


Everyone is Getting COVID. It’s time to learn and deal with the virus.
PART III: Repurposed Drugs, A Culture of Shaming, and Citations

A Brief Look at Repurposed Drugs
Drugs are designed to target specific aspects of either the host’s cells or to target the pathogen directly. As a pathogen’s dynamics change, it should be expected that viable therapeutics be reassessed to determine which ones should be more effective. We have already seen this happen with monoclonal antibodies, so we should expect a similar reassessment with off-label/repurposed drugs.
Now, I will not speak to the effectiveness of these therapeutics, but will discuss them more from the pharmacodynamic perspective and provide a brief overview for the important mechanisms of action.
Here, we will look specifically at Hydroxychloroquine and Fluvoxamine.
In Heather Heying’s Omicron newsletter, she commented that she was prescribed Ivermectin for her infection and experienced a rare side effect of visual disturbances. Because of this, her prescription was changed to Hydroxychloroquine. She commented that Hydroxychloroquine is expected to be more effective than Ivermectin in dealing with Omicron due to its mechanism of action.
I have extensively written about Hydroxychloroquine, and so I will point to my Hydroxychloroquine Anthology Series for a deeper examination of the drug. Instead, I’ll talk specifically about Hydroxychloroquine’s main mechanism of action against Omicron, which is actually is proposed main mechanism of action in general.
With Omicron, it appears that its main method of viral transmission is through cell-to-cell transmission, likely through the utilization of the endosomal pathway.
The endosomal pathway is part of the overarching endocytic pathway. The endocytic pathway describes the cellular trafficking pathway that shuttles objects into and out of a cell and depends upon many cellular organelles that make up the endosomal pathway. This includes endosomes themselves, which are membrane-bound organelles responsible for helping traffic molecules and structures. This also includes lysosomes, which are vesicles that digest foreign objects and pathogens for elimination and removal.
The main mechanism of action of chloroquine analogues is to target the endosomal pathway. Hydroxychloroquine is a weak base, and when it enters into lysosomes it immediately becomes protonated. The increase in lysosomal pH causes lysosomes to not function properly, essentially shutting off the endosomal pathway from carrying out its duties. It’s through this mechanism of action that chloroquine analogues elicit both their antimalarial and immunomodulatory properties, and it’s also the likely mechanism of action against Omicron. As Omicron relies on shuttling through host cells by utilizing the endosomal pathway, shutting down this pathway will prevent viral particles from spreading to uninfected cells.

To add a little bit more information, here is an excerpt from Al-Bari, 2017:
Chloroquine analog is a diprotic weak base. The unprotonated form of chloroquine diffuses spontaneously and rapidly across the membranes of cells and organelles to acidic cytoplasmic vesicles such as endosomes, lysosomes, or Golgi vesicles and thereby increases their pH (Al‐Bari 2015). On oral administration, the analog is readily absorbed and concentrated in tissues such as the liver, spleen, and kidney (Al‐Bari 2015)‐ where several fatal viruses harbored, replicated, and infected (Geisbert et al. 2003). In cellular levels of the tissues, chloroquine becomes highly concentrated in such acidic organelles leading to dysfunction of several enzymes, e.g. those required for proteolytic processing and post‐translational modification of viral proteins (Fig. 1) (Savarino et al. 2003; Marzi et al. 2012). Consequently, chloroquine analogs inhibit the production of several cytokines, chemokines or mediators, whose excessive appearance contributes the severity of viral infections. Therefore, the inhibition of endosomal acidification by chloroquine analogs may become a potential therapeutic strategy for viral infections and associated pathologies.
The increasing evidence suggests that the entry, replication and infection processes of several viruses such as Ebola, Marburg, dengue, Chikungunya, HIV etc. are highly dependent on endosomal‐lysosomal acidification and the activities of several host endosomal proteases ‐ which are also active in acidic pH environments (Sun and Tien 2012; Barrow et al. 2013). By neutrality of acidic pH in endosomes, chloroquine analogs inhibit these viral entry and replication processes into the cytoplasm of susceptible cells and thereby abrogate their infections (Chiang et al. 1996; Savarino et al. 2003).
So that leaves us with Fluvoxamine. Many people have discussed the use of Fluvoxamine in helping with COVID, and it may prove useful in those experiencing long-COVID symptoms. So how is it that an anti-depressant can target SARS-COV2 and elicit some antiviral properties?
I’m planning on writing about Fluvoxamine as my next series so I’ll save most of my information for that post and will provide a brief description here.
Although Fluvoxamine is mostly known as a selective serotonin reuptake inhibitor (SSRI), Fluvoxamine actually elicits many different activities aside from acting as an anti-depressant.
Surprisingly enough, as can be seen by Fluvoxamine’s amine and similar structure to Hydroxychloroquine, Fluvoxamine is able to target the endosomal pathway in a similar manner as well by increasing the pH of lysosomes and altering the endosomal trafficking route.
As indicated by Sukhatme et. al.:
S1R agonists like FLV and fluoxetine are lysosomotropic (Hallifax and Houston, 2007; Kazmi et al., 2013). Fluvoxamine has a predicted pKa of 8.86 (DrugBank, 2005; Wishart et al., 2018) and is susceptible to protonation in the physiological pH range. Less polar, unionized form of basic drugs can easily cross membranes. Basic drugs like FLV can get protonated in the lysosome, which hinders the now-charged moieties from crossing membranes. β-coronaviruses, like SARS-CoV-2 and mouse hepatitis virus (MHV), use lysosomal trafficking to escape from infected cells (Ghosh et al., 2020) (Figure 1). GRP78/BIP, a chaperone that facilitates coronavirus infectivity (Chu et al., 2018; Ha et al., 2020), is co-released with β-coronaviruses through this pathway (Ghosh et al., 2020). The SARS-CoV open reading frame protein 3A (ORF3a) (Gordon et al., 2020) is a viroporin that localizes to lysosomes (Ghosh et al., 2020), disrupts their acidification (Yue et al., 2018), and contributes to viral egress (Lu et al., 2006; Castano-Rodriguez et al., 2018; Yue et al., 2018). Given the lysosomal egress of β-coronaviruses from infected cells, lysosomotropic drugs like FLV could have antiviral effects in the virus laden lysosomes (Homolak and Kodvanj, 2020) (Figure 1).
Both Fluvoxamine and Hydroxychloroquine target Omicron at a pathway that it is likely to utilize to a greater extent than prior variants. Although we do not have evidence of trials with respect to these therapeutics and Omicron, we can suspect that they are likely to be more effective when used early on in the disease (I should remind everyone that we are speculating here).
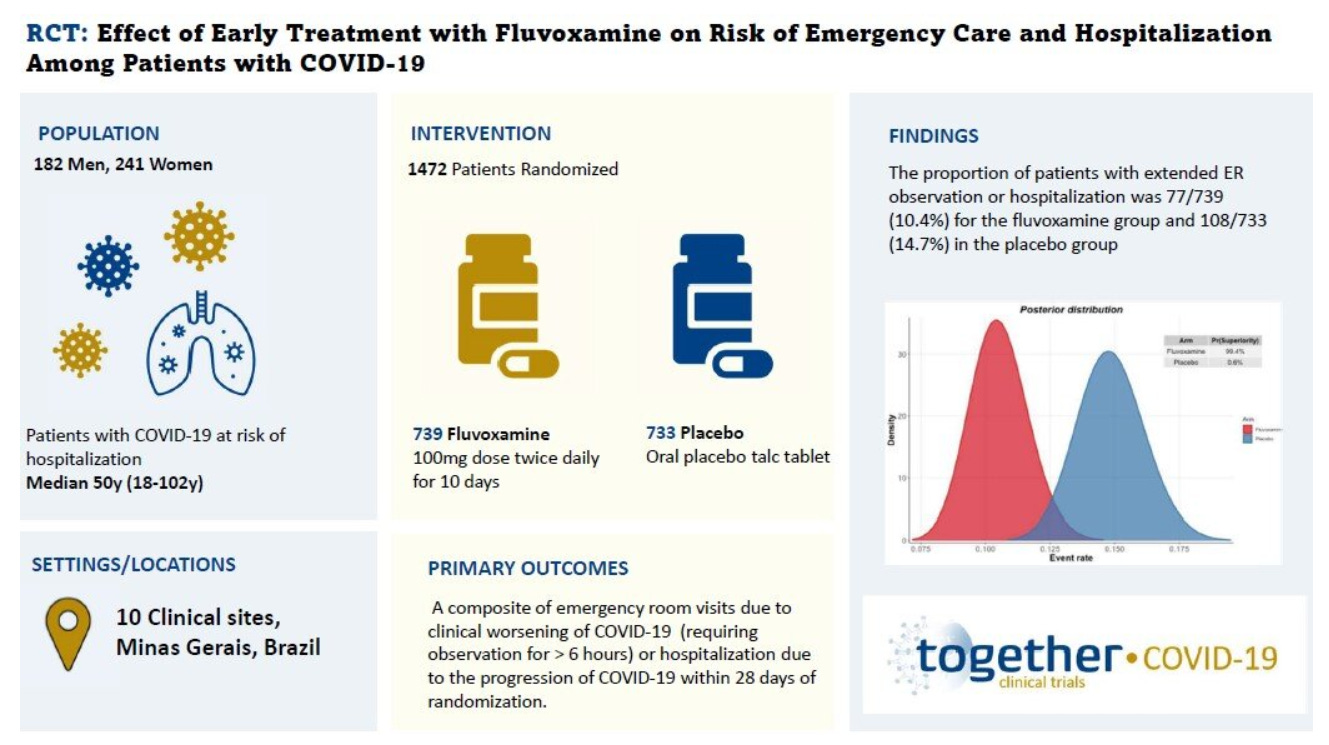
Unlike supplements or over-the-counter options, repurposed use of any prescription medication has been heavily criticized. What’s even more strange is that, in nearly all aspects, Fluvoxamine has been considered an effective treatment by many and was considered one of the only effective treatments in the TOGETHER Trial.
So how is that Fluvoxamine, a drug that is considered safe and has even been considered effective by many governments and trials, still not being adopted as a drug in the COVID arsenal? It’s hard to argue why, although it doesn’t appear that there could be any valid reason against Fluvoxamine. It’s frustrating to see that repurposed, inexpensive drugs have to overcome such a high barrier while brand new, expensive drugs with unknown toxicities are allowed to gain EUA approval. Dr. Pierre Kory has even just made a post about Fluvoxamine, so please take a look at that as well on his Substack.
Take into consideration that PAXLOVID and Molnupiravir are still not seeing widespread use, and by the time it does come to market we may be over the Omicron wave, and that the safety profile of these new therapeutics are still an area of concern, then we can clearly see that many of these policies are doing nothing more than to harm patients who would like to at least try something. More importantly, the approval of Molnupiravir should indicate that there’s something more going on than the purported “safe and effective” mantra that have been used to justify the use of certain therapeutics.
Remember what Kim Iversen stated in her video; people would rather try something even if it provides marginal benefits, rather than try nothing at all. We have essentially been placed into a position by the CDC and FDA where we have tried nothing and are all out of ideas, and acting as if we really have things under control or still insist on blaming the unvaccinated for all of the rampant infections.

Heads up again, but everyone is getting Omicron, vaccinated or not, and because of that we should stop blaming the unvaccinated and blame those who still decide to sit on their hands and not provide any reasonable guidelines for dealing with the infection, or providing any form of substantive information that people can use to make their own decisions.
We have outlined plenty of options here, none of which are mentioned in mainstream circles as possibilities. As Omicron waxes and wanes in many regions of the world practical, accessible remedies should be taken into consideration, even if they are likely to provide little benefit. Something is better than nothing, and nothing is all we’re expected to do, and unfortunately for several people by the time any type of intervention is attempted it may be far too late.
It’s Time to End the Shaming
So before I provide my concluding remarks, I would like to explain why I decided to make this post.
When writing this post I was actually going to take it into a completely different direction. Fortunately, I decided not to as it was likely to provide too much personal information. What I will state is that many people I know have gotten COVID in January including many family members. It became really hard to find any friends or family members who did not get COVID within the past few weeks.
But what was alarming to me was how many of these friends and family kept quiet about being ill. Most of this information came to us through the Asian Rumor Mill (we’re a gossipy bunch, for those who don’t know) rather than through direct conversations.
Now, I personally don’t care who got COVID. As is well-known by now we are all getting Omicron at some point, so there’s no point in being concerned about getting it. What I found so strange was the idea that so many people have kept their infections secret, including those who we have come into contact with.
My original post was going to go into detail about a conversation I had with someone I knew, who reached out to me to tell them that their family was sick and that my family should get tested. This person made a remark that their family did not want to tell us because they were too “prideful” to tell us that they were sick.
What this person didn’t seem to understand was that this was not pride, and in fact was a prime example of shame. It’s an example that so many people getting COVID are ashamed of themselves, as if they had committed some cardinal sin against society and have themselves become a victim of a plague, and someone who should be considered one of the “untouchables” in society’s eyes.
I’m sure many of us have come across Twitter posts of staunch COVID followers who ended coming down with COVID themselves. These people have lamented the fact that they thought they did everything right; they wore masks, they stopped seeing family members, they got vaccinated and boosted, and they somehow still came down with COVID. It’s a prime example of the pride before the fall; those who have bought into the COVID narrative so deeply that they can’t fathom the idea that they eventually got sick- how could doing everything “right” turn out so wrong?
The histrionics and performative dance that so many have attempted to follow for the past two years have done nothing but to instill an ideology of puritanism, rather than rationality. Many have thought that they would be untouched if they followed the guidelines and did whatever was asked of them, who now have to live with the cognitive dissonance that everything that they thought would work did, in fact, not work. What’s an even greater misfortune is that these people have not been provided the tools to make sense of their situation and understand that the policies and guidelines that have been implemented have been both severely flawed and impractical.
Even now, so many people continue to believe that the vaccine would prevent them from getting ill. What a shock for so many who may have bought into this lie and now are surprised that they did, in fact, still get sick. It’s even more alarming that many people who have lived in fear of constant variants and mutated strains of COVID also don’t appear to understand that Omicron is so far removed from prior variants that we can’t use the same line of logic for Omicron as we have for prior variants.
So many people have remained silent about getting infected, rather than informing others as a precautionary measure because they are concerned that they would be chastised for falling ill, as only those who don’t follow the puritanical policies are the only ones to get the disease. As a society we have never condemned those who have gotten seasonal colds and flus, and in fact it’s an expected part of the winter season. The same can’t be said for COVID even when we have such a high transmissible variant.
Let’s be clear here; everyone is going to get COVID now, and we need to learn how to deal with it, rather than feeling ashamed that we have somehow done something wrong. As the saying goes, there’s no point in crying over spilled milk. Those who haven’t gotten COVID yet need to learn that they can’t engage in paranoia, but should instead learn how to properly deal with the virus.
It’s a shame that so many people have felt the need to be ashamed for contracting a virus. At some point people need to realize that there’s no shame in getting sick, that they need to focus on getting better and moving on with their lives.
So if you are someone who finally comes down with the sickness, do not feel any shame for finally getting COVID. It’s bound to happen to most of us at this point. More importantly, don’t feel ashamed to alert people such as your employer than you have fallen ill. If your employer engages in histrionics, try to engage in a more rational approach to calm down the paranoia. For employers, they should also understand that freaking out at employees who end up contracting COVID does no good. In fact, you’re likely to create an atmosphere where no one wants to come forward with being ill for fear of retaliation for getting sick, and thus creating an environment where everyone at work will try to argue “it’s just the cold” instead of staying home.
So do not feel ashamed, and don’t let others shame you. It’s about time people act like adults and stay level-headed and rational.
Dealing with Omicron
A lot of what I have written in these posts have not changed much from prior posts.
When it comes to Antigen or PCR Tests, care must be taken to understand the extend to which these tests are able to measure what is intended. Both should be used at the early stages of the infection, with PCR tests being far more sensitive and would provide results before Antigen tests, which may not be accurate until several days into the disease onset. Unfortunately, these tests may cause problems when used as a measure for whether someone has gotten over their illness. Here, shedding viral fragments may obscure results as there is no way of discerning if these people would still be considered infectious.
Whether or not vitamins, supplements, or at-home remedies do work against COVID is besides the point. Modernity has created a generation of people who are overfed and undernourished, and so many people are likely to be vitamin deficient anyways. We are also still within our winter season here in the Northern hemisphere, meaning many people are more likely to be vitamin D deficient due to several months without proper sunlight exposure.
When it comes to nasal sprays, neti pots, or mouthwashes there really is no downside if used properly. Even if many of these remedies prove to be ineffective, there’s still plenty of reasons to deploy such remedies. Neti pots can help reduce congestion when ill, and mouthwashes may help to reduce the odds of getting gingivitis and provide a fresh breath.
Repurposed drugs such as Hydroxychloroquine and Fluvoxamine have been given an unearned bad rep. We still have yet to see widespread use of PAXLOVID and Molnupiravir, although the safety profile of these drugs are still in question. The idea that repurposed drugs, and even supplements and at-home remedies should not even be attempted should alarm people about the lack of any guidelines or actual proactive approaches by the NIH or CDC.
A doctor’s ability to practice as a doctor has been severely hindered. It should be up to medical professionals, as well as the patient/doctor relationship to provide the type of care that is best for the patient without interference by agencies who can’t even be bothered to address the lack of any viable therapeutics, and would instead turn to wishful thinking that those who get ill don’t become severely ill and require hospitalization. It’s a strange paradox, where we are told to live a life of fear because of this virus and yet doctors are told to not try anything until it’s too late. Either the virus is deadly and we throw whatever we can at it, or the virus is nothing to fear and we move on with our lives. The idea that the CDC and FDA can find it a viable option to deploy both is both nonsensical but also antithetical to rational policy-making.
Omicron has greatly changed the landscape of COVID, and yet the policies and approaches are still just as antiquated as ever. Now that everyone is likely to get Omicron, it’s time to learn how to deal with the virus in a way that benefits the patients more than it does the bureaucrats.
Citations
Koczula, K. M., & Gallotta, A. (2016). Lateral flow assays. Essays in biochemistry, 60(1), 111–120. https://doi.org/10.1042/EBC20150012
Kramer, A., Eggers, M., Hübner, N. O., Walger, P., Steinmann, E., & Exner, M. (2021). Virucidal gargling and virucidal nasal spray. GMS hygiene and infection control, 16, Doc02. https://doi.org/10.3205/dgkh000373
Guenezan J, Garcia M, Strasters D, et al. Povidone Iodine Mouthwash, Gargle, and Nasal Spray to Reduce Nasopharyngeal Viral Load in Patients With COVID-19: A Randomized Clinical Trial. JAMA Otolaryngol Head Neck Surg. 2021;147(4):400–401. doi:10.1001/jamaoto.2020.5490
Baxter, A. L. et al. Rapid initiation of nasal saline irrigation to reduce severity in high-risk COVID+ outpatients: A randomized clinical trial compared to a national dataset observational arm. medRxiv Available at: https://www.medrxiv.org/content/10.1101/2021.08.16.21262044v3.full .
Mohamed, N. A. et al. Early viral clearance among COVID-19 patients when gargling with povidone-iodine and essential oils – a clinical trial. medRxiv Available at: https://www.medrxiv.org/content/10.1101/2020.09.07.20180448v1.full#T2.
Diniz do Nascimento, L., Moraes, A., Costa, K., Pereira Galúcio, J. M., Taube, P. S., Costa, C., Neves Cruz, J., de Aguiar Andrade, E. H., & Faria, L. (2020). Bioactive Natural Compounds and Antioxidant Activity of Essential Oils from Spice Plants: New Findings and Potential Applications. Biomolecules, 10(7), 988. https://doi.org/10.3390/biom10070988
Meister, T. L., Todt, D., Brüggemann, Y., Steinmann, J., Banava, S., Brill, F., Steinmann, J., Pfaender, S., & Steinmann, E. (2021). Virucidal activity of nasal sprays against severe acute respiratory syndrome coronavirus-2. The Journal of hospital infection, 120, 9–13. Advance online publication. https://doi.org/10.1016/j.jhin.2021.10.019
Elkin, S. R., Lakoduk, A. M., & Schmid, S. L. (2016). Endocytic pathways and endosomal trafficking: a primer. Wiener medizinische Wochenschrift (1946), 166(7-8), 196–204. https://doi.org/10.1007/s10354-016-0432-7
Derendorf H. (2020). Excessive lysosomal ion-trapping of hydroxychloroquine and azithromycin. International journal of antimicrobial agents, 55(6), 106007. https://doi.org/10.1016/j.ijantimicag.2020.106007
Al-Bari M. (2017). Targeting endosomal acidification by chloroquine analogs as a promising strategy for the treatment of emerging viral diseases. Pharmacology research & perspectives, 5(1), e00293. https://doi.org/10.1002/prp2.293
Sukhatme, V. P., Reiersen, A. M., Vayttaden, S. J., & Sukhatme, V. V. (2021). Fluvoxamine: A Review of Its Mechanism of Action and Its Role in COVID-19. Frontiers in pharmacology, 12, 652688. https://doi.org/10.3389/fphar.2021.652688
Reis, G., Dos Santos Moreira-Silva, E. A., Silva, D., Thabane, L., Milagres, A. C., Ferreira, T. S., Dos Santos, C., de Souza Campos, V. H., Nogueira, A., de Almeida, A., Callegari, E. D., de Figueiredo Neto, A. D., Savassi, L., Simplicio, M., Ribeiro, L. B., Oliveira, R., Harari, O., Forrest, J. I., Ruton, H., Sprague, S., … TOGETHER investigators (2022). Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial. The Lancet. Global health, 10(1), e42–e51. https://doi.org/10.1016/S2214-109X(21)00448-4
Thank you for this wealth of information! Lord knows our public health authorities are not forthcoming with any useful information. I have used several of these methods after a recent exposure incident (mouthwash & neti-pot). Do remember to read the instructions for the neti-pot and use the appropriate type of water or you can actually cause more harm than good.
I had COVID about a year ago and in hindsight I would say it was actually a good experience for me. I'm not much of a stickler for the public health recommendations. I spent most of April - June 2020 gardening & raising chicken (outside, digging in dirt - all great for the immune system). I also avoid hand sanitizer like the plague and would never describe myself as a germ-o-phobe. Unless you suffer from SCIDs the excessive sterilization we inflict on ourselves really isn't good for your immune system. Back to my COVID experience - I went to another state (TN - my goodness, they aren't super crazy with the mandates down there) for the holidays (even though it was greatly discouraged) and low and behold we came home with the coof. It was a bit chaotic to say the least, BUT I did get to spend time with my dad (who was likely the source of our infection - turns out several of his care-givers had it - like basically everyone had it down there) who passed away a few weeks later. If I hadn't of gone I wouldn't of seen him just before he died and I am grateful for that opportunity. We weren't given the opportunity to see my father-in-law before he died in April 2020 as he was locked away in a nursing home. That is my source of shame. We blindly followed public health protocols and he died from loneliness/abandonment (he was there because my mother-in-law could not care for him as he required). We should have taken him out and cared for him ourselves - if I would have known I wasn't going to be back to work full-time until July we probably would have done that. It's ironic that COVID has nothing to do with his death, yet our response to COVID had everything to do with his death.
Nobody should ever feel shame for coming down with a respiratory sickness. We all gotta breath air! For those trusting the public health authorities (vaccines, boosters, social & familial distancing & N95 masks) I am sure they could feel shame as they thought they were doing all the right things and still got sick.
The only ones who should be feeling shame are those who inflicted so much emotional and psychological damage on children, young adults, people who have lost their jobs, people who are deathly afraid to see family members... Yet, they seem to have no shame whatsoever. This farce has gone on long enough. When it is over ... they need to be held accountable for all this collateral damage.
Thank you for the great information! I am recovering from Covid that I got twice in 5 months and this time I didn’t tell anyone and neither did my mom who got it from me. So the part you mention about shame is so true and I haven’t heard anyone else bring that up. I was embarrassed when I got it the first time and was frustrated and embarrassed the second time. I have not had the vaccine so I was hoping that my natural immunity would have protected me from getting it again and so quickly at that. As you said, everyone is going to get it and we need to just accept it and deal with it just as we do colds and flu and move on from this madness. Thanks for the great article!