


Hydroxychloroquine: An Overview
Part II-1: Evidence as Treatment Against SARS-COV2

Here, I’ll go into more detail about Hydroxychloroquine as a therapeutic against SARS-COV2. This will include a few more specific mechanisms of action, in vitro activity, pairing with zinc and Azythromicin, and examining the evidence in a clinical setting.
Although most studies with HCQ looked at it paired with Azithromycin or alone, the clinical data that will be included will look mostly at dual therapies (either with Azithromycin or Zinc) since most proponents of HCQ usage argue that supplementation with Zinc is vital to its antiviral activities.
Mechanisms of Action against SARS-COV2
As I previously highlighted Hydroxychloroquine seems to work by both targeting lysosomes and eliciting antiviral properties there, as well as operating as an immunomodulator and reduce the cytokine storm that forms in later disease progression.
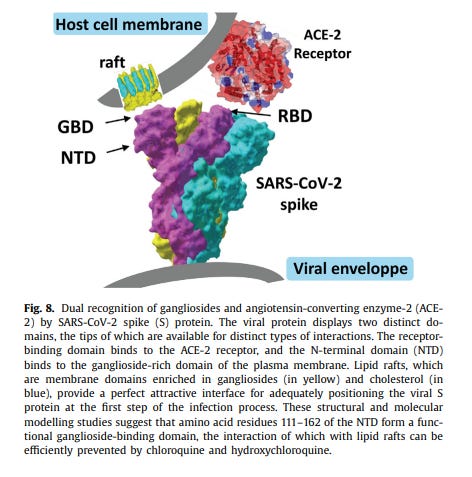
However, it seems like there may be another target for Hydroxychloroquine. Although the main focus with receptor binding has examined the dynamics between the virus’ spike protein and the ACEII receptor, the SARS-COV2 viral particle most likely requires the assistant of other host membranous structures in order to facilitate attachment and viral entry.
One group that seem to be responsible is called sialic-acid containing glycoproteins (proteins that contain carbohydrates) and gangliosides (lipids bonded to sugars), and it seems that both Chloroquine and Hydroxychloroquine may bind to these glycoproteins/gangliosides and inhibit the binding of SARS-COV2’s spike protein.
Computer modeling conducted by Fantini et. al. 2020 suggests that both Chloroquine and Hydroxychloroquine share similar molecular motifs to parts of SARS-COV2’s spike protein. By looking similar to parts of the spike protein that may be responsible for binding to host cell gangliosides, CQ and HCQ may be able to bind to these gangliosides and inhibit binding of the spike protein itself.

Unfortunately, this study was based on computer modeling, meaning that this mechanism of action may not actually occur in vitro or in animal models. However, the researchers did indicate greater binding affinity of HCQ compared to CQ, which correlates with HCQ’s supposed higher efficacy. So this does indicate another possible mechanism of action of HCQ, one that may be specific to SARS-COV2’s viral entry into host cells.
A Tale of Dual Therapies: Zinc and Azithromycin
Commentary around HCQ usually did not involve the drug alone, but instead usually paired with another compound, either the mineral Zinc or the antibiotic Azithromycin. Here, we’ll take a look at both and examine their mechanisms of action.
HCQ and Zinc
Zinc has been known to have antiviral properties, but more importantly it seems to be very effective against respiratory diseases. There also is some evidence that Zinc could be effective against SARS-COV2.
As noted in a review by Skalny et. al. 2020 (emphasis mine):
Specifically, Zn2+ cations especially in combination with Zn ionophore pyrithione were shown to inhibit SARS-coronavirus RNA polymerase (RNA dependent RNA polymerase, RdRp) activity by decreasing its replication (39). These important findings demonstrate that Zn2+ may be considered as the particular antiviral agent in COVID-19 treatment. Of note, recent trials have indicated efficiency of chloroquine antiviral activity as a treatment of COVID-19 (40), although the intimate mechanisms of its antiviral activity require further investigation (41). Earlier findings demonstrate that chloroquine is a zinc ionophore increasing Zn2+ flux into the cell (42). Moreover, the authors also propose that chloroquine-mediate zinc influx may underlie anticancer activity of the compound (42). Similarly, it was hypothesized that increasing intracellular Zn2+ concentration by chloroquine may also mediate its antiviral effect against SARS-CoV-2. In this view zinc supplementation without chloroquine might have similar positive effects without adverse side-effects of chloroquine treatment (43). Hypothetically, such an effect may be also observed using other zinc ionophores like quercetin and epigallocatechin-gallate (44) with substantially lower toxicity, although clinical trials supported by experimental in vitro studies are required to support this hypothesis.
Another Zn-related approach to modulation of COVID-19 may include targeting Zn ions in the structure of viral proteins. Particularly, it has been demonstrated that disulfiram-induced Zn2+ release from papain-like protease in MERS-CoV and SARS-CoV resulting in protein destabilization (45). In view of the presence of similar critical Zn-containing sites, Zn-ejector drugs (e.g., disulfiram) may be considered as potential antiviral agents (46) and components of targeted oxidation strategy in anti-SARS-CoV-2 treatment (47).
As indicated above, HCQ is considered to be a Zinc ionophore, meaning that HCQ may play a more passive role by helping facilitate Zinc movement into infected cells. Greater Zinc levels may elicit greater antiviral activity against SARS-COV2.
This evidence is supported by an in vitro study by Xue et. al. 2014, in which greater intracellular Zinc levels were achieved with coadministration with CQ.

T his may indicate a synergistic effect where HCQ may elicit antiviral effects in conjunction with Zinc.
Unfortunately, clinical trials with HCQ and Zinc seem to be spotty.
Zinc Clinical Trials
In a study conducted by Carlucci et. al. 2020 a combination therapy of Zinc with HCQ lead to better hospitalized patient outcomes compared to those who took HCQ alone.

However, a study conducted by Abd-Elsalam et. al. 2020 indicated that there was no statistical significance between a group treated with the combination Zinc/HCQ therapy versus HCQ alone.
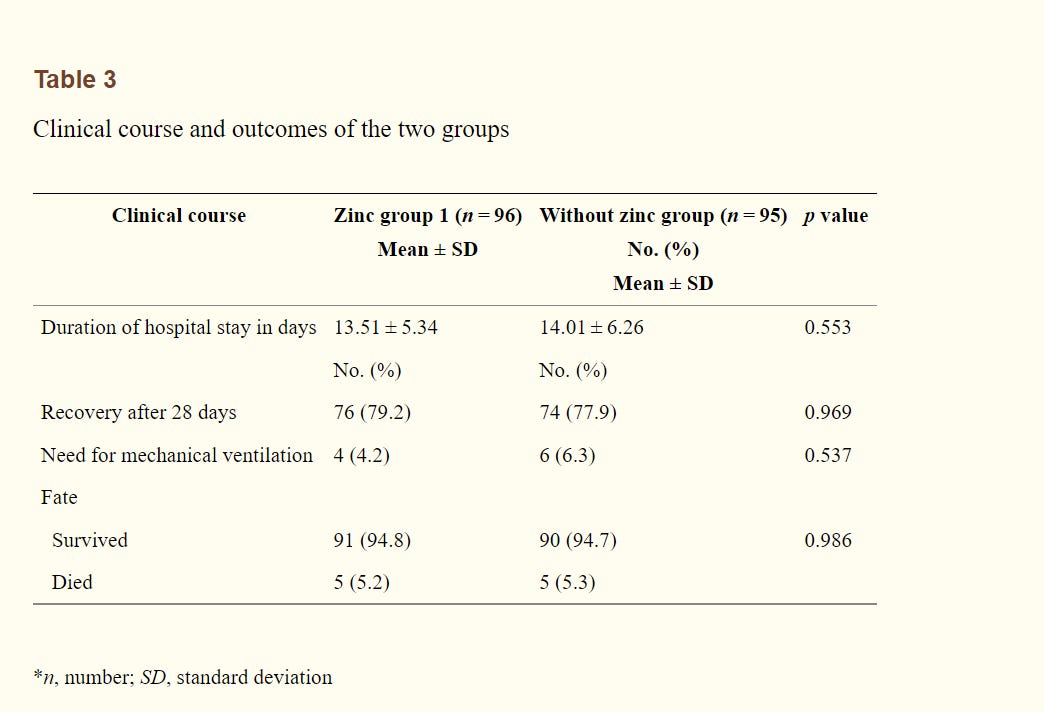
One thing to note is that these studies were done in a hospitalized setting, and at that point use of antiviral therapeutics may not be as effective as early treatment (as many HCQ/Zinc advocates suggest). This, once again, may point more to the idea that early treatment may be a lot more beneficial than when used in a hospital setting, although early treatment/prophylactic studies are difficult to find.
HCQ and Azithromycin
Azithromycin is a macrolide antibiotic that is used to target bacterial ribosomes during an infection, and its use with COVID may have stemmed from a concern about secondary infections that may arise during later COVID disease progression. However, it seems that its mechanism of action may be based more on a synergistic effect with HCQ. More specifically, both seem to play an important role in a process called ion-trapping.
Many functional groups of compounds can exhibit acidic or basic properties. Usually, these functional groups are assigned a pKa value, indication the group’s potential to act as an acid, and is usually used as a comparison to environmental pH (acidic levels of solution/environment).
For example, carboxylic acids tend to have pKa values around 4-5 while amines tend to have pKas around 9.
When it comes to our bodies, which have a pH slightly above 7 (~7.4) we refer to this as physiological pH, and it helps to determine whether or not certain compounds will behave as an acid or base in our bodies (note that the 7.4 is a general number; regions like the stomach will have a much lower pH).
A good rule of thumb when comparing pKa to pH is thus:
pKa < pH: in this instance the functional group remains “protonated” (keeps its hydrogen atom)
pKa > pH: in this case the functional group becomes “deprotonated” (a hydrogen atom is removed from the group)
Why is all of this important? I indicated that HCQ and its derivatives tend to target lysosomes, which are highly acidic. What seems to happen is that HCQ, with several amine groups (pKa ~9) will act as a base within lysosomes (pH ~ 5) and increase the environmental pH, rendering the lysosome unusable. More importantly, when HCQ enters into a lysosome and becomes protonated it cannot leave (charged molecules have difficulty moving across membranes), meaning that HCQ is essentially “trapped” inside the lysosome due to its ionic nature (hence ion-trapping).
It seems that both Azithromycin and HCQ are capable of engaging in ion-trapping, as hypothesized by Derendorf, H. 2020.

And a similar mechanism was proposed by Scherrmann, J. M. 2020, except it was alluded to that Azithromycin uptake may also be regulated by a transporter protein called ABCB1, and that uptake of Azithromycin may help to facilitate HCQ uptake (emphasis mine):
To sum up, the intracellular ABCB1 could represent a potent target for enhancing the antiviral and anti-inflammatory activities of the aminoquinolines when lysosomotropic ABCB1 substrates like azithromycin or ciprofloxacin are combined. This could explain why the association strategy leads to apparent rapid virus clearance and better clinical benefit vs. aminoquinoline use alone (1). Moreover, these observations justify the bi-therapy administration in the early stage of the disease or for prophylactic use, i.e., when the virus distributes within the disease target cells, such as the pulmonary epithelial cells. Experimental assessments of this hypothetical ABCB1 role could be easily investigated using both in vitro cellular models currently used with SARS-CoV-2 and widely developed for ABCB1 transport (19,20,46,50). Moreover, the reported co-localization of ABCB1 with other ABCs on the lysosomal membranes, such as ABCG2, ABCC1, and ABCC2 could also expand this experimental field of investigation as to their possible involvement in the activity of these lysosomotropic drugs (51).
Azithromycin Clinical Trials
Some of the first reported clinical trials involving combination HCQ/Azithromycin came from France. In one study (Gautret et. al. 2020) use of both HCQ and Azithromycin lead to a significant decrease in viral levels as compared to placebo, although this trial had a small sample size (N=42) and was an open-label, non-randomized trial. Another retrospective analysis conducted by Lagier et. al. 2020 indicated that early treatment with HCQ/Azithromycin lead to better clinical outcomes and quicker viral clearance. These results were also seen in Million et. al. 2020 with better clinical outcomes and reduced mortality in the group given the combination therapy.
These early results proved very promising, and they also highlighted that early treatment plays a vital role in improved outcomes.
However, the overall data may not be as clear.
A meta-analysis conducted by Fiolet et. al. 2021 indicated that HCQ usage did not lead to statistically significant better outcomes, and that combination therapy actually lead to increased mortality.
One of the most cited articles on HCQ/Azithromycin usage was reported by Cavalcanti et. al. 2020, in which hospitalized patients were either administered HCQ alone, in combination with Azithromycin, or provided placebo. Results indicated that neither HCQ alone nor in combination with Azithromycin lead to better clinical outcomes 15 days after administration. Note that this study was open-labeled, and the inclusion criteria had a wide acceptance margin (participants could have tested positive up to 14 days before trial).

Sorry, but this post became too long- it will be continued in another newsletter (Same part, but will be labelled with (Continued)).
Thank you for reading my newsletter. If you enjoy my articles please consider becoming a free subscriber in order to receive notifications.
And share with others who may find these newsletters interesting.
Also, please consider becoming a paid member. The research and work put into these articles takes many hours and being a paid subscriber allows me to continue to do this full time.
Dear Modern Discontent,
Thanks very much for your articles with such in-depth analysis of the most pertinent topics, based on your obviously long experience with and interest in molecular biology and on your energetic research of the latest developments.
I have not had time to read your recent articles fully and I look forward to doing so.
For me, and I guess some or many other readers, there's no need to apologise for length or how many articles it takes to properly cover a topic.
Best regards
Robin Whittle