


The Curious Emergence of Omicron
Part III: Loss of Neutralizing Antibodies

Natural Immunity and Two-Dose Vaccine Regimens show Reduced/No Protection Against Omicron (With Respect to Antibodies)
The targeting of vaccines and therapeutics against SARS-COV2’s spike protein provides a double-edged sword. Here, the administration of antibodies or therapeutics that can properly bind to the spike protein, in particular the receptor binding domain, are able to neutralize the virus’ ability to attach to host ACEII receptors and gain entryway into host cells.
But the virus’ dependency upon the spike protein also makes it the most malleable antigen, as constant mutations provide both greater odds of increasing receptor binding as well as providing a chance for antibody escape.
Omicron contains several dozen mutations within its spike protein, and so it makes sense why great attention is being paid towards these mutations’ effects on antibodies. Last week I posted about monoclonal antibodies losing effectiveness against Omicron. Many of these monoclonal antibodies (aside from Sotrovimab) were sourced from prior SARS-COV2 patients from the initial strain of the virus and the earliest variants. Because of this, I argued that loss of effectiveness in monoclonal antibody treatments should parallel a similar loss in effectiveness with respect to both natural immunity and the original vaccine dose regimen.
And it appears that this is what is happening; in nearly all of the studies I have looked at so far natural immunity and the original 2 dose vaccine regimen showed greatly reduced neutralization of Omicron.
Referring to the Zeng et. al. study once more, researchers collected blood sera from healthcare workers who received 2 doses of the mRNA vaccines (d & h). Sera was also collected from people who received boosters (e), were previously infected with Delta (g) or were admitted to either the hospital or ICU prior to the availability of vaccines (f). All across the board- aside from the boosters and those infected with Delta- the evidence suggests that sera antibody neutralization was greatly reduced against Omicron:
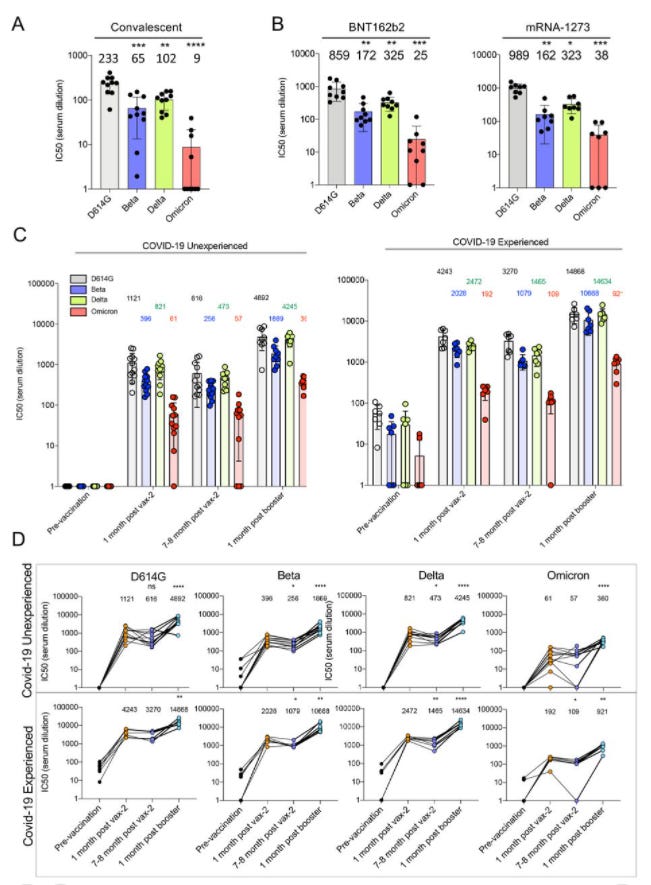
We next examined the ability of Omicron to escape vaccine-induced neutralizing antibodies, a critical measure of protection from SARS-CoV-2 infection16. To address this, we collected sera from 48 health care workers (HCWs) 3–4 weeks post-second dose of either Moderna mRNA-1273 (n = 20) or Pfizer/BioNTech BNT162b2 (n = 28). Having previously examined this cohort for the ability of the D614G, Alpha, Beta, and Delta variants to escape serum antibody neutralization (nAb)17, we compared the neutralization resistance of Omicron to these variants of concern. We found that the Omicron variant exhibited significantly more neutralization resistance, i.e., 22.9-fold (p < 0.001), compared to ancestral D614G, with the Alpha, Beta, and Delta variants exhibiting a 1.2-fold, 4.4-fold (p < 0.001), and 2.0-fold (p < 0.01) decrease in nAb titers, respectively (Fig. 1d). In total, only 27.1% (13/48) of HCWs exhibited nAb titers against Omicron above the detection limit (NT50 < 80); however, several individuals (1–3) exhibited strong nAb titers that were maintained against Omicron (Fig. 1d and andh).h). Moderna mRNA-1273 in HCWs slightly outperformed Pfizer/BioNTech BNT162b2 (Fig. S1a), as we have reported previously17,18.

There’s a few interesting takeaways from these results. The two-dose vaccines were based on the original strain of the virus, and so a comparison can be made between those who were vaccinated and those who were infected with Delta- essentially a comparison of how different variant “vaccinations” affect the antibodies produced. Here, the antibodies produced by the two-dose mRNA vaccine regimen showed a strong reduction in neutralization capabilities against Omicron while showing strong activity against the initially circulating strains (D614G), Alpha, and Gamma. Sera collected from patients previously infected with Delta seemed to show broad neutralization activity against all variants, although both Beta and Omicron showed lowered neutralization titers compared to the other 3 strains. In fact, the similar pattern can be seen with both the 2-dose regimen as well as hospitalized patients (ICU/hospitalized patients are expected to produce more antibodies, as there is evidence that more severe illness produces a greater immune response which can be seen when comparing the antibody response in the ICU patients).
Comparisons can be drawn based on these results. It raises questions as to the dichotomous antibody response, with 3 strains of the virus showing similar neutralization activity while both Beta and Omicron seem to be outliers. It would be interesting to see comparative analysis conducted between Beta and Omicron’s mutations and why they produced such a different immune response compared to the other variants, especially considering that Beta contains far fewer mutations compared to Omicron.
It is worth reiterating that these assays were done with antibodies, and don’t take into account the response by previously exposed B or T cells. The response by antibodies are not the only thing that should be taken into account, yet unfortunately many researchers tend to focus solely on antibody assays and not immune cell responses.
In my post last week I focused solely on assays that were targeted towards monoclonal antibodies. However, several of these studies also examined both natural immunity and the different vaccine regimens and saw similar results.
Here’s one from Wilhelm et. al. It’s a figure I have referenced twice already in prior posts, but I’ll provide a little more clarity to the important details:
To evaluate the protective capacity, antibody-mediated neutralization efficacy against authentic SARS-CoV-2 Omicron was determined in vitro using an isolate obtained from a double mRNA-1273-vaccinated travel returnee from Zimbabwe and compared to Delta. Neutralization performed with sera from double or triple BNT162b2-vaccinated individuals (6, 0.5 or 3 months after last vaccination/booster) revealed an 11.4-, 37.0- and 24.5-fold reduction, respectively (Figure 1A). Sera from double mRNA-1273-vaccinated and additionally BNT162b2-vaccinated individuals (sampled 6 or 0.5 months after last vaccination/booster) showed a 20- and 22.7-fold reduction in the neutralization capacity (Figure 1B). Poor neutralization against Delta and no efficacy against Omicron were observed using sera from heterologous ChAdOx1/BNT162b2-vaccinated individuals (Figure 1C). Additionally, the group receiving a third BNT162b2-vaccination showed a significant increase of NAb titers but a 27.1-fold reduction in neutralization against Omicron (Figure 1C). Neutralization of Omicron was 32.8-fold reduced using sera from double BNT162b2-vaccinated and previously SARS-CoV-2-infected individuals (Figure 1A).

In the Tada et. al. study cited in my monoclonal antibody series, a decrease in Omicron neutralization was also found, although not to the same levels as the prior studies cited.
Attention should be brought to the high variability in immune response towards Omicron. It appears that the antibodies produced by several patients did not produce any neutralizing capabilities (data points on the bottom seen in both the Wilhelm et. al. and Tada et. al. graphs). Although speculative, it’s likely that the antibodies produced by these patients did not target regions of the spike protein that remained conserved across the variants (think of “Sotrovimab” and how it targets conserved regions of the spike protein). If the antibodies only targeted regions which have mutated, it makes sense that no robust response was created against Omicron.
Several factors should be examined as to why such a response would occur, including confounding variables such as age and obesity status, which play critical roles in a patient’s immune response, and are likely to alter the antibodies a patient produces.
As expected, a booster regimen appears to confer the greatest antibody activity against Omicron in both those who were triple vaccinated as well as in those previously infected then vaccinated. Attention should be brought to the heterologous immune response (infected then vaccinated), as these patients overall exhibited stronger antibody activity than just the 3-dose patients.
There’s a few reasons why this would be occurring, but like I mentioned above think of Sotrovimab when examining these results. The strength of Sotrovimab is derived from its ability to target a region of the spike protein that remains conserved in both SARS-COV and SARS-COV2. It’s been well-established by now that antibodies that do not target regions undergoing constant mutations is the best way to garner consistent neutralizing activity against all variants.
What could be happening in the 3-dose and infected/vaccinated cohorts is that constant exposure to the spike protein could be eliciting a more varied immune response over time, eventually leading to the production of antibodies that are likely to target regions of the spike protein that prior exposure failed to target.
Think of a redundant activity (such as cleaning or even activities like puzzles), where you go through the motions and cover the bases of what needs to get done. It’s the same routine over and over again, but over time you may notice little things that you either missed or ignored (a corner of the house you never bothered to dust), and discovering this not only do you engage in whatever activity is needed, but are reminded to do so in the future as well.
There’s a lot of immunology responsible for this activity, such as rapid mutation of immune cells to produce highly varied antibodies which battle over who will become the “best” antibodies, but the point is that repeated exposure to the antigen finds the little bits that were missed during prior infections or vaccinations. If these new parts of the spike protein are conserved between the prior strains and Omicron, you are likely to produce neutralizing, cross-reactive antibodies that are likely to hold up against other variants.
In the case of what’s called heterologous exposure, in which the route of antigen presentation or vaccination is different (such as infection/mRNA vaccine or adenovirus/mRNA vaccine), the greater production of neutralizing antibodies is likely tied to that difference in antigen presentation, as people who have been previously infected would have been exposed to the entire virus and then exposed to just the S1 subunit when vaccinated with the mRNA vaccines. Also, the use of lipid nanoparticles, which are known to be adjuvants (elicit an immune response), would also produce a different immune response compared to just natural infection alone.
This raises a few questions in regards to the booster policies being implemented. Considering that those who were previously infected and then forced to receive COVID vaccinations due to mandates, these people are likely to have the most robust immune response, including against Omicron and relative to triple vaccinated individuals. As we are beginning to push towards mandating boosters, questions need to be brought up over the efficacy and legitimacy of such erroneous policies.
Overall, there’s a good reason for there to be concerns over vaccines and natural immunity playing any role against Omicron. On just the basis of assays utilizing antibodies against pseudotype viruses (viruses made to present with only the spike protein of SARS-COV2), we can see that Omicron showed a great level of reduced neutralization activity. However, the point must be made that these studies did not use actual SARS-COV2 viral particles, let alone Omicron variants. Even more important, the phylogenetic tree studies I included previously also highlight the importance of researchers to detail what mutations their version of Omicron contains, as differences in spike mutations are going to alter antibody binding.
The use of antibodies as a measure of immune function has been highly controversial. Our immune systems do not operate off of just the ability to produce antibodies, but is dependent upon the entirety of the immune response, including maturation and differentiation of B and T cells to best target pathogens as infections arise, yet most assays done of this nature do not take into account the activity of immune cells, and thus we are left ignorant of a pivotal part of our immune system.
But not all hope is lost. Fortunately, some researchers took to examining the response to Omicron by T-cells, and the results are very promising.
For a basic breakdown of T-cells, here is a reference from ASU, but here’s a more jargon heavy overview from Jarjour et. al. for those interested:
T cells are important regulators of cellular and antibody-mediated (humoral) immunity. Conventional T cells, distinguished by the expression of the cell-surface receptors CD4 and CD8, use clonally variable T cell receptors (TCRs) to recognize antigens derived from pathogen proteins in the form of peptide fragments associated with major histocompatibility complex (MHC) molecules (human leukocyte antigen [HLA] in people). This leads to T cell differentiation into a range of effector cell types tailored to control the invading organism (Table 1 ). Different types of pathogens require distinct immune effector cell types to be controlled. In the case of viral infections, these usually include “follicular helper” CD4+ T (Tfh) cells that induce B cells to produce high-affinity antibodies capable of neutralizing the pathogen and cytolytic CD8+ T cells that kill pathogen-infected cells. Clonal diversity in the pre-immune “naive” T cell population means rare cells will be present with TCRs able to recognize a new pathogen, such as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). In a productive immune response, these specific T cell populations undergo dramatic numerical increases and differentiate to manifest appropriate effector functions for elimination of the pathogen. This is usually followed by a substantial loss of effector cells but preservation of an elevated number of durable “memory” T cells of various types, also termed subsets (Table 1), which can be efficiently deployed if an individual is reinfected by the same pathogen (Figure 1 A). Since effective immune memory can persist for decades and typically results in enhanced responses and accelerated pathogen control, generation of robust and durable T and B cell memory is a goal of vaccines, including the many vaccines against SARS-CoV-2 that are currently in human trials.
In a preprint by De Marco et. al., researchers collected blood from volunteers who had only been vaccinated or had heterologous exposure through either a DNA/mRNA vaccine regimen or infection/vaccination. Then, researchers isolated their lymphocytes and challenged them against Omicron’s spike protein. Although a reduced response was seen against regions of the spike protein with high levels of mutation, the response to the entire protein appears to have held up.

This is an important study, as it takes into consideration more than just the activities of antibodies, but the cells that are responsible for signaling and producing the antibody response. As is suggested by these studies, a T-cell response to Omicron should still hold old up, indicating a quicker immune response to Omicron and should, ideally, lead to a quicker defense response.
Compared to the Wuhan strain, the Omicron variant carries over 35 mutations in the Spike protein. The impact of these mutations on antibody recognition has been shown to be substantial, with a significant loss of neutralizing activity in serum from both convalescent and vaccinated individuals 2,11. In previous variants, although antibody neutralizing potency was decreased, T cell responses were maintained 4,12, although some mutations have been shown to affect CD8 T cell recognition 13. Here, we find that T cell responses against the mutated regions in Omicron are strongly affected. However, as these regions cover only a small fraction of the whole protein the overall response against Omicron Spike appears to be largely preserved. Reactivity to the variant was similar regardless of vaccination and/or infection history. The finding of persisting and robust T cell responses despite the mutations in Omicron thus provide confidence that the cellular immunity against this variant will not be compromised.
Unfortunately, the researchers only used spike proteins in this study aside from whole viral particles, which may indicate a different response to the whole virus, especially considering the nature of immune escape elicited by whole viral particles.
This study outlines something critical to the COVID conversation, and it’s something many people have discussed yet seems to be missing in health policies. Antibodies are not the only thing that should matter; it’s the totality of the immune response, something we will clearly miss if we just collect and examine the binding of antibodies to antigens. This is also something that Dr. Malone brought up in his discussion with Joe Rogan about why immune cell response isn’t being taken into consideration.
From the perspective of researchers, it could be that neutralization assays are far easier to perform, as antibodies may be easier to isolate than T-cells, and may not require the same stringent storage requirements. That still doesn’t make up for the near abundance of COVID literature on antibodies over T-cell responses, and this situation is made even worse when antibody levels are what’s being used to drive vaccination policies.
It also doesn’t make sense that waning antibodies are being used to measure a decline in immune response. Even if antibody production for these COVID vaccines are shorter lived (compared to other vaccines), the T-cells should continue to remain. In fact, that’s the intent of the adaptive immune system. The creation of long-lived immunity that elicits a quicker response to a learned antigen is what drives the survivability of our species. Remember that, when not constantly exposed to an antigen, it makes no sense for the body to continuously produce antibodies. Our bodies try to behave in a less wasteful manner, and what’s more wasteful than constantly producing antibodies against an antigen you are no longer being exposed to? It’s both wasted resources and energy that could be better utilized by other biological processes. So it’s not about the antibodies, but the cells that produce the antibodies and their ability to quickly mount a response to future exposures to antigens that matters, and the idea that this isn’t being carefully analyzed should call into question the health policies that are being forced onto us.
We can see why many of the concerns over Omicron are warranted. So far, it seems that both the original vaccine regimen and natural infection do not provide strong neutralization against Omicron. However, a 3rd vaccine dose, possibly due to constant antigen exposure, likely produced antibodies that target conserved spike protein regions which confer greater neutralization activity against Omicron.
However, there’s also clear evidence that those who have had prior infections and two doses of the mRNA vaccines show comparable antibody titers to triple vaccinated individuals. Een without vaccination, people previously infected with Delta contain neutralizing antibodies against Omicron, something else that should be taken into consideration in the COVID discourse. With a greater push for booster mandates, health officials should understand that vaccines are not the only route to reaching herd immunity- even I remember a time when natural immunity was considered a part of herd immunity. We should become very concerned when, even at this point, natural immunity in all of its forms are not being taken into consideration when it comes to these mandates.
Even in the face of Omicron, public policy doesn’t seem to be able to keep up with the science.
Part IV will look into a shift in Omicron’s target cells, possibly altering its infection dynamics and indicating its reduction in severity and virulence.