


In Regards to Omicron
A few comments and open discussion.

Minor correction: On my post about Ba.4/Ba.5 I made a comment that we should look into older monoclonals for current utilize with this new subvariant. However, after thinking about it further I believe that remark was too premature based on the tiny data provided. In order to make such an argument there would need to be further analysis of the epitopes being targeted by the monoclonals (Eli Lily’s and Regeneron). I think I jumped the shark based on the comment made in the Forbes article. So as of now consider this hypothesis shelved until further evidence can be found to substantiate it.
Going into my post on Ba.4/Ba.5 I wanted to make some remarks about the complexities of immunity and how simple analyses or assumptions may not tell us much about anything.
But I also want to use this post to discuss a few things in regards to Omicron and generally the atmosphere surrounding COVID as it exists currently. This post will feel a little bit scrambled since it will likely come together as I form my thoughts, so please bear with me and let’s venture forward.
Because the immunity section was going to end up becoming super long, I decided to split this article up and save the immunity section for the future. Apologies for those looking forward to it! It should be out within a day or two.
The Omicron Enigma
Just like many people out there I was infected with Omicron, and at the time was the only SARS-COV2 infection that I received (at least as far as I am aware of). Nearly everyone from both naturally immune and vaccinated was able to get COVID, and because of that it caught people off guard.
Because of this, it’s rather strange how much of Omicron has been memory-holed.
At the time I wrote a few pieces on Omicron and its emergence, with the general hypothesis in the scientific community being that it was some offshoot of Alpha from long ago, or it may have come from animal reservoirs. In general, we didn’t know where it came from at the time, nor do we know about its origins now.
Considering how the emergence of SARS-COV2 called into question gain-of-function research and possible lab leaks, it only seemed plausible that people consider Omicron itself to be of lab origin.
Brian Mowrey of Unglossed has raised this hypothesis based on the mutation rate, as well as both Ba.1 and Ba.2 emerging at the same time (Ba.1 was able to outcompete Ba.2 until later on).
The Ba.1 and Ba.2 being different variants that emerged separate is very interesting. It alludes to the fact that there may have been a lot of noise that came about during the emergence of Omicron- sounds a bit too familiar to the initial coverage of COVID, right?
In one study by Mykytyn, et. al.1 researchers conducted antigenic cartography through utilizing pseudovirus particles expressing different spike proteins and infecting in vitro cells. Antigenic cartography maps the different responses of cells to the virus and generally provides some insight into the relationship between different variants. The results suggest that, not only are Omicron Ba.1 and Ba.2 very antigenically different than prior variants, but that they are themselves distinct from one another, suggesting either a divergence from a common ancestor or two independent emergences of each variant.

And the researchers provide this comment in regards to results of their neutralization results. Keep in mind that these neutralization assays come with many caveats, but on the basis of being consistent they at least follow the similar design of other studies:
Similar to pseudovirus data, we observed a reduction in neutralization titers of Omicron BA.1 sera against all other variants (2.4 to 9 fold compared to homologous) and poor neutralization of Omicron BA.1 by all non-homologous sera (8 to 112 fold reduction). In addition, Omicron BA.2 was also poorly neutralized by all sera (7 to 114 fold reduction), including Omicron BA.1 (8 fold reduction). Although Omicron BA.1 and Omicron BA.2 possess many overlapping mutations in S, the differences between the variants were sufficient to prevent efficient cross-neutralization. In agreement, our study shows that antibodies elicited against the original SARS-CoV-2 cluster do not neutralize Omicron BA.1 well, and vice-versa.
All this to say, Omicron essentially threw a wrench into everyone’s working model of COVID. No longer could we make the case that natural immunity was better than vaccinated immunity- everyone was getting sick regardless because the virus had mutated so extensively that it evaded nearly all prior immunity.
As another example, take this excerpt from Willet, et. al.2 for another idea of how evasive Ba.1 was be relating the mutations to immune invasion:
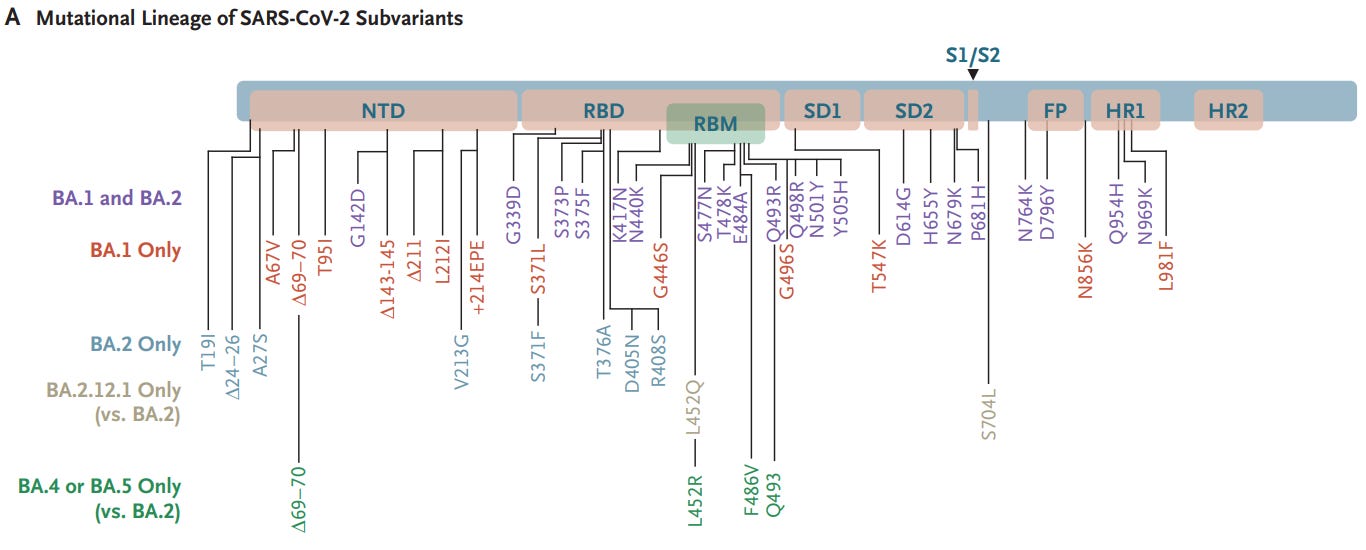
Within the spike protein, BA.1 and BA.2 sub-lineages share 21 amino acid mutations with 12 distinct mutations in BA1 and 6 in BA.2. BA.2 lacks the 69,70 deletion present in BA.1. The G339D, N440K, S477N, T478K, Q498R and N501Y mutations (present in BA.1 and BA.2) enhance binding of spike to the human ACE2 receptor, while combinations such as Q498R and N501Y may enhance ACE2 binding additively19. Deep mutational scanning (DMS) estimates at mutated sites are predictive of substantially reduced monoclonal and polyclonal antibody binding and altered binding to human ACE2 (Fig. 1b)20. Fourteen mutations in Omicron (K417N, G446S (BA.1), E484A, Q493R, G496S (BA.1), Q498R and to a lesser extent, G339D, S371L/F (BA.1/BA.2), S373P, N440K, S477N, T478K, N501Y and Y505H) may affect antibody binding on the basis of a calculated escape fraction (a quantitative measure of the extent to which a mutation reduces polyclonal antibody binding by DMS). Seven Omicron RBD mutations (K417N, G446S(BA.1), E484A, Q493R, G496S(BA.1), Q498R and N501Y) have been previously shown to be associated with decreased antibody binding, importantly falling in epitopes corresponding to three major classes of RBD-specific neutralizing antibodies (nAbs).
So there was a general expectation that nearly no one would be “fully” protected from Omicron, and as I recall the general sentiment at the time was to say that Omicron almost created an even playing field for the world. We were starting at square one, and fortunately for most us Omicron was mild so there was a general sentiment that this would be the beginning of the end for COVID.
But how many people reading this actually remember that this was a thing; that we (rightfully) took Omicron as some measure of immunity reset for the world? Why was it that there was no reworking of our understanding of COVID in the wake of Omicron?
Instead, it appeared that many eventually settled into Omicron and viewed it as a continuation of Delta, even thought it contained several dozen new mutations that absolutely does not follow the typical mutation rate one would expect for a naturally occurring virus (as natural as a virology lab in Wuhan can be considered natural).
Again, compare the mutations found in the spike protein of Alpha, Beta, Delta, and Omicron using the chart below from Lippi, et. al.3 Then compare the chart from Wednesday showing the mutations between Ba.1/Ba.2 and other subvariants of Omicron4.

Such a high degree of mutations (Note: there are more mutations in Ba.1’s receptor binding domain than there are mutations in the spike protein of other variants) requires some degree of contextualization, and one that takes into account how to go about parsing this high degree of mutations.
Do we try to find reasons to suggest why these mutations came about? Some suggest zoonotic jump from mice and rats as an explanation as to why these mutations in particular came about, yet there hasn’t been any evidence of mouse zero running about in South Africa. It may be from an immunocompromised individual, but that doesn’t explain why mutations that confer greater transmissibility yet lower virulence would be favored unless the net fitness favored these mutations, as well as why surveillance somehow did not see the emergence of some ancestral lineage (if the patient received longterm treatment). Both hypotheses don’t also take into account how both Ba.1 and Ba.2 emerged around the same time yet are so distinct from one another. That would generally leave us with a lab-based theory, whether released intentionally or a possible leak. In all cases though, it doesn’t follow the typical route through human serial passage, and so does it seem appropriate to include Omicron into the human evolutionary model?
This creates a host of problems, mostly because Omicron means that we can’t draw a line from Delta to Omicron- we can’t connect the dots and follow an evolutionary progression from one variant to another. In fact, this may be considered the improper inclusion of Omicron, and yet it appears to be happening everywhere.
Many models on COVID now just include Omicron rather than treating it as a separate entity to which we don’t know the origins of. Hypotheses now work around Omicron’s more transmissible yet reduced virulent nature to extrapolate assumptions. Now that Ba.4 and Ba.5 are appearing with greater virulence, it’s suddenly as if the Delta→ Ba.1/Ba.2 → Ba.4/Ba.5 line of viral progression is somehow something that was predicted for by several, as if they somehow knew that a variant like Omicron would arise when many have raised concerns about possible lab origins for this variant.
It’s even strange seeing many people remark that Ba.4 and Ba.5 are now the time where immune escape is happening, especially since immune escape was happening as soon as Omicron emerged and is not exclusive to this current subvariant. Again, more memory-holing appears to be at play here. Granted, there is an argument to be made that the combination of mutations found within Ba.4/Ba.5 are what makes the immune escape, but since this appears to be the general progression of viruses that find niches within humans (i.e. mutate to evade immunity), this may not be a surprise more than something that should be expected.
Even with this steelman, there are a few questions (as raised by Brian Mowrey) as to whether Ba.4/Ba.5 are actually distinct from Ba.2 as well5.
Omicron has become a conundrum for the scientific community and many others, yet it’s treated as if it’s not the anomaly that it should be designated.
It’s as if Omicron is being treated as the estranged child that has been welcomed into the COVID family, not some random stranger that appeared at the family picnic and eats all of the coleslaw and macaroni salad while Auntie Alpha looks on wondering who’s kid this is that just appeared out of nowhere.
In that regard, it doesn’t quite make sense how Omicron has inserted itself so seamlessly into the COVID discourse. Instead, it may be more viable to consider Omicron and Wuhan as completely separate viruses (to a degree), if not for the difficulty of figuring out exactly what to do with Omicron. This does raise problems of its own, but it should at least emphasize the fact that Omicron’s analysis may be biased by our analyses of prior variants.
There’s likely more I intend to say here that I can’t think of at the moment, but keep in mind that when parsing the information we should remember the strange emergence of Omicron and factor that into our working model, rather than disregard it’s sudden appearance and act as if it was just the normal state of affairs.
With that, I would like to know what you all think about Omicron given everything that has been going on.
Do you think Omicron emerged from animal reservoirs, or emerged from an immunocompromised individual? Or is there a possibility that Omicron, similar to the original Wuhan, may have emerged from a lab?
How do we contextualize the enigma that is Omicron? How do we relate it to prior variants, or should we consider it completely separate? If we do include Omicron with respect to variants such as Delta, how do we rationalize the high number of mutations that have still not been fully answered?
Consider these questions, and any other questions and think about opening up some discussion about what’s going on. I’ll try to release my immunity post either tomorrow or Sunday, so please be on the lookout for that!
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Omicron BA.1 and BA.2 are antigenically distinct SARS-CoV-2 variants
Anna Z. Mykytyn, Melanie Rissmann, Adinda Kok, Miruna E. Rosu, Debby Schipper, Tim I. Breugem, Petra B. van den Doel, Felicity Chandler, Theo Bestebroer, Maurice de Wit, Martin E. van Royen, Richard Molenkamp, Bas B. Oude Munnink, Rory D. de Vries, Corine GeurtsvanKessel, Derek J. Smith, Marion P. G. Koopmans, Barry Rockx, Mart M. Lamers, Ron Fouchier, Bart L. Haagmans
bioRxiv 2022.02.23.481644; doi: https://doi.org/10.1101/2022.02.23.481644
Willett, B.J., Grove, J., MacLean, O.A. et al. SARS-CoV-2 Omicron is an immune escape variant with an altered cell entry pathway. Nat Microbiol (2022). https://doi.org/10.1038/s41564-022-01143-7
Lippi, G., Mattiuzzi, C. & Henry, B. (2022). Updated picture of SARS-CoV-2 variants and mutations. Diagnosis, 9(1), 11-17. https://doi.org/10.1515/dx-2021-0149
Hachmann, N. P., Miller, J., Collier, A. Y., Ventura, J. D., Yu, J., Rowe, M., Bondzie, E. A., Powers, O., Surve, N., Hall, K., & Barouch, D. H. (2022). Neutralization Escape by SARS-CoV-2 Omicron Subvariants BA.2.12.1, BA.4, and BA.5. The New England journal of medicine, 387(1), 86–88. https://doi.org/10.1056/NEJMc2206576
Both Ba.1 and Ba.2 were detected and sequenced in November 2021. Ba.4 and Ba.5 were detected in January, although there is a possibility of their existence from earlier on. Remember that these strains are all derived from similar geographical regions, which would at least lend some value to the idea that all of the sublineages of Omicron may have come about around similar times rather than from one another.
https://www.nicd.ac.za/omicron-lineages-ba-4-and-ba-5-faq/
This is a great, thoughtful post. Just like you, I was wondering, how come a brand new variant, without anything intermediate, appeared out of nowhere?
I wrote an article on Dec 3 and then another:
https://igorchudov.substack.com/p/urgent-omicron-variant-likely-to
https://igorchudov.substack.com/p/omicron-as-a-bioweapon-thoughts-and
I did, and still do, have doubts as to mildness of Omicron. For example, Ba1 and Ba2 appeared at almost the same time. But it took Ba1 to "bust the gates" open for Ba2 to take hold some months later and start reinfecting people.
What exactly did Ba1 do, to make people more susceptible to Ba2? Nobody knows. There is a lot of mysteries in Covid-19 that people are not even perceiving as mysteries.
Is Covid mild if each reinfection kills 20% of lymphocytes andmonocytes?
In addition, there are several narratives. The "lab origin" narrative says that Covid and many variants all come from a lab. Another says that Covid is undergoing natural evolution and "Omicron proved Geert was right". Well if they all came from a lab, there is no evolution!
The truth is probably somewhere in the middle.
Nowadays, Geert and many people say that "Covid is regaining virulence". But perhaps it is reinfections that make people sicker and sicker, as opposed to innately higher vorulence. Lots of stuff to think about.
P.S. I and my son did NOT have Omicron despite zero preventative measures. We are both unvaxed and had Covid earlier (Nov 2020 for me and Apr 2021 for him)
The first thing to do for those infected with COVID-19, or who have sepsis, Kawasaki disease, MIS-C or any other clinital emergency is to get their circulating 25-hydroxyvitamin D up to at least 50 ng/mL 125 nmol/L. Any less than this and their immune system cannot work as effectively as it should against viral, bacterial and fungal pathogens. Low 25-hydroxyvitamin D levels also increase the risk of wildly dysregulated hyper-inflammatory responses, which kill cells indiscriminately. This drives sepsis, severe COVID-19, KD and MIS-C. In severe COVID-19, inflammation damages the endothelial cells in the lungs (which line the blood vessels and capillaries). This causes the blood to become hyper-coagulative. The resulting microembolisms worsen the hypoxia caused by the inflammation and damage the lungs, brain, spinal cord, heart and all other organs.
The best approach to COVID-19 and numerous other health problems is proper vitamin D3 supplementation so all people have at least 50 ng/mL 25-hydroxyvitamin D all year round. Without proper supplementation, most people have 1/10th to 1/2 of this. If this is not done, then those infected need a 4 hour boost of 25-hydroxyvitamin D by ingesting a single oral dose of calcifediol (which _is_ 25-hydroxyvitamin D: 0.014 mg per kg body-weight, which is 1 mg for 70 kg 154 lb average adult body-weight. If calcifediol is not available, bolus vitamin D3 should be used, such as a single dose of 10 mg 400,000 IU. This takes about 4 days to boost 25-hydroxyvitamin D safely over 50 ng/mL, due to the delays inherent in it being hydroxylated in the liver to 25-hydroxyvitamin D.
Except for those few people today who have 50 ng/mL or more 25-hydroxyvitamin D, no other treatment matters more than calcifediol or bolus vitamin D3 to attain this level. Magnesium, zinc, vitamin C, B vitamins and probably vitamin A are also important early nutritional interventions: https://c19early.com . Ivermectin, quercetin and other early treatments are also likely to be helpful, safe and easy to obtain.
Only then should anyone bother to fuss about monoclonal antibodies, or any of the other patented, profitable, treatments. None of them are more urgently important than meeting the immune system's nutritional needs.
Please read the research articles cited at: https://vitamindstopscovid.info/00-evi/ , the list of early treatments (with only the expensive ones FDA approved) at: https://nutritionmatters.substack.com/p/the-fda-cdc-and-most-other-western and the calcifediol or bolus D3 treatment at: https://nutritionmatters.substack.com/p/calcifediol-to-boost-25-hydroxyvitamin .
All sound too simple? Read the research!