


A PAXLOVID/Molnupiravir Combination Therapy?
A recent macaque study and a possible explanation for viral rebound.

Additional Context: As pointed out by Paula in the comment section there appears to be one macaque within the vehicle group that fared well as noted in Figure 2D with the one grey point that appears negative at 4 dpi. However, this led me to look back at Figure 3C and notice that all but one macaque showed no infectious titers at 4 dpi. This finding would be strange given the fact that we would assume that the vehicle/control group would fare worse rather than better.
Now, this could be a consequence of sampling in which case the collection of saline may be inconsistent on each day, which may account for the appearance of rebound within the combination group. However, given the fact that all the other vehicles showed consistent decline in infectious titer this may raise questions as it may contradict persistent viral load within the lungs as being a factor for rebound. Keep this in mind.
Controversies surrounding PAXLOVID and Molnupiravir as being the only “approved” outpatient treatments for COVID has caused a lot of speculation to their actual effectiveness.
Rampant reports of viral rebound in regards to PAXLOVID certainly raise questions as to what factors could be causing these phenomena, especially as reports generally focused on the vaccination status of individuals provided PAXLOVID and experiencing rebound.
However, as I reported a while back one study appears to suggest that this isn’t a phenomenon specific to PAXLOVID but appears to be the case with Molnupiravir as well.

Considering that both drugs have different mechanisms of action it makes one wonder what exactly is going on.
However, the use of either PAXLOVID or Molnupiravir is a rather strange one, mostly for the fact that these drugs are being used as monotherapies i.e. alone—something that doesn’t happen often with other infections.
HIV infection generally uses a cocktail of drugs that target the virus at different points during the replication cycle.
Even for COVID the FLCCC uses a cocktail of drugs in both their outpatient and inpatient treatment, although many of these treatments include commonly found items and it is suggested that not all of these therapies may be necessary. Remdesivir as used within the hospital setting is also provided along with several other medications.
All of this made for a strange situation, and when PAXLOVID was first announced I made a few comments that a protease inhibitor drug being used alone likely hasn’t been done before.
In essence, the use of these monotherapy drugs may be considered unprecedented for the treatment of a virus and possibly could be the reason for the rebound being witnessed.
During the FDA hearing for Molnupiravir several of the committee members made comments that Molnupiravir, a nucleoside analogue that has mutagenic properties, should probably be used in concert with PAXLOVID, such that the combination of the two would mimic the cocktail treatment for HIV and may be more effective.
Research into combination therapy of these two drugs has generally been carried out in vitro or using ferret and mice models.
However, a few weeks ago a preprint was released from Rosenke, et. al.1 examining the use of both PAXLOVID and Molnupiravir within nonhuman primates— in this case in rhesus macaques— and seeing if the combination worked better at fighting COVID than the individual treatments.

Study Design
To study the effectiveness of a combination therapy rhesus macaques were divided into four groups:
One control group
One given only PAXLOVID (containing both Nirmatrelvir [PF-07321332] and Ritonavir)
One given only Molnupiravir (MK-4482)
One given both
Each group comprised of 5 monkeys. Although a rather low number, the use of 20 nonhuman primates may actually be considered quite large for a trial such as this.
The researchers also used Delta as the variant as they considered it to be the more lethal variant. Given that we are in the Omicron wave this study does have to be looked at in a different context due to the mismatch of variants as compared to our current wave of variants.
The details of the study design are as followed:
To assess the efficacy of the two treatments individually and in combination, rhesus macaques were randomly divided into vehicle- or MK-4482-, PF-07321332- or combination treatment groups (n=5 per group). Animals were infected with 2×106 TCID50 of SARS-CoV-2 Delta VOC by combined intranasal and intratracheal routes (1×106 TCID50 each route). Drug treatments began 12 hours post-infection (12hpi) with animals receiving either vehicle or 130mg/kg MK-4482 (260mg/kg/day) or 20mg/kg PF-073211332 + 6.5mg/kg ritonavir (40mg/kg/day, 13mg/kg/day) or a combination of all 3 compounds consisting of the same doses as for individual treatments. Treatments were administered by oral gavage every 12h (7 treatments in total). The study ended 4 days post-infection (dpi) (12h following last treatment), at which time animals were euthanized for tissue collection and analysis (Fig. 1A).
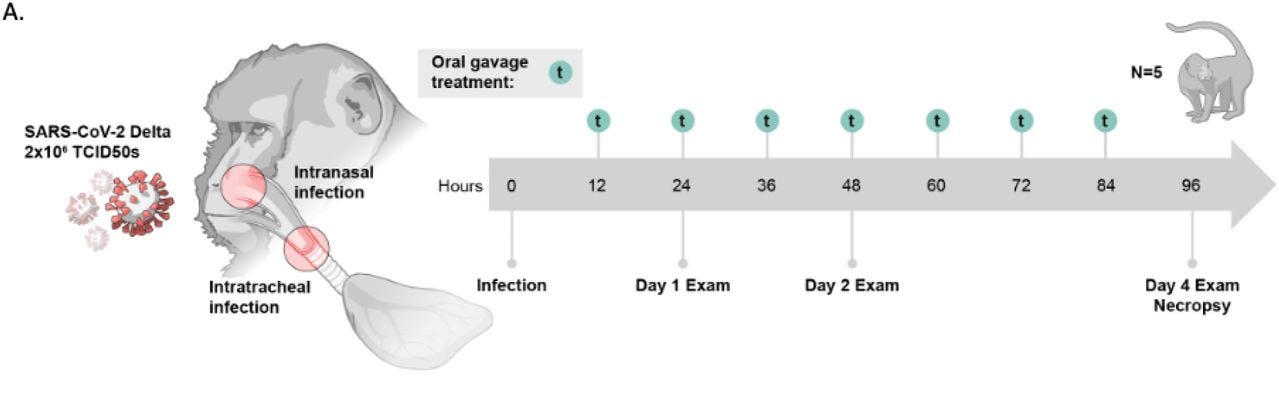
Remember that the “3 compounds” mentioned here includes Ritonavir the P450 inhibitor that is used in conjunction with Nirmatrelvir to increase the half life and serum concentration of Nirmatrelvir (PAXLOVID is the name for both of these drugs).
The dosing of these drugs also appear to be comparable the ones used during human clinical trials when size and mass are taken into account:
Dosing for the study was allometrically based on the clinical treatment schedules currently approved for use for COVID-19 treatment. Molnupiravir (MK-4482) is prescribed as an 800mg twice daily oral treatment (1600mg in total) within 5 days of symptom onset [31]. Similarly, nirmatrelvir is an oral treatment prescribed for twice daily oral treatment of 300mg (600mg total) with the addition of 100mg ritonavir (200mg/total) [32].
Results
When looking at these results remember that this is based on the results of the researchers with notes indicated where necessary.
1. Combination therapy appeared to show lower clinical scores indicating better improvement
First, infected macaques were measured based on clinical scores over the 4 days of the study, with a lower score being indicative of better outcomes and fewer symptoms2. In short, the control group had higher clinical scores and the combination therapy group had the lowest, although the researchers noted that differences in scores between groups was not statistically significant on any given day.
Animals in the vehicle treated group showed the highest scores throughout the experiment peaking at 2dpi. Animals in the group receiving the combination treatment scored the lowest throughout (Fig. 1B). Animals in the groups treated with either MK-4482 or PF-07321332 alone scored in between (Fig. 1B). Although differences between groups were not statistically significant on any single day of the study, AUC analysis showed a significant difference between the vehicle treated group and the group receiving the combination therapy (Fig 1C).

Remember that these scoring measures can be considered subjective, and in cases where the treatment group and control group are not properly blinded for the person conducting the scoring there is a possibility that biases may lead researchers to misinterpret signs of infection.
Put another way, if you know that the monkey you are seeing hasn’t been given therapeutics you may infer little behaviors as indications of severe infection while those given the combination may have their behaviors and symptoms underscored.
Keep that in mind when considering these scores.
2. Combination group had lower viral loads in and less viral replication within the upper respiratory tract
In order to examine viral load the researchers collected nasal and oral samples from macaques and conducted Subgenomic E (sgE)-based RT-PCR to measure SARS-COV2 viral replication.
Unlike regular genomic measures which may come from inactivated or “dead” viruses, subgenomic RNA comes from the transcription of structural protein genes before they are translated. This mechanism appears to be discontinuous leading to these fragments of RNA, which may give a better tell as to whether viral replication is occurring since they can only be produced during an infection.3
The “E” here refers to the envelope protein of SARS-COV2. Therefore, this PCR assay is measuring the presence of subgenomic E RNA within these samples.
Samples were collected 1, 2, and 4 dpi (days post-infection). Results suggest that all treatment groups showed reduced viral load. However, viral load was reduced the most among the combination group:
Compared to the vehicle treated group, sgE viral RNA loads in the nasal swabs were lower in all three treatment groups and remained significantly lower in the combination therapy group for the duration of the study. The PF-07321332, but not MK-4482, monotherapy treatment group was also significantly lower at 4dpi (Fig 2A). [...] At 1dpi, all treated animals had significantly lower infectious titers. By 2dpi, the differences between treated and untreated animals were further amplified and a larger subset of animals in each treatment group had no detectable infectious virus (Fig 2B). There were no significant differences in the levels of viral RNA detected in the oral swabs at any timepoint examined (Fig 2C), but AUC analysis performed for the entirety of the study did reveal a significant difference between the combination therapy and the vehicle control (Fig S1a). Infectious virus was significantly lower at 1dpi in all treated groups when compared to the vehicle control group, and treated groups remained significantly lower over the entirety of the study (Fig 1D).

It’s interesting that, compared to Molnupiravir, PAXLOVID appeared to perform better in viral clearance. It’s hard to determine why that may be the case. It may be a consequence of reduced bioavailability of Molnupiravir as well as some pharmacokinetic factors.
Probably more interesting is the discrepancy between the nasal samples and the oral samples as more of the macaques appear to have higher viral loads within their nasal region (comparing A/C and B/D above). It’s even interesting that 2 dpi the Molnupiravir group showed an elevated level of sgE RNA possibly indicating active replication.
Now, you may look at the above figures and wonder what the difference is between viral load as measured by sgE RNA and infectious titers. Although both are measures that correlate with replication-competent virus the association between the two may not itself be correlated to one another.4
Similar to regular RT-PCR sgE RNA measures may lead to false positives and may not provide a true reading of infectious virions. Therefore, although viral load may be high the actual level of infectious virions may be much lower or nonexistent (refer to the study from Footnote 3 and notes on the results from said study).
As interpreted by the researchers high viral load would be indicative of active replication while infectious titers may measure the ability for these monkeys to infect others. It’s rather confusing since both these measures can be synonymous but also may not be accurate comparisons.
Okay, I may be making this more confusing but understand that, for all intents and purposes, both measures appear to decrease over the course of 4 days and to a greater degree with the the combination therapy.
3. Lower respiratory tract results showed high viral load but low infectious titers
In order to examine the lower respiratory tract Bronchoalveolar lavages (BALs) were collected. This method takes saline and places it into a subsegment of the lung where it is then suctioned back up with the hope of collecting material from this region.
The researchers, after sacrificing the macaques, also removed six segments of lung tissue from each macaque (related to the total number of lobes) and examined them for viral load and infectious titer.
And it’s here where there may be a few methodological problems:
Tissue samples from each lung lobe were collected at 4dpi for viral load analysis. RNA was isolated from each sample for PCR analysis. Each lobe value was then pooled for total lung comparisons between groups.
This aspect alone normally wouldn’t be a big deal. However, given the fact that the nose, throat, upper airway, and lower airway are being examined and with the prior concerns of viral rebound leading to this combination study it would have been far more advantageous to have had the samples stratified and compared between macaques. At the point that all 6 tissue samples are taken for each macaque we are dealing with a total of 30 data points per treatment group with no way of discerning what sample came from which monkey.
Now, this creates a problem as we can’t associate lobe tissue with a specific macaque. We may see why this is a problem with the following Figure:

The results here contrast some of the results from the upper respiratory tract including far higher viral load and even indications infectious virions still persisting by Day 4.
The results shown for the lower respiratory tract are interesting given the fact that several macaques from each treatment group appear to still have relatively high viral load and infectious titer:
By 4dpi all groups had a single animal with detectable levels of infectious virus with all other animals being negative (Fig 3B).
There also doesn’t appear to be any “statistically significant” results for this study:
As shown in Fig 3A, sgE RNA loads were lower in PF-07321332 and combination therapy groups at 1dpi and 2dpi, compared to the vehicle controls. The differences were more pronounced between groups at 2dpi but at no time was the sgE significantly different between groups (Fig 3A).
It’s also interesting that at 2 dpi all of the combination macaques didn’t appear to have infectious titers but by day 4 there appears to be some type of recrudescence (rebound).
Altogether, these results are interesting in that they actually may elucidate the mechanisms of rebound, such that viral persistence may occur in a subset of patients due to persistent, infectious viral load within the lungs and lower respiratory tract that aren’t properly cleared due to the drug.
An explanation may be provided by the researchers. The last thing they examined were concentrations of either drugs or metabolites in both sera and the lungs of these macaques.
Interestingly, drug concentrations were lower in the lungs compared to sera:
As plasma was collected prior to dosing at each exam point, levels of each therapeutic molecule in the plasma reflect the lowest circulating concentrations over the treatment course. At each time point, levels of all 3 drugs were readily detectable, with a mean of 46.47nm for EIDD-1931 [the active metabolite of Molnupiravir] and 12.75nm for PF-07321332 in plasma. Drug concentrations were lower in lung tissue with a mean of 21.52nmol/g EIDD-1931 and 0.06nmol/g PF-07321332. Combination therapy increased these values in both plasma and lungs to 76.17nM EIDD-1931 and 19.21nM PF-07321332 in plasma and 23.84 nmol/g EIDD-1931 and 0.36 nmol/g PF-07321332 in the lungs. All values agree with the treatment scheme in both plasma and lung homogenate samples, with anticipated slight temporal fluctuations. Lung levels of EIDD-1931 were also in good agreement with previous data examining efficacy of MK-4482 in the Syrian golden hamster model [21].
The data here is rather limited, and there’s no information on the proper therapeutic dose for lung tissue to put it lightly, but given the fact that bioavailability of the drug in lung tissue appears to be lower in sera we may infer that reduced viral clearance may be due to lack of drug accessibility in the lungs, although more studies may would be needed to validate these results (and in some ways this was already assumed due to the anecdotal events of rebound anyways).
Is a combination therapy better?
In talks of rebound one comment that has been brought up is that the treatment duration of 5 days may have been too short with some researchers suggesting a longer dosage period would be necessary.
Although the current study suggests that combination therapy was very effective in reducing viral load and eliminating infectious virions the results of the lower respiratory tract suggest that the virus may persist in a few select macaques up to the 4 day mark. The researchers were also selective in their wording, usually not referring to the fact that combination wasn’t better than individual treatments alone, but compared to the control group5:
As shown here, individual treatment with both compounds resulted in significantly reduced SARS-CoV-2 viral load in the upper and lower respiratory tract significantly reducing SARS-CoV-2 shedding and replication, and ultimately led to less severe respiratory disease compared to vehicle treated animals.
So it’s hard to say whether a combination therapy would be better if the argument is that time and dosing may be the actual reason for recrudescence. Granted, the dosing argument would come with the caveat that dual therapies may overcome that low dose barrier.
There’s also the fact that clinical trials for both PAXLOVID and Molnupiravir used a 5 day cutoff limit (enrolled within 5 days of symptom onset or positive PCR). The results for these macaque studies, especially Fig. 2C, suggest that even with treatment started 12 hours post infection led to high viral invasion within the lungs.
The researchers noted that indications of pneumonia or lung pathology were lower in treated macaques (not shown here), but given that the presentation of COVID within these macaques were relatively mild it’s hard to associate the lung tissue staining results with severe COVID.
As such, even mild infection may lead to severe viral invasion of the lungs.
Given this fact, it could be that later treatment of the disease with either PAXLOVID, Molnupiravir, or both (including other treatments) may allow for deep viral invasion of the lungs. Low bioavailability of treatment drugs within the lungs as noted in this study may indicate that viral clearance may be suboptimal and allow for the persistence and resurgence of virions, which may then spread to the upper airways and lead to positive PCR tests days after a negative test and the presentation of viral rebound.
We have to keep in mind that the verification of rebound among non-PAXLOVID groups is rather limited due to the fact that, for the most part, many people may not be undergoing constant PCR testing and therefore lack of continuous monitoring of individuals using other treatments may miss other rebound scenarios.
In any case, the research here provides some insights into the viral persistence within the lungs as being a possible factor for rebound. This isn’t a unique hypothesis as many people have considered this to be the case when first reports of recrudescence came to light.
Further research may provide better insights, and even possible clinical trials that extend the duration or increase the dosing of treatment may provide better evidence towards the phenomenon of rebound.
However, given the fact that Molnupiravir’s mutagenic properties have never been extensively researched there should be concerns about the safety of this drug. For the most part, the uncertainties of these new drugs paired with the uncertainties of viral rebound makes for a complicated scenario.
If you enjoyed this post and other works please consider supporting me through a paid Substack subscription or through my Ko-fi. Any bit helps, and it encourages independent creators and journalists outside the mainstream.

Rosenke, Kyle & Lewis, Matthew & Feldmann, Friederike & Bohrnsen, Eric & Schwarz, Benjamin & Okumura, Atsushi & Bohler, W. & Callison, Julie & Shaia, Carl & Bosio, Catharine & Lovaglio, Jamie & Saturday, Greg & Jarvis, Michael & Feldmann, Heinz. (2022). Combined Molnupiravir and Nirmatrelvir Treatment Improves the Inhibitory Effect on SARS-CoV-2 in Rhesus Macaques. 10.1101/2022.09.03.506479.
The researchers list a few of these scoring criteria below:
Animals were scored for signs of disease daily by the same person blinded to the study groups using a previously established scoring sheet [19]. A score (0–15) was assigned for each of the following: general appearance, skin and fur, nose/mouth/eyes/head, respiration, feces and urine, food intake, and locomotor activity. All scoring was performed prior to anesthesia for treatments and examinations. Groups scored evenly in the morning prior to inoculation (0dpi).
Dagotto, G., Mercado, N. B., Martinez, D. R., Hou, Y. J., Nkolola, J. P., Carnahan, R. H., Crowe, J. E., Jr, Baric, R. S., & Barouch, D. H. (2021). Comparison of Subgenomic and Total RNA in SARS-CoV-2 Challenged Rhesus Macaques. Journal of virology, 95(8), e02370-20. Advance online publication. https://doi.org/10.1128/JVI.02370-20
As noted in this review by Bruce, et. al. many assays that had low Ct values when testing for sgE RNA did not find isolatable viruses and may be an indication of a false positive. The researchers gave two hypotheses:
While we were initially surprised by the number of samples with viral RNA detectable by Mills‐sgE and Wölfel‐sgE that lacked isolatable virus, and by our observation of sgRNA outside of cells, there are several potential explanations for this. First, RNA could be released into the supernatant by infected cells undergoing apoptosis. Second, given that sgE:E in the supernatants remain relatively constant (including at time points before cell death), it is also possible that SARS‐CoV‐2 sgRNA is packaged into virions and actively released.
Further testing by these researchers led them to assume the latter hypothesis i.e. that sgRNA may be packaged within virions may be the reason for these results.
Bruce, E. A., Mills, M. G., Sampoleo, R., Perchetti, G. A., Huang, M. L., Despres, H. W., Schmidt, M. M., Roychoudhury, P., Shirley, D. J., Jerome, K. R., Greninger, A. L., & Botten, J. W. (2022). Predicting infectivity: comparing four PCR-based assays to detect culturable SARS-CoV-2 in clinical samples. EMBO molecular medicine, 14(2), e15290. https://doi.org/10.15252/emmm.202115290
The researchers do make this note:
Compared to individual drug treatments, combined therapy resulted in increased efficacy with decreased SARS-CoV-2 shedding and replication early post infection and milder disease as compared to monotherapy.
Although that isn’t quite substantiated by their own research as all throughout they indicate that there was no statistically significant difference between the groups on any given day.
I found it interesting that at least one of the controls (gray dots) did just as well as anyone in the treatment groups. What was special about that one that enabled him to clear the virus on his own? As an unvaxxed person who had omicron in April and wasn’t very sick (and will never vax my kids) I think research into why some people/monkeys do fine on our own is essential.