


Remdesivir: COVID's Standard of Care that May be Causing more Harm than Good (REVIEW)
Part V: When you blame everything but the drug.

I think we have covered a lot in regards to Remdesivir and toxicity. However, reports on Remdesivir and its possible toxicity have not been as transparent.
In fact, it seems that any reporting revolves around obfuscating any evidence against Remdesivir.
I’m not quite sure why the media feels the need to defend a drug, especially since so many journalists can’t even be bothered to do a bit of research on the topics that they cover.
Usually these arguments that sidestep the evidence against Remdesivir seem to come in two forms; either the carrier molecule is the problem or its due to COVID itself. We’ve seen these factors appear in the literature multiple times so we know that these are things that have been looked into.
However, we will need to dive further and see the problems with how Remdesivir is presented, and how any concerning side effects may be swept under the rug.
Blaming it on the Carrier Agent
We’ll spend most of our time discussing a compound that is used along with Remdesivir during its administration.
Now, I mentioned at the beginning of the series that prodrug groups are added to nucleosides in order to increase their hydrophobicity, increase cell permeability, and reduce their odds of being metabolized by enzymes.
However, there is a drawback to this formulation if the attempt to resolve one problem may lead to others.
In general, drug design is based on the acronym ADME (Absorption, Distribution, Metabolism, Excretion). The most important two for our scenario are the first two- absorption and distribution.
The way a drug is transported changes how it is administered and how available the drug is to reach their destination.
When it comes to Remdesivir it seems that the prodrug group that is added made Remdesivir too hydrophobic, to the extend it has reduced solubility in water. More specifically, this means that Remdesivir would not be able to circulate within the body because it would not want to stay within the blood, if it would enter there at all.
In order to solve this problem Remdesivir is administered with a carrier agent which is a molecule that can “pull” Remdesivir into solution and help circulate it within the body.
The carrier molecule in question is called sulfobutylether-β-cyclodextrin, or SBECD for short.
It’s a long name but you can discern the structure by breaking it down.

As can be seen SBECD is a cyclic (cyclo) structure comprised of carbohydrate/sugar molecules (dextrin). The R-groups depicted on the structure above indicate that there may be several different groups that can be substituted in place of the “R”. For SBECD, the group can either be a hydrogen (-H) or it can be the 4-carbon chain (butyl) structure with the additional sulfite (sulfo) group. The bonds formed between a C-O-C group are also called an “ether” group. And finally, the beta refers to the bonds between each sugar molecule that comprise the ring structure. Taken altogether, this is how the structure got it’s name of sulfobutylether-β-cyclodextrin. This is an unnecessary tidbit, but just in case anyone was curious and wanted to know where the name came from.
The importance of this molecule is that it essentially acts as an emulsifier. This structure is water soluble and has great interactive affinity to Remdesivir. Therefore, SBECD is able to “pull” Remdesivir into solution by sitting in the middle of the molecule and entering into solution. Another name for these molecules is “surfactant”, which is a portmanteau of “surface acting agent”.
If all of this is still confusing, just remember that the behavior of SBECD and surfactants in general are how soaps (including dish and hand soap) as well as laundry detergents operate.
SBECD has been used for decades as a solubilizer. However, prior formulations of cyclodextrin have been known to have fairly serious side effects.
Here’s an excerpt form a review by Stella et. al, explaining a brief history and reasoning behind the formulation of SBECD:
“In the early 1980s the need for a new drug solubilizer for parenteral formulations became apparent. The way one solubilized intractable, poorly water-soluble drugs for parenteral use during this period was pH-adjustment for ionizable drugs and use of co-solvents or surfactants. However, reports by Dye and Watkins, 1980, Watkins, 1979, Hüttel et al., 1980 began to describe anaphylactoid like reactions, later also called Idiosyncratic Histamine Release, with the use of the popular surfactant Cremphor EL. Other surfactants were also implicated. These observations were critical as around 1984, a novel, breakthrough drug to treat breast and ovarian cancers, taxol, later known as paclitaxel, was in clinical studies in women at the National Cancer Institute. The clinical formulation used consisted of a taxol/paclitaxel concentrate of 50% each of Cremophor EL and ethanol. This concentrate was then diluted with Normal Saline (NS) prior to infusion to patients. In the mid-1980s a number of women receiving paclitaxel had severe reactions to this solvent, namely, the Cremophor EL component. As Rowinsky et al., (1993) later stated, “a high incidence of major hypersensitivity reactions due to the Cremophor EL vehicle used in formulation disrupted and almost terminated the clinical development of paclitaxel.””
And so SBECD was created in order to reduce possible side effects.
Although some animal models have suggested possible nephrotoxicity as well as hepatotoxicity (when provided at 2000 mg/kg doses), it doesn’t seem like this has transferred over into human trials and administration. This could be due to the very short half life of SBECD, which seems to hover around 1.5 hours.
Overall, it seems like SBECD is fairly safe, at least in humans.
Which brings us to this weird bit of information from Remdesivir’s fact sheet. We’ve already covered that Remdesivir may play a role in drug-induced toxicity, but it seems that instead the blame is being put onto SBECD.
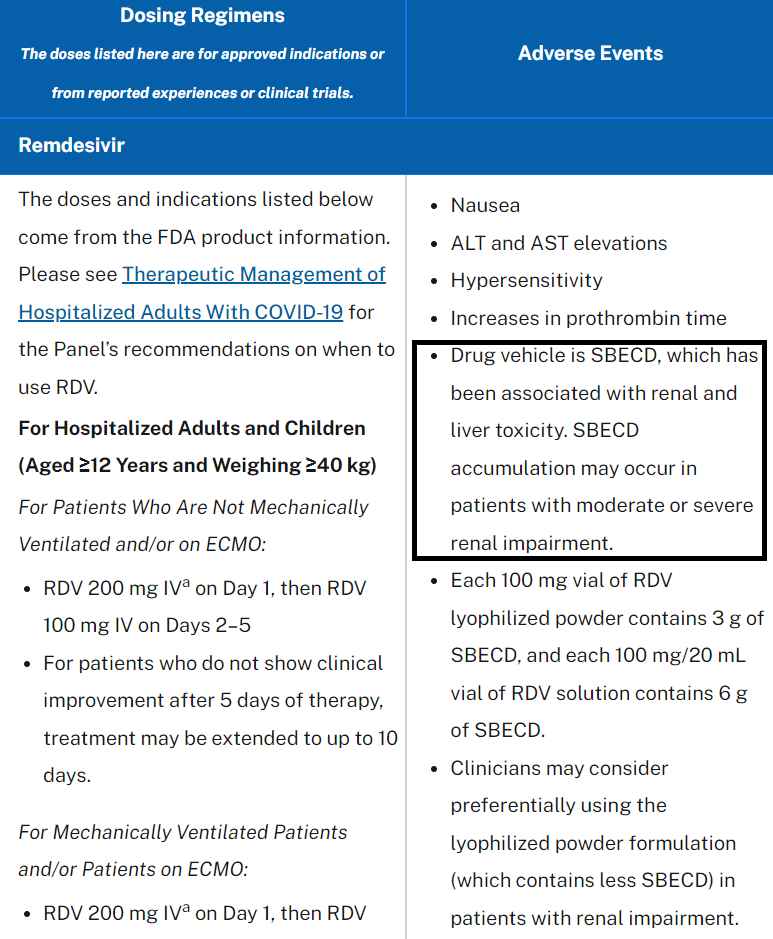
It’s interesting that part of this chart, which is taken from the NIH’s COVID-19 Treatment Guidelines website lists SBECD as being the possible toxic agent. Even more interesting, there isn’t any citation to studies to support this idea.
So we’re being told that Remdesivir may lead to elevations of liver enzymes, there may be some concerns about liver and kidney damage, but all of this is being attributed to SBECD and not Remdesivir.
Unlike the NIH, we’ll look at the evidence and see if any information supports this position.
SBECD is commonly used as a carrier agent for the compound voriconazole, which is an anti-fungal used in life-threatening fungal infections. Although rarely used, there should be some evidence of possible toxicity in this group, as the absence of Remdesivir may point to SBECD as a possible agent.
In a case study from Mach et. al, 4 patients with severe renal impairment were given voriconazole and SBECD. In all patients a large increase in SBECD was observed. One patient, a 75-year-old female had a reduced level of SBECD hours after administration and made a full recovery:
“A 75-year-old woman submitted with acute myeloid leukemia showed a maximal sulphobutylether beta cyclodextrin sodium plasma level of 145 μg/ml in the initial phase of treatment with intravenous voriconazole (Figure (Figure1,1, Table Table1,1, patient no. 1). After a few days renal function recovered and the plasma levels came down to less than 20 μg/ml after 10 days of treatment with intravenous voriconazole.”
However, 3 patients ended up with renal failure, and these 3 had the largest levels of SBECD:
“In contrast to the patient with a recovery of renal function the remaining three patients showed renal failure during the complete period of intravenous treatment with voriconazole. In these patients an accumulation of sulphobutylether beta cyclodextrin sodium plasma levels was determined with a maximum of 523 μg/ml in a 18-year-old man submitted with myocarditis (Table (Table1,1, patient no. 2), 409 μg/ml in a 57-year-old man submitted with multiple myeloma (Table (Table1,1, patient no. 3), and 581 μg/ml in a 47-year-old man submitted with intestinal ischemia (Table (Table1,1, patient no. 4).”
Although these cases look alarming, the researchers could not find evidence that renal failure occurred due SBECD. Considering that severe renal impairment was caused by the fungal infection, and that patients reached levels almost similar to the ones in animal models, the lack of clear evidence makes it hard to argue definitive proof against SBECD.
However, these results were also mirrored in another study where voriconazole was given to patients undergoing continuous renal replacement therapy (dialysis).
In a study by Kiser et. al. researchers looked at SBECD levels in 10 patients undergoing therapy due to a fungal infection.
In the context of this study the constant filtration efficiently removed SBECD, meaning that the direct action of SBECD on renal and hepatic function can’t be fully discerned. Nonetheless, the researchers suggested that they did not find any nephrotoxicity or hepatotoxicity associated with SBECD:
“Although our study was small, no evidence to suggest SBECD as a cause of hepatotoxicity or nephrotoxicity was demonstrated in our study patients. This finding is consistent with other SBECD safety studies in humans [3,18]. Additionally, animal studies have only been able to demonstrate cyclodextrin toxicities when dosages more than 50-fold greater (3,000 mg/kg) than those used in humans were administered [3,19,20]. Unlike other cyclodextrins used in these animal studies, SBECD undergoes only minimal tubular reabsorption and limits concentrations within the intracellular tissues of the kidney, potentially reducing the risk of nephrotoxicity. Nevertheless, the FDA labeling for voriconazole recommends that IV therapy be avoided, if possible, in patients with a CrCl <50 ml/min [5]. Our data suggest that IV voriconazole can be safely administered in this population if the patient is concurrently undergoing CVVH.”
So we have to be careful with this study. Although it mentions no indications of toxicity from SBECD, the constant removal through filtration may have played a role.
Taken together though, there doesn’t seem to have been serious prior signals to raise concerns, although we can argue the evidence is a bit spotty as well.
In the realm of COVID the evidence here is a bit sparse.
As was listed in the FDA treatment guideline Remdesivir comes in two forms; either lyophilized (dried) or in serum form. The lyopholized form comes with half the amount of SBECD and is usually reserved for patients who may suffer from renal impairment.
With this information we can make the assumption that administration of Remdesivir in the lyophilized form would lead to less incidences of renal and hepatic injury as compared to patients who received the serum form.
A recent study by Shah et. al. wanted to answer this assumption. In this study, 1,000 hospitalized COVID patients were either provided Remdesivir in lyophilized form or in solution form.
As the researchers found, there was no statistically significant difference between the two groups, although they noted that there were slightly higher incidences of acute kidney injury in the group given the solution form:
“Despite these baseline differences, there were no statistically significant differences, but there were trends toward a lower incidence of AKI using peak serum creatinine (3.2% versus 4.5%, P = 0.218) and early discontinuation due to abnormal liver function tests (LFTs) (0.9% versus 2.3%, P = 0.09) in patients who received remdesivir lyophilized powder compared to those who received solution, respectively (Table 2)”... “However, use of the injectable solution formulation of remdesivir, older age, baseline hypertension, days of symptom onset to remdesivir administration, and a CrCl of <30 ml/min on the day of remdesivir administration were not significantly associated with peak Scr AKI.”
These results match the results in the prior studies in people who suffered from renal impairment. Remdesivir treatment did not seem to lead to AKI in those patients, although if they were suffering from kidney disease already they were more likely to have been provided the lyophilized form of Remdesivir.
So we’re stuck at an impasse here. The biggest issue is that none of Remdesivir’s formulations exclude SBECD, so any study that utilizes Remdesivir has no way of controlling for SBECD to a full extent. However, the prior evidence in antifungal treatment, and its use over several decades should be evident of a relatively safe carrier agent (similar to other off-label drugs we may have heard about).
The evidence isn’t there to fully rule out SBECD, but that doesn’t make sense as to why Remdesivir is not included as a possible toxic agent. If anything, both Remdesivir and SBECD should be considered to have possible toxic side effects, especially if there’s no way of delineating the effects between Remdesivir and SBECD.
So on one hand, we have no discernible effects for the drug in use, the evidence against the carrier agent is spotty, and yet the carrier agent is the compound to be concerned about and not the drug or both together.
In any incident we should expect to go off of the basis of the precautionary principle; if unsure of what may be a toxic agent, it may be best to assume both until evidence proves otherwise. But we’ve continuously seen this approach be used in a selective manner.
So I would not argue that SBECD itself is the agent that is causing kidney and liver damage, but it would be best to assume that both Remdesivir and SBECD may be of questionable safety, which calls into question why NIH’s guidelines have been written the way it has. In no way can the NIH argue that Remdesivir is safe while arguing that SBECD should be blamed for any adverse reactions.
Blame it on the COVID
I think we’ve covered this point extensively, but I think we should cover it in the context of media reporting and their version of the blame game.
Recently, reports began circulating from a chiropractor named Dr. Ardis who suggested that Remdesivir may be killing many people.
If anyone would like to hear his perspective, check out this segment. Remember that it’s not the entire video. (A longer, different video can be seen in this Rumble video. Remdesivir talk starts around the 8:45 mark):

I won’t attest to the veracity of his claims, although remember that the Ebola trial did not use a placebo group so it’s a study that examines relative effectiveness compared to standard of care (ZMapp). Remdesivir was also the only antiviral that was used in the study. Also, remember that Ebola is an extremely deadly disease. A lack of a placebo group means that we can’t discern how many people would have died without being provided treatment (when studies use standard of care as the control instead of placebo, it’s done due to ethics- it’s considered highly unethical to deprive people of any treatment option and so a standard is used as a control instead of a placebo).
Personally, I would claim that Dr. Ardis’ arguments are not fully contextualized and should be taken with some skepticism.
However, the response to Dr. Ardis’ claims are what seem to be the most concerning. Instead of arguing the merits of his claims the media instead decided to resort to typical talking points.
Take, for example, this piece in First Draft arguing against Dr. Ardis’ claims:
“A former US chiropractor’s false claim that the antiviral drug remdesivir is responsible for Covid-19 deaths has been viewed hundreds of thousands of times on various video platforms. Remdesivir is approved for use in the treatment of hospitalized Covid-19 patients around the world, including in the European Union, the United States and Australia. While there has been conflicting data about whether the drug is effective in preventing Covid-19 deaths, the latest research, such as this peer-reviewed study published in August, found treatment with remdesivir was associated with lower mortality compared to best supportive care.”
And the article ends with this comment:
“The Associated Press debunked Ardis’s false claims in this fact check report, citing expert opinions that the symptoms described would be associated with severe Covid-19 infection and not remdesivir. Falsehoods and conspiracy theories about possible treatment for Covid-19, including remdesivir, may have real-life consequences if online narratives discourage people from seeking medical care, as NBC’s Ben Collins reported.”
So the issue here is whether Dr. Ardis’ claims are false (note that he is referred as a chiropractor- one should consider this an attack on his position as an authority figure, although I would argue to examine his comments for merit rather than proof by authority). I would rather argue that it requires nuance, skepticism, and contextualization, but I think we’ve done a good job of outlining all of these already, as it seems that the biggest factor in Remdesivir’s toxicity may be the timing of the drug when someone may be likely to suffer from kidney and liver damage from the disease itself and would thus exacerbate the symptoms.
But we don’t get that here. Instead, we are told that these are “false claims” and yet are then told that the evidence is unclear although a recent study is cited.
This is a typical tactic that will be used by many in the media; randomly cite a study without putting it within the context of all other studies. One study does not override all of the prior evidence, but adds to the discourse. Also, look at how the one study is used to generalize to all of “the latest research”. Readers who are unable to discern this misdirection may fail to notice that they may need to find more than one study to argue that much of the recent literature is in favor of Remdesivir’s use.
Also, take a look at how the paper ends. The journalists indicated a “fact check” from “expert opinions”. Personally, I wouldn’t consider an opinion a fact. I mean, I’m pretty sure they are complete opposites, but I’m not a journalist so I unfortunately know better than to consider an opinion a fact, but that’s just me.
The issue here revolves around this Associated Press “fact check”, which I assume will be filled with plenty of evidence. Instead, it seems to just be based on opinion (but remember, it’s expert opinion!):

Notice how this claim is laid out and how it’s done so intentionally. No one is claiming, at least from what I have seen, that Remdesivir’s toxicity is leading to “lungs filling with fluid”. This is obviously a symptom of COVID, and so its inclusion (especially as the first symptom) is done to intentionally throw off the claims of dissenters and make them seem absurd. The main argument has been made around possible kidney and liver damage NOT the lungs or pneumonia!
We can also see that with the “assessment”. The inclusion of the “fluid in the lungs” phrase is combined with the “renal failure” to argue overall that this is caused by the disease and not the drug.
Unfortunately, the AP “fact check” doesn’t cite any actual studies. It mentions a study that showed Remdesivir reduced recover times which is like the NIH’s “final report” study, and I’ve pointed out the issues with that study already.
But look at how the AP approaches this study. Did they decide to examine the study themselves? No, they went to an “expert”, Dr. John Mellors, to describe to them what the results of the study are. Note, I didn’t put “expert” in quotation marks to argue Dr. Mellors is not an expert, but to argue that media outlets will use the term “expert” as a form of validation instead of making any sort of substantive argument.
There is another expert who is mentioned, Dr. Hana El Sahly, who seems to have helped conduct a study with Remdesivir. Now, conduct is a broad term- let’s assume that her helping would mean that her name should appear on a study. One of the only studies I could find was this study which did not compare Remdesivir to a placebo or standard of care, but compared Remdesivir’s use with an anti-inflammatory called Baricitinib.
Based on this, it would be hard to argue that this would be suggestive of Remdesivir’s safety profile even if it is considered to be more effective relative to Remdesivir alone.
But here’s something even more sneaky that is occurring. Both “experts” used by the AP made mention to kidney failure and nothing directly about lung fluid buildup. Dr. Sahly mentions lung side effects and mentioned that [these] side effects did not occur in her study. It’s very broad, generalized terms that don’t add any merit to the claims being made. If we are going to argue about fluid filling lungs, why not bring up evidence against the argument that Remdesivir does not, in fact, lead to fluid buildup. It’s a pretty easy argument to make, but it seems like the argument being made by the AP’s journalists is to resort to vacuous, inane remarks that add nothing to the discourse except to push a narrative in favor of Remdesivir.
And this is the most striking thing to have come about. Why not emphasize that the evidence isn’t fully there in favor or against Remdesivir’s safety and effectiveness?
This is an issue of fact-checks in general. It’s more about the claim and the empty rebuttal more than it is to make any substantive argument. Honestly, how many people would have made it past the bullet points I laid out above?
When there’s a Lack of Evidence but Certainty of Opinion
I’ll end this point reiterating this point again. The evidence in regards to Remdesivir’s safety profile is spotty. However, its use in late-stage disease should absolutely be questioned. Any side effects, which may be likely to occur, will be further exacerbated when other confounding variables are at play.
This is the same argument I made in regards to Hydroxychloroquine’s usage as well, so in that regard my perspective remains consistent.
But here’s the kicker; which one of these compounds has had their EUA removed, and which one is continued to be used improperly as a standard of care against COVID?
The evidence against SBECD or the disease itself are arguments I have made already, and even in this area we can see that the evidence is both sparse and muddy.
Taken altogether, there really is no clear and decisive evidence towards any safety profile. But instead of arguing in favor of that until more research comes out, why have the NIH, the FDA, and media outlets resorted to playing the blame game and blaming everything else BESIDES Remdesivir?
So fine, maybe they should argue that SBECD or COVID could play a causative role AS WELL AS REMDESIVIR, and should not be excluding Remdesivir in its entirety.
Hopefully, we will see more evidence, but for now remain skeptical and always look for evidence. And absolutely, under no circumstances, should you use the phrase “fact check” as a phrase that provides any form of merit or evidence.
Citations
Stella et. al, 2020. Sulfobutylether-β-cyclodextrin. Taken from https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7196545/
Mach et. al, 2006. Accumulation of the solvent vehicle sulphobutylether beta cyclodextrin sodium in critically ill patients treated with intravenous voriconazole under renal replacement therapy. Taken from https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC1592308/
Kiser et. al, 2015. Evaluation of sulfobutylether-β-cyclodextrin (SBECD) accumulation and voriconazole pharmacokinetics in critically ill patients undergoing continuous renal replacement therapy. Taken from https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC4338618/
Shah et. al, 2021. Renal and Hepatic Toxicity Analysis of Remdesivir Formulations: Does What Is on the Inside Really Count? Taken from https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8448111/#B6