
Is PAXLOVID rebound more common than previously thought?
A recent study from Scripps suggests that viral rebound after PAXLOVID treatment may be higher than was previously been reported.

Cover image from New Scientist
Edit: Brian Mowrey rightfully pointed out in a post from April that the confirmed cases may be a consequence of early seroconversion rather than a prior infection:
Once again, the trial excluded individuals with Covid vaccination (as reported during the medical assessment at enrollment) or previous confirmed infection. This high rate of antibody positives (51.84%; (540+528)/(540+487+528+505)) should thus be driven by early immune response to the current infection.
So the “confirmed case” may actually not be previous infections, and may just be a consequence of the infection that was measured during the time of enrollment into the study. Keep that in mind as a correction for the comment that was meant to be a correction below!
PAXLOVID rebound vs viral rebound
Yesterday I posted an article suggesting that viral rebound may be a feature and not a bug of COVID, to the extent that viral rebound appears to occur more frequently than was previously assumed.
Now, the article came about due to an LA Times article suggesting as much, and I wanted to see where the LA Times was getting their data from to make such an argument.
Some may wonder if my post was intended to serve as a defense of PAXLOVID or as a refutation of the PAXLOVID viral rebound argument.
I would argue that the fight over early treatments or the vaccines are not quite the same. PAXLOVID is not likely to see the same adverse reactions as the vaccines, and its use isn’t intended to serve as a prophylactic.
However, similar institutional and regulatory capture are at play here given that early treatments were barred in lieu of the vaccines and now the treatments of PAXLOVID and Molnupiravir. The high bill of PAXLOVID is certainly not something to dismiss, and we should be reminded that many doctors had their licenses and ability to practice jeopardized for doing something that doctors have always done before— treat their patients without obstruction from higher federal agencies.
In short, the post was not meant to argue that PAXLOVID treatment did not lead to viral rebound, but that we should keep in mind that viral rebound may be a consequence of COVID infection in general, so to what extent PAXLOVID may either attenuate or exacerbate the rebound effect remains to be determined. This goes in line with the vaccines, and quite frankly prior immunity as well.
It was a mere reminder to not let new information override old information, but to understand how to piece the information together in a meaningful way. I and others remember that there were plenty of anecdotes of people who got COVID, felt much better, but a few days later would start feeling symptoms again.
It’s hard to quantify anecdotes, but given that these accounts came before the terms viral rebound or recrudescence were even codified in the literature we may have missed out on vital information, only to have initial thoughts now overridden by the story or study of the day.
Essentially, what may have been viral rebound with PAXLOVID may now be a narrative of viral rebound from PAXLOVID.
NOW, with that being said PAXLOVID certainly is not out of the clear! I at least need to explain the title of this article aside from seeming clickbaity.
A few studies have suggested that viral rebound may be higher in PAXLOVID groups compared to placebo groups.
The data from Pfizer’s EPIC-HR PAXLOVID1 trial showed slightly more viral rebound in the treatment group compared to the placebo group:
From baseline through day 14, viral load rebound occurred in 23 of 990 patients (2.3%) in the nirmatrelvir–ritonavir group and in 17 of 980 (1.7%) in the placebo group (Figure 1B and Table S2). Results regarding viral load rebound were similar in the nirmatrelvir–ritonavir group and the placebo group in analyses of the presence of coexisting illnesses, nirmatrelvir exposure, recurrence of moderate-to-severe Covid-19 symptoms (Fig. S1), the occurrence of hospitalization or death, baseline SARS-CoV-2 serologic status, and nirmatrelvir resistance (as assessed by SARS-CoV-2 Mpro gene or cleavage mutations).
A 0.6% difference is hard to quantify as being significantly different, and maybe we shouldn’t be too generous to Pfizer in possibly downplaying their own accounts of rebound as they only included information for those they believe to have shown viral rebound using their own defined terms.
However, when looking at this data should we infer that the difference is due to PAXLOVID, or whether the 1.7% serves as the baseline value for expected viral rebound? All that could really be inferred is that viral rebound is possible even without antiviral treatment.
One thing that needs correcting is the seroprevalence of the participants.
In yesterday’s post I commented that participants in the EPIC-HR trial had no prior immunity.
However, looking again it appears that several of the participants had evidence of previous infection:

Apparently the comment that “confirmed” cases were excluded was what made me assume that people with prior infection were not included without looking at the demographic breakdown.
Rather, people with known prior infections were not included, and those unaware that they had COVID at some point were included in the study, which strangely suggest many people were just unaware of their status.
Anyways, apologies for not catching that! A correction will be added to yesterday’s post to note that the serostatus of the participants was known.
Now, when looking at the viral rebound from the EPIC-HR trial there appears to be more rebound within the seropositive group compared to the seronegative group. The below chart was taken from the study which was referenced in yesterday's correspondence2:

This information is, again, interesting although there isn’t much in the way of assessing how prior immunity may interact with the pharmacodynamics of PAXLOVID.
The researchers make this comment insinuating no strong association [context added]:
In the present and/or persistent VLR population, seropositivity was 59% and 57%, and in the transient VLR population seropositivity was 43% and 28%, for placebo and nirmatrelvir-ritonavir, respectively. In brief, there did not appear to be a strong association with serostatus when entering the study (either positive or negative) and VLR [viral load rebound].
No, “strong associations” does not mean that there is no association, and so there may be a possibility that prior immunity may influence the viral rebound dynamics, although note that the sample size is rather small for this group and additional studies would be needed to figure that out.
So note that we are dealing with whether prior immunity plays some role in the viral rebound, or if something with PAXLOVID may create a unique scenario that makes viral rebound more likely than an untreated infection. Or, there could be a combination of factors at work.
New Scripps Study on PAXLOVID
As Brian Mowrey pointed out in the comments section yesterday a new study3 also suggests that viral rebound may be higher with PAXLOVID use than previously described.
This study was carried out by Scripps Research Translational Institute along with a telehealth company called eMed.
The study enrolled participants who tested positive using eMed’s “Test-to-treat” kits.
Participants had to give consent to participate in the study and were enrolled into either a PAXLOVID group ( n=127) or a control group (n=43) based on whether the participant wanted a course of PAXLOVID.
Participants who gave consent to be included in the study were sent an overnight kit with 12 antigen tests and a 5 day course of PAXLOVID for those who wanted it. The antigen tests were telehealth proctored, with each participant performing an antigen test at set intervals until day 16 of the study:
Enrolled participants were shipped, overnight, a kit with twelve eMed telehealth proctored Abbott BinaxNOW COVID-19 rapid antigen home tests. Participants in the Paxlovid arm completed their first study-provided antigen test and their first symptom surveys on days 2 and 5 of the 5-day Paxlovid course (day 2 was the quickest the study kits could be delivered to participants), and then every other day through day 16. After the 16-day period, participants completed a persistent/long COVID symptoms survey at 1-, 3-, and 6-month intervals.
And a layout of the study’s design can be seen below:

Fortunately, the researchers of this study provided an outline of their definitions. Usually studies push their definitions into the body of the work rather than keeping it separate, so it’s nice to see the definitions actually separated out and easy to recognize:
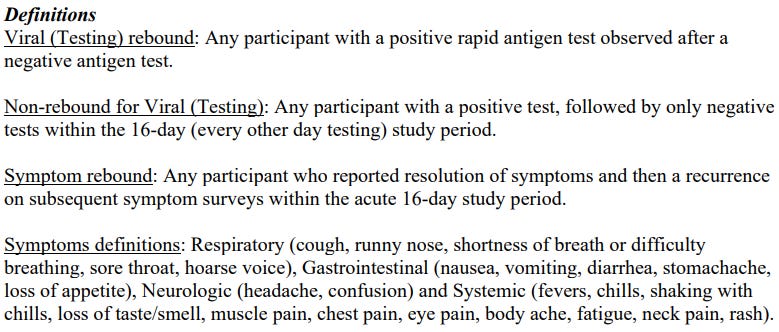
It’s still not a perfect definition as there isn't an explanation if viral load rebound and symptoms rebound are measured on some inclusionary/exclusionary factor, and it’s different than the one used for the EPIC-HR PAXLOVID viral rebound study so keep that in mind4.
Also, the participants in this trial skewed younger than other studies. Around 85% of the PAXLOVID group and 90% of the control group were below the age of 65 (Table 1).
There’s no indication for prior immune status aside from the fact that a majority of participants were indicated to have had at least one vaccine.
Now, interestingly the results of this study show a much higher rate of rebound in both the PAXLOVID and the control group compared to prior studies (emphasis mine):
Virus testing rebound incidence trended higher in the Paxlovid group (18/127; 14.2%) than in the control group (4/43; 9.3%) (Figure 3a and Table 1). Symptom rebound incidence was notably higher in the Paxlovid group (18.9%) than the control group (7.0%). Participants who rebounded also reported less body ache compared to those who did not rebound. There were no notable differences in viral rebound by age, gender, pre-existing conditions, or symptom groups during the acute 16-day follow-up period.
Unfortunately, there’s no breakdown of the duration of viral rebound for each participant so we’re not made aware of the time between negative tests and positive resurgence, or how long the viral rebound lasted.
Interestingly, reports of symptom rebound were far greater in the PAXLOVID group compared to the control group, although this is the only information available describing that phenomenon:
Out of the control group, 2 had a symptom rebound that lasted less than 5 days and 1 had a rebound that was 5 days or longer. In the Paxlovid group 10 had a symptom rebound that was less than 5 days, 10 had symptom rebound that was 5 days or more and 4 had more than 1 symptom rebound during the 16-day follow-up period.
So in parsing the data what can we find?
The evidence here suggests that PAXLOVID rebound may be higher than previously reported in the literature and may be far more common than originally thought, as the percentages here are higher than previous studies.
Viral rebound may be a common feature of SARS-COV2 infection, although there is a lack of investigation and research. The researchers note that the viral rebound in the control group is comparable to other studies.
To the above comments the researchers note the following (emphasis mine):
Our study demonstrated an overall viral testing rebound incidence of 14% and a symptom rebound incidence of 19% among Paxlovid treated cases. Both incidences are higher than have been reported in prior retrospective studies which ranged from 2% to 6% [20, 21]. However, we also show that both viral (9%) and symptom rebound (7%) occurs in the absence of treatment with Paxlovid. Testing rebound in the control group matches reported viral rebound incidence in other studies of untreated patients with COVID-19, which was 12% [11, 17]. A notable finding in our study was that symptom rebound in the control cohort was lower than in the Paxlovid arm.
The last note is rather interesting. We have to keep in mind that the information around PAXLOVID and viral rebound may create more heightened awareness around those prescribed PAXLOVID, and so many of these participants may have been more meticulous in noting any symptoms that they have.
This study was conducted in August 4 - November 1, 2022, so it’s not too far-fetched to assume that PAXLOVID participants may have been influenced to be aware of possible signs of rebound.
However, the viral rebound evidence as supported by the positive antigen tests would infer that more than just biases and influence should account for the symptom onset.
So what exactly is influencing this PAXLOVID rebound?
Brian Mowrey has outlined a factor in PAXLOVID building off of Igor Chudov’s initial works, and as Brian notes the drug may serve as a pause, rather than a stop mechanism which may influence the antiviral response. It’s also the fact that various obfuscation mechanism may be at play which, when the virus’ proteins pass by can immediately return back to ramping out the rest of the stalled proteins and resume replication:

This is likely a framework that many researchers will build off of, and I’ll likely use it in rationalizing the broader viral rebound issue.
However, given that viral rebound is occurring in those not provided PAXLOVID, and that this viral rebound may be seen in those given Molnupiravir we may consider a complex interplay between the host immune system, viral dynamics, and antiviral treatments and how all come together to influence the ebb and flow of an infection.
I find the researchers comment rather apt here:
While Paxlovid treatment reduces severe outcomes [4], the high incidence of viral and symptom rebound in both treated and untreated cohorts suggests that investigation is needed around the changes caused by Paxlovid in the virologic and immunologic milieu of the pathogen and host.
So again, a multitude of processes are occurring all at once. It’s unlikely that researchers will be able to piece together every little mechanism that is involved with the viral rebound and how antivirals may fit into this phenomenon, but there’s likely to be various mechanisms, all intrinsically tied together that contribute to the phenomenon that is viral rebound.
But I’ll save a lot of that pontification for another time.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Anderson, A. S., Caubel, P., Rusnak, J. M., & EPIC-HR Trial Investigators (2022). Nirmatrelvir-Ritonavir and Viral Load Rebound in Covid-19. The New England journal of medicine, 387(11), 1047–1049. https://doi.org/10.1056/NEJMc2205944
This data (and table) comes from a June study which was used as the correspondence in yesterday’s post:
Holly Soares, Mary Lynn Baniecki, Rhonda Cardin et al. Viral Load Rebound in Placebo and Nirmatrelvir-Ritonavir Treated COVID-19 Patients is not Associated with Recurrence of Severe Disease or Mutations, 03 June 2022, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-1720472/v1]
The Paxlovid Rebound Study: A Prospective Cohort Study to Evaluate Viral and Symptom Rebound Differences Between Paxlovid and Untreated COVID-19 Participants
Jay A. Pandit, Jennifer M. Radin, Danielle Chiang, Emily Spencer, Jeff Pawelek, Mira Diwan, Leila Roumani, Michael Mina
medRxiv 2022.11.14.22282195; doi: https://doi.org/10.1101/2022.11.14.22282195
Remember that the EPIC-HR studied used PCR testing and defined a viral rebound as an increase in viral load of at least 0.5 log.
I have to hop out before reading! - but note that EPIC used an IgM inclusive assay so once again these could mostly be early seroconverters. There is a consistency with the divide for the "viral load" PCR results. This was discussed in https://unglossed.substack.com/i/52792651/assay-what
Still not gonna take it, even if I do get covid again.