


Case Review: Are Proton-Pump Inhibitors Dangerous?
An examination of the literature.

Note: Figures, Footnotes, and References have been removed to fit the email size. Please refer to the site for those additions.
For a large part of my (relatively) young life I’ve had issues with stomach irregularities. The more than occasional gassiness or the rumbling of an upset stomach was probably happening more than should be considered normal. A few years ago I discussed this issue with my primary care physician (PCP). She diagnosed me with gastroesophageal reflux disease, or GERD, and prescribed me with Ranitidine (brand name Zantac) and a large list of foods I should avoid- I’m pretty sure the only thing I would be able to consume would be water1.
Stomach issues plague many Americans including GERD, diarrhea, gastroenteritis, and other stomach-related issues. One drug that has been prescribed by the millions to help alleviate such stomach woes is proton-pump inhibitors (PPI). However, recent concerns have emerged about the widespread use of these drugs and whether they are as safe as they appear to be. Here, we will dive into some of the literature and see if these concerns are founded.
Brief History of PPIs
Proton-pump inhibitors are a class of drugs2 intended to treat stomach issues by reducing the production of gastric acid. The most commonly prescribed PPI is Omeprazole (brand name Prilosec), although several other PPI inhibitors have made their way to the market. They can either be prescribed or available over-the-counter.
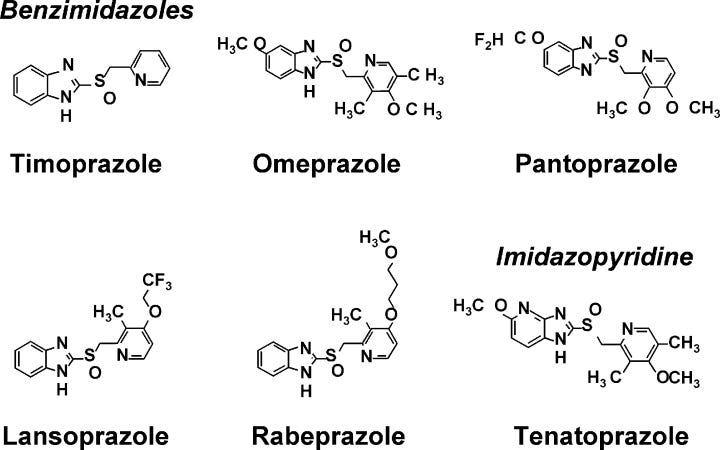
PPIs are a relatively new class of drugs. Prior treatment for stomach issues involved the use of calcium carbonate tablets or histamine2-receptor antagonists (of which Zantac is one such drug). However, the emergence of PPIs in the late 1980s and their greater clinical effectiveness compared to H2R antagonists has led them to surpass H2R antagonists in prescription and usage (taken from Strand et. al.3):
Since the introduction of omeprazole in 1989, proton pump inhibitors (PPIs) have steadily become the mainstay in treatment of acid-related disorders. When compared with earlier agents such as histamine2-receptor antagonists (H2RAs), synthetic prostaglandin analogs, and anticholinergics, PPIs have demonstrated consistent patient tolerance, excellent safety, and generally superior acid suppressing capability than prior agents.1,2
As of 2015, there are six PPIs approved by the United States Food and Drug Administration (FDA) (Table 1).3 Adoption of PPI use has been widespread among primary care providers, and their presence is ubiquitous within the armamentarium of the modern gastroenterologist. For most, this class of drugs represents the first choice for treatment of esophagitis, nonerosive reflux disease (NERD), peptic ulcer disease (PUD), prevention of nonsteroidal anti-inflammatory drugs (NSAID) associated ulcers, Zollinger-Ellison syndrome (ZES), and functional dyspepsia.4–6 In combination with antibiotics, PPIs are also an integral part of eradication therapy for Helicobacter pylori.7
Mechanism of Action/ Pharmacodynamics
PPIs have a rather exciting mechanism of action. PPIs inhibit H+/K+ ATPase transporters, which uses energy in the form of ATP to push hydronium ions (H3O+) across a concentration gradient4 into the lumen of the stomach. Thus, by inhibiting these transporters acid does not move into the stomach and symptoms are hopefully alleviated.

Inhibition of these transporters first starts with absorption of PPIs within the small intestine. Afterwards, the drug must then make it to parietal cells5 within the stomach, which are where the proton transporters are located.
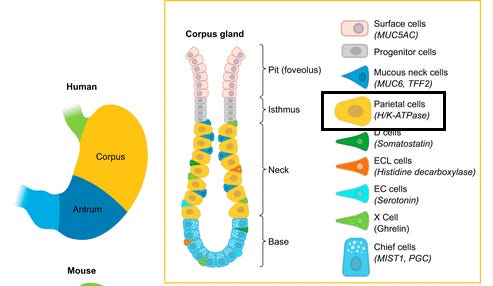
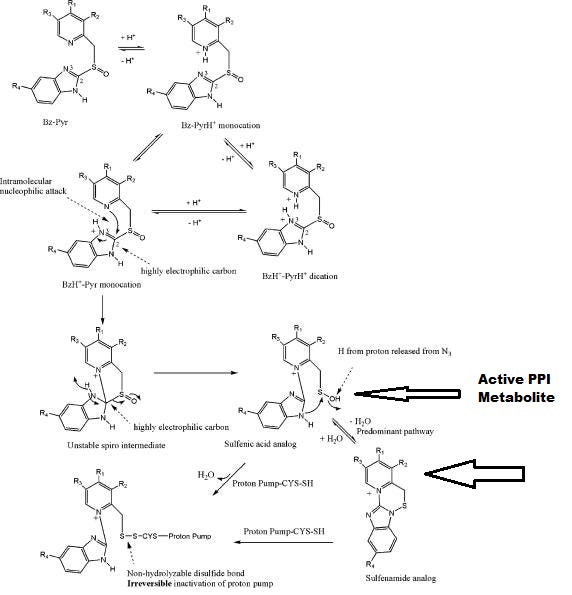
The secretory caniculi of parietal cells are extremely acidic (pH ~1) and when PPIs enter into this region of the cell they become protonated, eventually leading to a cascade of intramolecular reactions (reactions with itself). The main product of these reactions, a sulfenic acid/sulfenamide analog, serves as the active PPI metabolite that inhibits the proton transporter. The sulfenic acid analog can bind to cysteine amino acid residues of the proton transporter, forming a disulfide bridge and covalently inhibiting the transporter. This covalent bonding makes PPIs irreversible inhibitors and is the reason for their high effectiveness6.
Pharmacokinetics
PPIs require an acidic environment in order for the molecule to become activated and the intramolecular reaction to occur. However, this means that gastric acids are just as likely to lead to this reaction and quickly inactivate the drug. To avoid this, PPIs are covered in an enteric coating that prevents them from being targeted by gastric juices until they can reach the small intestines where they can become absorbed by the body.
The typical half life of PPIs are around 1 hour, but because they irreversibly bind to proton transporters the inactivation can occur for up to 48 hours7 and thus their effects are long lived after administration. Oral bioavailability of PPIs are relatively high, although they may suffer from the first-pass effect and be metabolized by the liver before they can elicit their effects. Omeprazole suffers from low bioavailability.
Cytochrome P450 enzymes serve as the main source of PPI metabolism. The most active isozymes are CYP2C19 and 3A4. Phenotypic expression8 of these isozymes alter the metabolism of PPIs. For example, people of East Asian ancestry such as Chinese, Japanese, and Korean people have lower phenotypic expression of these isozymes and thus are more sensitive to PPIs. People who have higher expression of these isozymes are likely to not notice an effect because of higher drug metabolism, highlighting the importance of examining genotypic variance when prescribing medications in order to provide an individual-based regimen.

Overuse and Over Prescribed
With such a cheap, relatively safe profile and ease of accessibility PPIs have become one of the go-to methods for treating stomach-related conditions. Paired with the consequences of modern living and we can easily see chronic, overly excessive use of PPIs becoming a common occurrence.
This has raised concerns that PPIs are being over prescribed (Safer, D.9):
PPIs are approved by the Food and Drug Administration (FDA) for 10 days for the treatment of Helicobacter pylori, up to 2 weeks for “heartburn”, up to 8 weeks for GERD and for 2 - 6 months for ulcers [18, 19]. Nonetheless, in a community survey, 60% remained on PPIs for over a year and 31% remained on them for 3 or more years [20][...]
In practice, these drugs are most commonly prescribed by primary care physicians and for the treatment of indigestion [24]. Over 60% of patients taking PPIs do not have a licensed/labeled indication for taking this medication or a documented GI diagnosis [24].
But there are also concerns that clinical settings may be abusing PPIs as well.
Take this excerpt from a 2008 BMJ article (Forgacs, I. & Loganayagam, A.10):
Although it might be assumed that overprescribing occurs mainly in primary care, evidence of inappropriate use of proton pump inhibitors in secondary care is abundant. In hospital inpatients taking proton pump inhibitors in Australia,3 Ireland,4 and the UK,5 63%, 33%, and 67% of patients did not meet their country’s criteria for taking the drug. In a series of hospital inpatients in Michigan, USA, 20% of patients were taking a proton pump inhibitor on admission and another 40% were prescribed the drug during their hospital stay (mostly for prophylaxis). At discharge, half the patients were taking a proton pump inhibitor—more than double the number who were taking the drug when admitted.6 In this study, 90% of patients did not need to take these drugs unless having gastro-oesophageal reflux at some time in the past is accepted as a reasonable indication.
In many cases hospital use of PPIs were predominately based on prophylactic usage and tended to not have another appropriate indication of use (Heidelbaugh et. al.11):
From an inpatient perspective, appropriate initiation of PPI treatment would be limited to primary conditions requiring directed therapy [such as undifferentiated upper gastrointestinal (GI) bleed, duodenal or gastric ulcer, or erosive esophagitis] or a select population of intensive care unit (ICU) patients requiring prophylaxis. Inappropriate PPI use in the ICU and on general care floors remains extensive, however, leading to significant yet controllable cost expenditure both in the hospital setting and after discharge [Heidelbaugh and Inadomi, 2006].
So it appears that the relatively cheap, easily accessible nature of PPIs may actually be detrimental. Because they are relatively safe doctors may consider it to be easy to prescribe without having a proper diagnosis- in their minds they may not see any harm in doing such a thing. However, if patients believe that their symptoms will be alleviated by PPIs, even though there may not be evidence to substantiate this position, they may continue to use them long-term under these supposedly false pretenses. There are also questions as to whether the symptoms a patient is experiencing is related to excessive stomach acid, once again raising questions about proper use of PPIs. Remember that the safety profile of drugs are relative to their use, and it seems that the excessive use of PPIs may contribute to several adverse reactions.
Adverse Reactions/Side Effects

Several people have commented that they have tried PPIs but with limited success, only to later find out that there were some concerns with PPI usage. There have been growing concerns over the past few years about dangerous side effects, and of course this has led to drug lawsuits popping up including some you may have seen on daytime television.
At a time where more people are becoming critical of the medical establishment we can see why this may create renewed interest on such a commonly used drug. But are the concerns warranted, or could they be overblown?
The acidic environment of the stomach plays a critical role in maintaining and protection our body’s various functions. Not only is it one of the first sites of digestion and absorption, stomach acids also help break down pathogens that are passed from our airways and upper respiratory tract and collect within our mucus. Certain vitamins and minerals may also require a highly acidic environment to become bioavailable and absorbed into our intestines. When stomach acid production is greatly reduced, the reduced acidity of the stomach may no longer be able to fulfill these functions and thus may contribute to several maladies. This effect is called hypochloridia (low stomach acid- literally low hydrochloric acid) and is likely responsible for all of the issues experienced with long-term PPI use.
Enteric Disease and Altered Microbiome
As previously stated, reduced stomach acid may prevent the proper breakdown of ingested material including bacteria. This may allow bacteria to take hold within the intestines and cause disease known as enteric disease leading to upset stomach, bloat, and diarrhea. Epidemiological evidence now suggests a possible correlation between long-term hypochlorhydric agents and enteric infections, most notably of C. difficile.
Additional information is provided from this review by Strand et. al.:
Further, there is evidence that PPI use may enhance patient susceptibility to a multitude of enteric infections including small intestinal bacterial overgrowth,92 Salmonella, Campylobacter jejuni, and Clostridium difficile.93 Infection with C. difficile (CDI) is of particular importance given the associated morbidity and escalating health burden posed by this problem. In 2012, a meta-analysis of 42 observational studies which included over 313,000 patients found that PPI use was associated with both incident (OR, 1.7) and recurrent (OR, 2.5) CDI.94 This observation led the U.S. FDA to issue a drug safety communication regarding the importance of PPI exposure, though the impact of both dose and duration of PPI treatment on this association remains unclear.
Unfortunately, most of this evidence comes from retrospective studies12, so no clear evidence is available. However, the amount of retrospective studies indicating PPI use with CDI and other enteric infections can be considered rather alarming.
The reduced acidic environment of the stomach does not just affect possibly pathogenic bacteria, but it also changes the microbiome by selecting for certain bacteria that would otherwise be degraded by stomach enzymes. Therefore, it is possible that an altered microbiome provides for a more hospitable environment for enteric infections.
Two pivotal studies were conducted to examine the microbiome of long-term PPI patients. In one study conducted by Jackson et. al.13 researchers looked at the gut microbiome of 1800 elderly twins who have previously taken PPIs. The results of these studies showed a reduced level of gut flora diversity in those taking PPIs as well as an increase in specific taxa of bacteria. What’s interesting is that the researchers noted the presence of pharyngeal bacteria within the gut, again suggesting that bacteria were not being properly eliminated within the stomach.
Similar results were found in another study by Inhamm et. al.14 in which PPI users had altered microbiome and had the presence of oral bacteria within the gut as well. Overall, these results suggest a strong link between PPI use, hypochloridia, and altered gut flora.
Rebound Acid Hypersecretion
Patients who abruptly stop using PPIs may notice a time frame in which gastritis and other gastroesophageal symptoms come back possibly even worse than before. Evidence suggests that the acid levels of these people are above their pre-PPI levels, suggesting a possible rebound effect. This effect usually occurs a few days after abruptly ending PPI use and may persist for weeks. In RCTs with healthy patients provided PPIs there was a noticeable rebound effect. However, the rebound effect seen in those with GI symptoms could not be separated from the original GI symptoms and so the extent of the rebound effect remains slightly controversial. Therefore, it’s hard to discern the true effect of rebound for those experiencing GI symptoms pre-PPI, although patients who may experience such a rebound may be more inclined to continuously use PPIs.
Reduced Vitamin and Mineral Absorption
There have been suspicions that the absorption of calcium, iron, and magnesium may be affected by PPIs and therefore may contribute to other maladies such as bone fractures and heart disease. However, the evidence appears to be inconsistent. In some circumstances meta-analyses suggest a possible relationship but heterogeneity, weak associations, and conflicting results confound the data. As it appears there is not enough evidence to suggest a possible link, although further studies may provide more concrete evidence.
The vitamin B12 requires acid-based release from proteins in order to become available. Reduced acidity of the stomach may prevent the proper release of B12 and possibly reduce absorption. However, the results here are conflicting as well.
Overall, the evidence is weak in relating PPI use to reduced vitamin and mineral absorption. The FDA released a label revision for PPIs to include the possibilities of fractures, but later corrected this labeling to indicate very low risk in short term, OTC use.
Kidney Disease / Heart Disease
The unique activation of PPIs allows it to select for parietal cells. However, other acidic environments may end up activating PPIs as well. Some of these targets are lysosomes, and PPIs may exhibit lysosomotropism similar to that of Fluvoxamine and Hydroxychloroquine. Some of these lysosomes reside in other organs including the kidneys and heart. This hypothesis suggests that PPIs may play a role in kidney and heart disease.
Although the available information is not robust, the available evidence does suggest a link between long-term PPI use and chronic kidney disease (taken from Jaynes, M. & Kumar, A.):
Shortly after the introduction of PPIs, case reports suggesting an association between their use and the development of acute interstitial nephritis (AIN) emerged.35 This association has been substantiated by further studies, but it is only in the last decade that the potential relationship between PPIs and the development or progression of CKD has been examined. The first large-scale study published examining the relationship between PPI use and CKD included two individual patient cohorts intended to represent the general population. In each group both the adjusted and unadjusted analysis found a significant positive relationship between PPI use and the development of CKD. Interestingly, H2RA use was not found to be associated with CKD in either cohort.32 The results of a similarly designed study by Xie and colleagues paralleled those of the Lazarus study. They found that PPI use was associated with a higher incidence of CKD, kidney disease progression and end-stage renal disease (ESRD).35 They also found that increased duration of exposure was associated with an increased risk of adverse renal outcomes up to 720 days of exposure; after 720 days, this association disappeared. A subsequent large, Swedish cohort study also found an association between cumulative PPI use and CKD progression.36 The most recent evaluation of PPI exposure and CKD by Li and colleagues using complex pharmacoepidemiologic tools to estimate the effect of unmeasured/unknown confounders on the relationship of PPI use and risk of CKD suggests that confounding factors alone were unlikely to explain the reported association.
For a small subset of patients there may be concerns of kidney disease in the form of acute interstitial nephritis. However, these patients may also be taking several medication and suffer from other concurrent diseases, which should be taken into account. Nonetheless, this raises questions as to the extent of kidney disease with long-term PPI use.
As for heart disease, the evidence is quite muddy. Some studies have suggested an increase in cardiac events with PPI use, although the evidence here is confounded. For one, some PPI patients may be on a Clopidogrel/Aspirin prophylactic regimen to prevent cardiac ischaemic events. PPIs are known to reduce the effectiveness of clopidogrel, and thus the effects of PPIs on cardiac disease may be tangential and not a directly related. Clopidogrel is an antiplatelet drug that requires activation by the same isozyme that metabolizes PPIs. The use of PPIs is therefore hypothesized to compete with Clopidogrel and thus reduces its antiplatelet capabilities. The FDA eventually included a warning label indicating that use of specific PPIs may reduce the effectiveness of Clopidogrel. As it stands, the effects of PPIs on heart disease is conflicted and affected by confounding variables.
Cancer Risk
Instances of gastric cancer have been in decline the past few years, notably due to greater levels of medical intervention and reduced rates of H. Pylori infection, a bacterial infection related to peptic ulcers and stomach cancer. However, there are concerns that gastric cancer may be attributed to PPI use. Hypochloridia may lead to an increase in the production of the hormone gastrin. This increase in gastrin is called hypergastrinemia and may cause downstream harm by altering gastric mucosa. Hyperastrinemia is also indicated in H. Pylori infections. Since PPIs are prescribed in those with H. Pylori infections there are questions as to whether PPIs are the causative agent in gastric cancer or if the damage from H. Pylori is the causative agent. Again, the concerns over cancer may be confounded by the presence of a pathogen. Therefore, further studies should be conducted to disassociate PPIs and H. Pylori in regards to gastric cancer. As for now, the evidence is concerning although not fully elucidated yet aside from correlative data.
Not Enough Evidence, but Real World Concerns
PPIs are available in nearly every market and are relatively cheap and easy to administer. In a modern world where stomach problems are likely to ravage millions of Americans and people worldwide there are concerns that PPIs may be used as a cheap way of alleviating these issues, leading them to be overused and for far longer than is recommended. Concerns have been increasing in the past few years that long-term PPI use may be associated with several side effects.
The FDA recommends no more than a 14 day course of OTC PPI use up to 3 times a year. However, the accessibility of these drugs may lead people to use them for much longer periods of time. Prescription PPIs may be provided for chronic use which raises question as to time-related increase in adverse reactions.
In general, the evidence is conflicting and confounded by many variables in regards to adverse reactions. The clearest evidence suggests that long-term use may alter the gut flora and there may some concerns about chronic kidney disease. It’s important to keep in mind that many of these studies are either observational or retrospective. Observational studies are important in understanding when an unwanted signal emerges, although further studies should be done to further analyze that signal. For now, the overall limited data does not provide enough concrete evidence in regards to heart disease, cancer, or nutrient deficiency.
But regardless, many of these studies were conducted in long-term users of PPIs, which raises question as to whether these side effects would be a concern if PPIs were not prescribed for so long. In many instances PPIs may be used for management of symptoms and not be used to treat the disease directly. If the disease is properly treated there may be no need for pharmaceutical interventions to treat symptoms. For example, obesity is considered one of the leading risk factors for GERD15. If there are concerns about long-term use of PPIs, it may be in the best interest of patients to look the cause of these GI issue and address them directly.
It’s a consequence of the times when it is far easier to prescribe a drug and deal with the symptoms rather than trying to fix the actual problems. This is a lesson many have learned when it comes to COVID, but it’s a lesson that should span all forms of medicine. It’s always better to prevent and treat the disease rather than to deal with just the symptoms alone.
Citations, References, and Additional Studies
Some of the articles here have been referenced above, but some are additional as well. For review studies keep in mind that many are looking at similar studies and may provide the same information.
General Review
SACHS, G., SHIN, J.M. and HOWDEN, C. (2006), Review article: the clinical pharmacology of proton pump inhibitors. Alimentary Pharmacology & Therapeutics, 23: 2-8. https://doi.org/10.1111/j.1365-2036.2006.02943.x
LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Omeprazole. [Updated 2019 Apr 15]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548771/
Strand, D. S., Kim, D., & Peura, D. A. (2017). 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut and liver, 11(1), 27–37. https://doi.org/10.5009/gnl15502
Shin, J. M., & Sachs, G. (2008). Pharmacology of proton pump inhibitors. Current gastroenterology reports, 10(6), 528–534. https://doi.org/10.1007/s11894-008-0098-4
Mechanism of Action
Roche V. F. (2006). The chemically elegant proton pump inhibitors. American journal of pharmaceutical education, 70(5), 101. https://doi.org/10.5688/aj7005101
Overprescription
Forgacs, I., & Loganayagam, A. (2008). Overprescribing proton pump inhibitors. BMJ (Clinical research ed.), 336(7634), 2–3. https://doi.org/10.1136/bmj.39406.449456.BE
Heidelbaugh, J. J., Kim, A. H., Chang, R., & Walker, P. C. (2012). Overutilization of proton-pump inhibitors: what the clinician needs to know. Therapeutic advances in gastroenterology, 5(4), 219–232. https://doi.org/10.1177/1756283X12437358
Safer D. J. (2019). Overprescribed Medications for US Adults: Four Major Examples. Journal of clinical medicine research, 11(9), 617–622. https://doi.org/10.14740/jocmr3906
Muheim, L., Signorell, A., Markun, S., Chmiel, C., Neuner-Jehle, S., Blozik, E., Ursprung, P., Rosemann, T., & Senn, O. (2021). Potentially inappropriate proton-pump inhibitor prescription in the general population: a claims-based retrospective time trend analysis. Therapeutic advances in gastroenterology, 14, 1756284821998928. https://doi.org/10.1177/1756284821998928
PPI use and Microbiome
Jackson, M. A., Goodrich, J. K., Maxan, M. E., Freedberg, D. E., Abrams, J. A., Poole, A. C., Sutter, J. L., Welter, D., Ley, R. E., Bell, J. T., Spector, T. D., & Steves, C. J. (2016). Proton pump inhibitors alter the composition of the gut microbiota. Gut, 65(5), 749–756. https://doi.org/10.1136/gutjnl-2015-310861
Reveles, K. R., Ryan, C. N., Chan, L., Cosimi, R. A., & Haynes, W. L. (2018). Proton pump inhibitor use associated with changes in gut microbiota composition. Gut, 67(7), 1369–1370. https://doi.org/10.1136/gutjnl-2017-315306
Imhann, F., Bonder, M. J., Vich Vila, A., Fu, J., Mujagic, Z., Vork, L., Tigchelaar, E. F., Jankipersadsing, S. A., Cenit, M. C., Harmsen, H. J., Dijkstra, G., Franke, L., Xavier, R. J., Jonkers, D., Wijmenga, C., Weersma, R. K., & Zhernakova, A. (2016). Proton pump inhibitors affect the gut microbiome. Gut, 65(5), 740–748. https://doi.org/10.1136/gutjnl-2015-310376
Side Effects/Adverse Reactions
Haastrup, P.F., Thompson, W., Søndergaard, J. and Jarbøl, D.E. (2018), Side Effects of Long-Term Proton Pump Inhibitor Use: A Review. Basic Clin Pharmacol Toxicol, 123: 114-121. https://doi.org/10.1111/bcpt.13023
Jaynes, M., & Kumar, A. B. (2018). The risks of long-term use of proton pump inhibitors: a critical review. Therapeutic advances in drug safety, 10, 2042098618809927. https://doi.org/10.1177/2042098618809927
Savarino, V., Dulbecco, P., & Savarino, E. (2016). Are proton pump inhibitors really so dangerous?. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver, 48(8), 851–859. https://doi.org/10.1016/j.dld.2016.05.018
Ariel, H., & Cooke, J. P. (2019). Cardiovascular Risk of Proton Pump Inhibitors. Methodist DeBakey cardiovascular journal, 15(3), 214–219. https://doi.org/10.14797/mdcj-15-3-214
Bavishi, C. and DuPont, H.L. (2011), Systematic review: the use of proton pump inhibitors and increased susceptibility to enteric infection. Alimentary Pharmacology & Therapeutics, 34: 1269-1281. https://doi.org/10.1111/j.1365-2036.2011.04874.x
Guedes, J., Aquino, J. A., Castro, T., Augusto de Morais, F., Baldoni, A. O., Belo, V. S., & Otoni, A. (2020). Omeprazole use and risk of chronic kidney disease evolution. PloS one, 15(3), e0229344. https://doi.org/10.1371/journal.pone.0229344
Paz, M., de Alencar, M., de Lima, R., Sobral, A., do Nascimento, G., Dos Reis, C. A., Coêlho, M., do Nascimento, M., Gomes Júnior, A. L., Machado, K., de Menezes, A., de Lima, R., de Oliveira Filho, J., Dias, A., Dos Reis, A. C., da Mata, A., Machado, S. A., Sousa, C., da Silva, F., Islam, M. T., … Melo Cavalcante, A. (2020). Pharmacological Effects and Toxicogenetic Impacts of Omeprazole: Genomic Instability and Cancer. Oxidative medicine and cellular longevity, 2020, 3457890. https://doi.org/10.1155/2020/3457890
Cheung, K. S., & Leung, W. K. (2019). Long-term use of proton-pump inhibitors and risk of gastric cancer: a review of the current evidence. Therapeutic advances in gastroenterology, 12, 1756284819834511. https://doi.org/10.1177/1756284819834511
I was essentially told that I could not eat fatty, spicy, sour/citrus, or fried foods and had to limit coffee intake. So pretty much everything was off the tables.
The important structures of PPIs are called pyridylmethylsulfinyl benzimidazoles.
Strand, D. S., Kim, D., & Peura, D. A. (2017). 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut and liver, 11(1), 27–37. https://doi.org/10.5009/gnl15502
This type of movement is considered active transport. To move a compound against a gradient is to move it in a direction it would favorably not move. Here, the high levels of acid within the stomach makes it difficult to add additional acid. Such a movement is not energetically favorable. In order to make this movement occur outside energy is needed to be put into the system. In this case, energy comes from ATP. The breakdown of ATP into ADP and phosphate provides the energy needed to move hydronium ions into the lumen and thus making the stomach more acidic.
People who would like to learn more about gastric parietal cells can find more information here: The Physiology of the Gastric Parietal Cell. Amy C. Engevik, Izumi Kaji, and James R. Goldenring Physiological Reviews 2020 100:2, 573-602
For those interested in the chemistry aspect of PPIs, I recommend this paper: Roche V. F. (2006). The chemically elegant proton pump inhibitors. American journal of pharmaceutical education, 70(5), 101. https://doi.org/10.5688/aj7005101
This long 48 hour period of inactivation is due to the time frame before more transporters are made by parietal cells.Safer D. J. (2019). Overprescribed Medications for US Adults: Four Major Examples. Journal of clinical medicine research, 11(9), 617–622. https://doi.org/10.14740/jocmr3906
Phenotypic expressions are the expressions of our genes, meaning that we can either visibly see them or can isolate the proteins involved in certain processes. Essentially, phenotypic expression is downstream of our genes.
Safer D. J. (2019). Overprescribed Medications for US Adults: Four Major Examples. Journal of clinical medicine research, 11(9), 617–622. https://doi.org/10.14740/jocmr3906
Forgacs, I., & Loganayagam, A. (2008). Overprescribing proton pump inhibitors. BMJ (Clinical research ed.), 336(7634), 2–3. https://doi.org/10.1136/bmj.39406.449456.BE
Heidelbaugh, J. J., Kim, A. H., Chang, R., & Walker, P. C. (2012). Overutilization of proton-pump inhibitors: what the clinician needs to know. Therapeutic advances in gastroenterology, 5(4), 219–232. https://doi.org/10.1177/1756283X12437358
A list of studies can be found by Jaynes, M. & Kumar, A.:
Jaynes, M., & Kumar, A. B. (2018). The risks of long-term use of proton pump inhibitors: a critical review. Therapeutic advances in drug safety, 10, 2042098618809927. https://doi.org/10.1177/2042098618809927
Jackson, M. A., Goodrich, J. K., Maxan, M. E., Freedberg, D. E., Abrams, J. A., Poole, A. C., Sutter, J. L., Welter, D., Ley, R. E., Bell, J. T., Spector, T. D., & Steves, C. J. (2016). Proton pump inhibitors alter the composition of the gut microbiota. Gut, 65(5), 749–756. https://doi.org/10.1136/gutjnl-2015-310861
Imhann, F., Bonder, M. J., Vich Vila, A., Fu, J., Mujagic, Z., Vork, L., Tigchelaar, E. F., Jankipersadsing, S. A., Cenit, M. C., Harmsen, H. J., Dijkstra, G., Franke, L., Xavier, R. J., Jonkers, D., Wijmenga, C., Weersma, R. K., & Zhernakova, A. (2016). Proton pump inhibitors affect the gut microbiome. Gut, 65(5), 740–748. https://doi.org/10.1136/gutjnl-2015-310376
Chang, P., & Friedenberg, F. (2014). Obesity and GERD. Gastroenterology clinics of North America, 43(1), 161–173. https://doi.org/10.1016/j.gtc.2013.11.009
A few years ago I went through that “foods to avoid” list with my husband and we were both left wondering what he could eat! Fortunately following a healthier diet & cutting out bread/grains helped rid him of his GERD without medication. Unfortunately these types of diets are hard to follow long term - there’s just so much yummy bad-for-you food!! We’re both working on moderation & eating less (Americans eat way TOO much food).
There always seems to be unintended consequences to these marvelous modern medicines and you have shown how important it is to understand what these medications do to our bodies. I have always thought it should be better to treat the root cause rather than the symptoms!
RN/VA: My peers and I have noted that 15 years ago or so almost all of our patients (psyche) were on omeprazole, then starting about 2 years ago almost no one was. We assumed it was because of the co-morbidities/side effects mentioned in your very thorough paper.