behavioural impairment (an at-risk state for dementia), cognitive function in older adults with high vs. low autistic traits, and “brain training” task repetition.22, 23, 24, 25, 26
Keep in mind that people were not supervised while taking the test, so outside variables such as noise, interruptions, and things of that nature may contribute to the results.
As to the actual tests, I took “The Cognitron Challenge”, which was a series of different tests from addition/subtraction, number and letter recall, and pattern recognition. There was one test I had an issue with (Verbal Analogies), which joined two pairs of words, with you being asked if the comparisons between the two were true or false.
In short, I think that test in particular required you to actually know the words being compared, otherwise your “wrong” answers may be due to ignorance rather than actual cognitive impairments. I guess that means something for me in particular since I scored pretty poorly on that part.
In any case, try the tests available if interested. They do ask for very basic demographic info at the end to compare you to others within your group.
When looking at Round 1 and Round 2 test results relative to baseline groups, those who tested positive seemed to perform worse on these tests relative to those who self-reported as being SARS-COV2 negative and asymptomatic (reference group). Also, among the SARS-COV2 positive group, the longer the duration of symptoms the worse the performance appeared to be.

The data isn’t consistent at some points, such as the “Negative, symptom duration <4 weeks” group which appeared to do better than the asymptomatic, negative group on Round 1 of testing but then did worse on Round 2.
Also, irrespective of positivity, all groups that reported symptoms seemed to do worse than those who were not positive and presented with no symptoms, which may suggest that other circumstances of health may contribute to cognition. This highlights one of the issues of Long COVID studies when other factors are not accounted for in the assessment, as other maladies can contribute to feelings of brain fog, depression, and fatigue.
Note that the biggest discrepancy appears to lie among the “Positive, symptom duration >12 weeks” group when compared to the negative, asymptomatic group, which the authors note as being the group that stood out the most in their Discussion (emphasis mine):
Our results partially support the hypothesis that those with community-based SARS-CoV-2 infection show cognitive deficits in performance accuracy relative to non-infected individuals, but only among groups with ≥12 weeks symptom duration from prospective symptom logging and/or self-reporting as not recovered and “back to normal” following infection. For these individuals with detectable deficits at initial testing, longitudinal follow-up showed deficits persisted at almost two years since infection.
When taking into account the self-perceived status of participants’ symptoms, those who self-reported to still have symptoms (based on the question highlighted earlier in the post) at the time of Round 1 testing did worse than those who perceived themselves to have recovered.
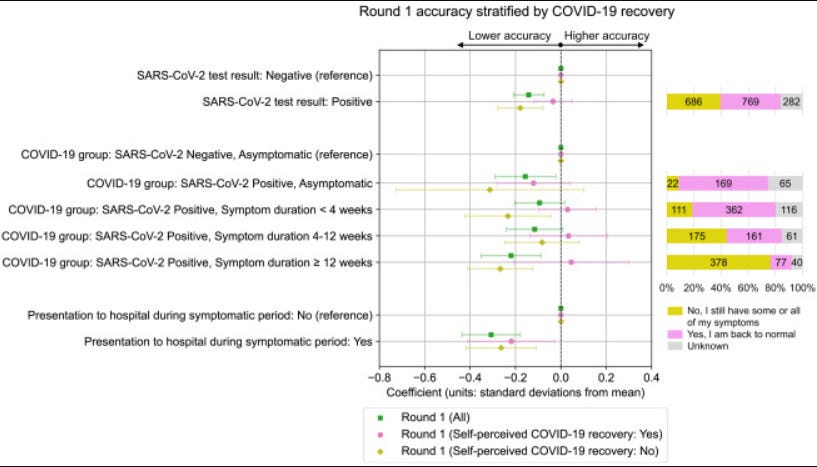
This appears to suggest that ongoing symptoms may be associated with poorer cognitive performance (at least as measured by the cognitive tests provided), although the strength of symptom duration in this case doesn’t appear to be as strong as the possible perception that one is not well at the time of taking a cognitive test.
Now, the question some people may have is with respect to this “aging 10 years” suggestion made in the Smithsonian Magazine article.
When seeing this comment note that these comparisons are all relative. That is, exactly what groups are being compared to when making such a point?
The researchers make this comment within their Discussion about this aging [context added]:
The deficits in composite task accuracy scores [for those positive and symptoms greater than 12 weeks] were comparable in scale to the effect of presentation to hospital during illness, an increase in age of approximately 10 years, or exhibiting mild or moderate symptoms of psychological distress, but smaller than other effects such as lower educational attainment or above threshold fatigue levels (Fig. S5).
All this means is that the cognitive test scores among those who may be categorized as being Long COVID sufferers (sans the negative testing requirement) appear to be similar as those among the groups listed above. It doesn’t necessarily mean that you appear to have the cognition of someone 10 years older than you.
Note that the reference for the age groups used were participants between the ages of 50 and 60, and the researchers themselves comment that the effect size they are referring to is comparing the 50-60 age group to the 60-70 age group, so it’s not as if this information can be extrapolated to all age groups to infer that people in their 20s with Long COVID have cognitions similar to people in their 30s.
So this is a bit of reporting with a tinge of lacking context, maybe for the sake of clickbait.
Conclusions
All in all, this study, albeit a bit interesting on the surface, also doesn’t appear to add much to what was already considered when it comes to Long COVID.
One thing that the researchers mention is that those who were infected between Round 1 and Round 2 of testing showed quicker symptom clearance relative to those in 2020 and not the same degree of worse testing results.
They make a comment suggesting that this may be related to vaccination and reduction of symptoms:
Conversely, in an opportunistic analysis of individuals who were recruited with SARS-CoV-2 negative statuses but had first infections between rounds of cognitive assessment, we found much less convincing evidence of cognitive sequelae for these later COVID-19 infections. Such infections occurred after vaccination against SARS-CoV-2 (>99% of 257) and skewed towards shorter durations than infections before Round 1, which may reflect our sampling strategy, as well as the reduced likelihood of long COVID (illness duration ≥4 weeks) for more recent delta vs. alpha and omicron vs. delta variants,49, 50 and following vaccination.20
But it’s also likely that better treatment protocols and less severe variants may account for this difference. It depends mostly on the variant/time of infection, as Round 2 participants would have included those who were infected with Omicron. Shuffling of participants would also have to be taken into account as well in between Rounds, so there’s multiple reasons for this difference in between Rounds.
For some infected during 2020 their test results were worse than baseline, which may suggest that for some people Long COVID may still persist 2 years after the infection period. It coincides with the fact that post-viral syndrome may persist for years.
The researchers also comment that symptom resolution tended to be associated with improved test results, although the source of the symptom can’t be considered within the context of this study, only temporally associated with a COVID infection.
There’s a lot about Long COVID and COVID vaccine adverse reactions that are yet to be answered. The growing concern over cognitive changes among these people warrants necessary investigation, even if those in power don’t appear to be too compelled to look for themselves.
This study, on the surface at least, suggests that cognition may recover after symptom resolution, but more qualitative tests would be needed to answer that question, especially for those vaccine injured. In reality, a lot of surveillance data is missing for those people.
It may be worth considering this sort of study in relation to those who are vaccine injured and see what information can be gathered. More importantly, it can provide some insights into the duration of vaccine-related complications and underlying factors. Tying symptoms with other measures can provide much needed insights, and may tell us how long certain symptoms seem to persist or what the course of recovery may seem like for those who may be injured.
There’s still a lot of information that is missing, and better constructed studies can help with figuring out whatever is going on.
Substack is my main source of income and all support helps to support me in my daily life. If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists such as myself to provide work outside of the mainstream narrative.

Nathan J. Cheetham, Rose Penfold, Valentina Giunchiglia, Vicky Bowyer, Carole H. Sudre, Liane S. Canas, Jie Deng, Benjamin Murray, Eric Kerfoot, Michela Antonelli, Khaled Rjoob, Erika Molteni, Marc F. Österdahl, Nicholas R. Harvey, William R. Trender, Michael H. Malim, Katie J. Doores, Peter J. Hellyer, Marc Modat, Alexander Hammers, Sebastien Ourselin, Emma L. Duncan, Adam Hampshire, Claire J. Steves. The effects of COVID-19 on cognitive performance in a community-based cohort: a COVID symptom study biobank prospective cohort study. eClinicalMedicine, 2023; 102086 DOI: 10.1016/j.eclinm.2023.102086
"Cognitron". That's what I shall name my genius world domination robot.
Been a long 31 months of going through this Long Covid journey especially the brain fog, confusion and fatigue. Any information on this topic is like Gold to me. Thank you.