


New Study Suggest Link Between mRNA Vaccines and Heart Damage
What does a recent abstract tell us about the relationship between the vaccines and heart inflammation markers?

Recently, an abstract highlighting a concerning relationship between the mRNA vaccines and heart damage/inflammation began circulating on Twitter. The recent abstract indicates that the researcher tested a group of people pre and post-vaccination and measured certain inflammation biomarkers using a PULS test.
If the results are accurate, it would indicate an alarming concern about the use of these vaccines. But before resorting to histrionics we should see what we can gather from the abstract and parse the information as best we can.
Here’s the abstract in full:
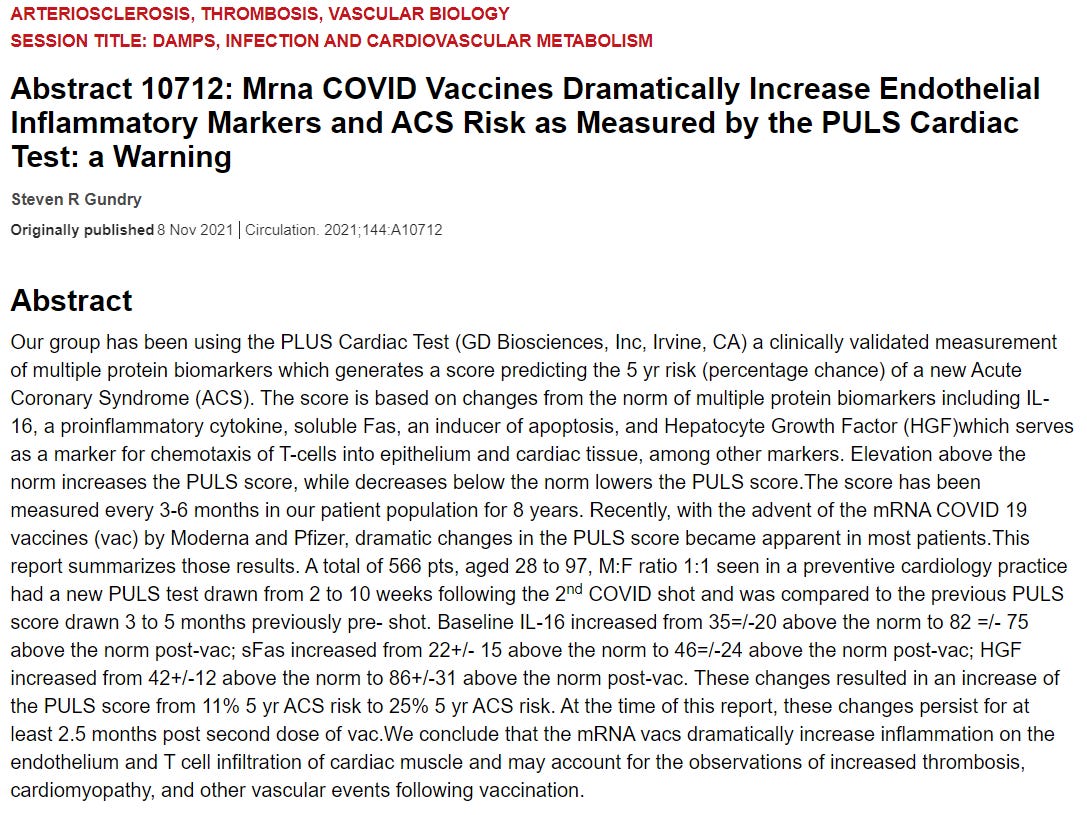
A first thing to note for those who haven’t read science papers, an abstract serves to act as a brief summation of a paper. It’s essentially a teaser that takes a little bit from the introduction, methods, results, and discussion, and usually it’s the only part of a paper you’re allowed to view if the paper is put behind a paywall. In this case, it seems that Dr. Gundry presented his findings at the American Heart Association conference. This may create a predicament as it may indicate a full paper may not be released. It’s hard to tell what’s going on at this moment so we will just analyze the abstract and extrapolate from there.
To start off, the researcher indicated his team used a PULS Cardiac Test. PULS stands for Protein Unstable Lesion Signature Test. As can be inferred from the acronym, the test is intended to measure biomarkers that may become elevated after an incident of heart inflammation/damage.

As both the abstract and the excerpt noted, the biomarkers may be examining endothelial damage that may result in Acute Coronary Syndrome (ACS).
The definition and pathophysiology of ACS are the following (Taken from StatPearls on PubMed):
Acute coronary syndrome (ACS) refers to a group of conditions that include ST-elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), and unstable angina. It is a type of coronary heart disease (CHD), which is responsible for one-third of total deaths in people older than 35. Some forms of CHD can be asymptomatic, but ACS is always symptomatic.[1][2][3]…
The underlying pathophysiology in ACS is decreased blood flow to part of heart musculature which is usually secondary to plaque rupture and formation of thrombus. Sometimes ACS can be secondary to vasospasm with or without underlying atherosclerosis. The result is decreased blood flow to a part of heart musculature resulting first in ischemia and then infarction of that part of the heart.
The endothelial comprises the inner lining of both blood vessels and lymphatics in the body. By measuring elevated biomarkers doctors are able to predict and prevent the occurrence of thrombosis (blood clots), myocardial infarctions (heart attacks), and other heart damage before it occurs.

The individual biomarkers aren’t important, just know that they’re intended to indicate that something may be occurring with the heart or blood vessels.
The last thing to note is that biomarkers were measured before vaccination, creating a baseline that the researchers could use as a comparison.
Although the abstract provides some good information, it still requires some context and additional information before we can understand the broader idea of the study, so there are some important details that we need to note.
The abstract doesn’t indicate a difference between Pfizer and Moderna vaccine recipients.
Hypothetically, if there is a relationship between the mRNA vaccines and heart issues we could argue that the Moderna vaccine should lead to greater elevated biomarker levels. This would actually help better argue that the vaccines may increase the risk of heart disease, as the Moderna vaccines contain a higher dose of mRNA than Pfizer (100 ng vs 30 ng, respectively). It would actually indicate a dose-dependent increase in inflammation. Unfortunately, the abstract does not differentiate between the two, and therefore no such conclusions can be drawn at the time.
The cohort has a very wide age distribution (Ages 28-97).
The PULS data for each participant was collected over a period of 8 years (it seems that the minimum age for this test is 20, and after collecting data for 8 years the youngest participant possible would be 28), and many factors come into play over those 8 years. Older participants may be more likely to have age-related biomarker elevations, and may be more likely to be prescribed medications for diseases such as high blood pressure, high cholesterol, etc. The researchers may have controlled for medication usage, in which case that would not be a concern. Nonetheless, it is very likely that age will play a contributing factor in regards to the study results. An easy way of clearing this up would be to stratify the ages and compare biomarkers between age demographics. As it stands, the overall increase in biomarker levels is concerning, and having age-stratified data would help put the information into perspective.
There are a few nitpicky things to point out, including that only 3 of the 9 biomarkers measured in a PULS Cardiac Test were included in the abstract. It would be nice to know whether or not the other biomarkers were elevated as well.
Also, the study does not indicate the causative agent for the elevated biomarkers. This is a highly controversial area and not much information has come out about what could be the cause of heart inflammation. There are 3 possible agents; the spike protein, the lipid nanoparticles (LNP), or the mRNA itself.
The only difference between the virus’ spike protein and the vaccine’s spike protein is a modification that prevents the vaccine produced spike from “clasping” onto the ACEII receptor. The issue here is whether or not the cascade of events (viral entry and propagation, release of viral proteins, etc.) involved in viral infection is the concern, or if the main concern is the ability of the spike protein to bind to the receptor in general. In that case, there would be concerns about the spike protein produced by the vaccine possible causing damage.
The LNPs are also an area of concern. The vaccines do not include an adjuvant (a compound that stimulates an immune response) since the LNPs were considered to serve as adjuvants. If the LNPs are able to travel they may be able to create an inflammatory response. Again, there’s not much research about LNP’s role, although some studies are beginning to emerge. Here’s a preprint from Ndeupen et. al. 2021 suggesting that the LNP’s may be highly inflammatory. I haven’t read the study in full, but it would indicate an area that should be looked into.
Here’s the researcher’s summary from the preprint:
In summary, the first vaccination’s side effects, except for CARPA, are likely associated with robust inflammation induced by the LNPs. In contrast, after the second vaccination, side effects could be further exacerbated by immune responses targeting cells expressing the vaccine protein or its peptide derivatives. Whether innate memory responses (Netea et al., 2011) to LNPs also contribute to amplifying the side effects remains to be determined (Figure 4). Overall, the robust inflammatory milieu induced by LNPs, combined with presentation of the vaccine-derived peptides/protein outside of antigen-presenting cells, might cause tissue damage and exacerbate side effects. Since self-antigen presentation in an inflammatory environment has been linked to autoimmune disease development (Charles A Janeway et al., 2001), this merits further investigation, albeit not detected here.
The mRNA may also play a role in inflammation, although this one is more complex. Our cell’s machinery is actually able to differentiate exogenous genetic sequences and present a response to clear out the foreign genetic material. The mRNA may be less likely to be an inflammatory agent, as it is sequestered within the LNP. Any free-roaming mRNA would end up being digested by ribonucleotides if noticed. That doesn’t mean the mRNA may play a causative role, but it is less likely out of the 3.
The results of this abstract are very concerning. It adds some perspective and justification to the possible increase in heart conditions post-vaccination. However, the results need to be met with skepticism. This study shouldn’t be seen as pure validation, but should indicate that more research should be looked into within this area. Also, remember that the PULS score indicates risk of ACS within a 5-year time span. It doesn’t mean that biomarkers will continue to be elevated after vaccination (measures were taken 2.5 months after the second dose) and so it’s important to see how long it would take for biomarkers to return to baseline, if they do at all. Nonetheless, the time frame immediately after vaccination would be seriously concerning, and incidences of heart disease or symptoms should be mapped to time frames post-vaccination.
The results of this study are very concerning, but we need to see if more information comes out in the near future. Hopefully the researchers release a full paper to examine, but until then the data should be seen with a good deal of skepticism.
Thank you for reading my newsletter. If you enjoy my articles please consider becoming a free subscriber in order to receive notifications.
And share with others who may find these newsletters interesting.
Also, please consider becoming a paid member. The research and work put into these articles takes many hours and being a paid subscriber allows me to continue to do this full time.
Citations
Gundry, S. R. 2021 Abstract 10712: Mrna COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test: a Warning. Taken from https://www.ahajournals.org/doi/10.1161/circ.144.suppl_1.10712
Singh et. al. 2021. Acute Coronary Syndrome. Taken from https://www.ncbi.nlm.nih.gov/books/NBK459157/
Ndeupen et. al. 2021. The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7941620/
I'm shocked, shocked, to that someone found a link between these injections and heart damage.
Well, not, not really. What's actually shocking is that it's in a paper published by the AHA.