


Have Monoclonal Antibodies Lost their Effectiveness? (Review)
Part I: Overview of the Common Antibodies in Circulation

With a new variants comes renewed concerns about escape mutations and whether vaccines may hold up.
Most variants of SARS-COV2 reside within the spike protein. It’s the antigen most responsible for binding to the ACEII receptor, so it should come as no surprise that the spike protein will bear most of the mutations.
Here’s a list of Omicron’s protein mutations for those interested (mutations are compared to the Wuhan/wildtype strain of the virus).

It stands to reason why there are concerns that vaccines may lose effectiveness; the antibodies produced by the vaccines, all of which target the spike protein, may not have the same neutralizing abilities in the wake of new mutations, especially because of the high number of spike protein mutations.
By that same logic the concerns are transferred onto monoclonal antibodies, one of the only outpatient treatments that have been granted EUA’s until recently with the approval of Molnupiravir and PAXLOVID.
This has raised some controversy over the use of monoclonal antibodies against Omicron, and many regions of the country have decided to pull its usage out of concern over their effectiveness in the face of a new variant. However, as of now there is a lack of real world evidence to validate such a move, leading to questions as to what evidence is being used to support such a policy.
We’ll work with the limited data so far and examine whether the concerns over monoclonal antibodies are warranted, and what this would mean for the coming Omicron landscape.
A Brief Overview of the Monoclonals in Play
Before we begin, I suggest people read my prior posts on Regeneron and mutations to get an understanding of the relationship between antigens, antibodies, and how mutations may alter the binding of antibodies. For the sake of the monoclonals mentioned in this newsletter, this brief review is also helpful for those wanting additional information.
Some of the important takeaways include the following (all taken from my Regeneron post):

So we’ll first take a look at the 3 most commonly circulating monoclonals.
REGEN-COV: Regeneron’s Monoclonal Therapy (Casirivimab & Imdevimab)
REGEN-COV aka Regeneron (also previously known as REGN-COV2), is the most well-known monoclonals in the world of COVID therapeutics. Regeneron contains two monoclonal antibodies, Casirivimab (REGN-10933) and Imdevimab (REGN-10987), and were manufactured by Regeneron Pharmaceuticals Inc.
The search for these two monoclonals are very interesting, as they relate to the interaction between natural/vaccine induced antibody production and their utility against viral antigens.
Both Casirivimab and Imdevimab were sourced through an arduous process of antibody selection. First, antibodies were sourced from either the convalescent plasma of previously infected COVID patients or from transgenic mice that expressed human ACEII receptors and were inoculated with SARS-COV2.
This is an important concept. Most people seem to be naïve to the fact that monoclonals work exactly the same as the antibodies produced through either natural infection or vaccines, and that’s because they are the same antibodies we produce! This concept seems to be lost on many people who seem to believe that monoclonals are contrived, experimental drugs when in reality nearly all of them have been sourced from prior infections. It’s an important idea to keep in mind when examining monoclonals.

The collection of antibodies were then tested to measure their binding efficacy and neutralizing capabilities. The end result were a group of antibodies that bound directly to the spike protein’s receptor binding domain or bound to outside regions of the spike protein.
Eventually, the choice was made between Casirivimab (REGN- 10933 which binds to a loop of the spike protein peripheral to the RBD) and Imdevimab (REGN-10987 which binds directly to the RBD of the spike protein).
One of the most important features of this dual antibody selection is the non-overlapping nature of these two antibodies. Because the paratopes (the varied amino acids of an antibody that bind to an antigen’s epitope) of these antibodies do not share epitopes a loss of function in one antibody due to a spike mutation should not affect the binding of the other. Unless massive accumulations occur, the hope was that both antibodies should not lose binding capabilities meaning that at least one of the antibodies should be effective in neutralizing the virus.

This ideal situation would only occur with the slow emergence of new mutations. However, COVID variants which contain several dozen spike protein mutations create a much more difficult scenario to assess. We’ll examine these in greater detail further on.
The Tortuous History of Eli Lilly’s Monoclonal Antibodies (Bamlanivimab & Etesevimab)
One of the other commonly used monoclonals comes from the pharmaceutical company Eli Lilly. This dual therapy, similar to Regeneron, were sourced from patients with prior SARS-COV2 infections.
Taken from Dougan et. al.:
Two such neutralizing monoclonal antibodies, bamlanivimab and etesevimab, were isolated from convalescent plasma obtained from patients with Covid-19 in the United States and China, respectively.27,28 These potent neutralizing monoclonal antibodies target the surface spike glycoprotein of SARS-CoV-2 that mediates viral entry into host cells.29,30 Bamlanivimab was developed by Eli Lilly after its discovery by researchers at AbCellera Biologics and at the Vaccine Research Center of the National Institute of Allergy and Infectious Diseases. Etesevimab was a result of the collaborative efforts of Eli Lilly, Junshi Biosciences, and the Institute of Microbiology of the Chinese Academy of Sciences.
Although used as a dual therapy, Eli Lilly first received an EUA for Bamlanivimab (LY-CoV555) alone. However, the emergence of the Beta and Gamma variants led to a large loss of neutralizing activity for Bamlanivimab, and Eily Lilly asked for their EUA to be revoked. They would eventually return and receive a renewed EUA for the combination therapy of Bamlanivimab and Etesevimab (LY-CoV016), which showed greater neutralizing capabilities in the wake of Delta.
Although promising, the dual therapy committed one of the greatest cardinal sins outlined above; both monoclonals bind to similar regions of the spike protein RBD. This creates a large problem. Because both antibodies share binding regions, they must compete with one another for binding to the proper spike region. This is a very dangerous situation, as you wouldn’t want your therapeutics to compete with one another for neutralizing activity. It also means that a mutation in the spike protein that affects one antibody is very likely to affect the binding of the other.
Unlike Regeneron, which would rely on the neutralizing activity of the other antibody should a deleterious mutation arise, Eli Lilly’s combination would likely lose activity in BOTH antibodies. Out of all of the combinations, Eli Lilly’s combination therapy serves as one of the most problematic in the face of emerging mutants/variants. Again, we’ll see why that will be the case later on.
The Unique Case of GlaxoSmithKline’s Sotrovimab
So far most of the monoclonals covered were derived from people with prior SARS-COV2 infection. Because of structural similarities between different virus strains, it would make sense that antibodies produced to fight SARS-COV may also work on SARS-COV2 if it targets shared regions between the two virus’ spike protein.
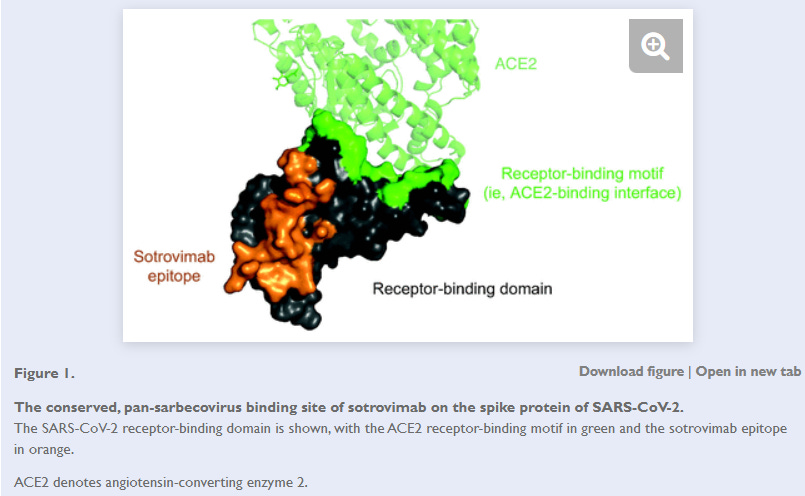
This introduces us to Sotrovimab, a monoclonal antibody developed by GlaxoSmithKline and Vir Biotechnology. Unlike the prior monoclonals mentioned, the parent monoclonal of Sotrovimab was actually sourced from a patient previously infected with the original SARS-COV strain from the 2003 outbreak. Because of this, Sotrovimab was designed to bind to a conserved region of the spike protein shared between both SARS-COV and SARS-COV2. This cross-reactivity with powerful neutralizing activity breaks one of the bullet points made above, although this seems to be a unique scenario due to the sourcing of an antibody specifically with this capability. In fact, the original researchers mentioned as much; the idea to source an antibody that targets a conserved region may suggest an extremely vital region for the spike protein, and as I have mentioned before vital binding regions are the least likely to mutate. This is why Sotrovimab, prior to the emergence of Omicron, has been highly effective against all of the previously circulating variants when tested in a nonclinical setting.
Here’s an excerpt taken from Gupta et. al.:
Sotrovimab, formerly known as VIR-7831, is an engineered human monoclonal antibody that neutralizes SARS-CoV-2 and multiple other sarbecoviruses, including SARS-CoV, the virus responsible for the SARS outbreak two decades ago.13 In fact, the parental form of sotrovimab, S309, was isolated from a SARS survivor.13 We hypothesized that a monoclonal antibody that neutralizes all sarbecoviruses would target a highly conserved epitope that would be functionally retained as SARS-CoV-2 evolves (Fig. 1).
Even more interesting, Sotrovimab contains a mutated effector region. The effector region of an antibody is the structural region furthest from the antibody’s epitopes. If you imagine the “Y” shape of an antibody, the epitopes exist at the top of the Y’s prongs while the effector region is the base stalk. The effector region is important for binding to immune cells and providing immune-dependent responses to pathogenic infections. The mutation found in Sotrovimab seems to confer greater effector capabilities, and in fact it provides Sotrovimab with an extraordinary median half-life period of nearly 49 days.
For all of the reasons mentioned above Sotrovimab has been given the name of “super antibody” due to the reduced odds of running into escape mutations. However, although the odds are greatly reduce the chances of escape mutations arising are still there. In Sotrovimab’s fact sheet they reference the emergence of an escape variant during in vitro testing. They also provide a few concerning amino acids that would also lead to antibody escape.
Although Sotrovimab seems like one of the most promising monoclonals on the market, we still need to disabuse the notion that there is no possibility of it losing effectiveness in the face of new mutations.
The search for monoclonal antibodies to target SARS-COV2 encapsulates the scientific rigor and methodology that is required to find promising therapeutics. It also indicates the relationship between scientific discovery and real-world practice.
Eli Lilly originally started with only one monoclonal antibody, and although Bamlanivimab showed strong initial neutralizing activity it quickly did not hold up in the face of the emerging Beta and Gamma variants, as would be expected with the use of one monoclonal therapy. This led to the addition of another antibody (Etesevimab) which targets a similar region as Bamlanivimab. Although this dual therapy showed promise, it commits the cardinal sin of overlapping binding regions, meaning it is the most likely of the available monoclonals to become ineffective against newer mutants/variants.
Regeneron took a different approach, and instead of utilizing a monoclonal that binds to similar regions decided to administer a dual therapy that did not contain overlapping paratopes. Casirivimab binds peripherally to a loop of the spike protein while Imdevimab binds directly to the RBD of the spike protein. Such a combination is less likely to experience reduced effectiveness as mutations arise, although the sudden emergence of multiple mutations are likely to lead to drastic reductions in effectiveness.
GSK took the most unique approach. If emerging mutations are a concern, it would stand to reason that finding the most conserved spike protein regions, along with an antibody that binds to these regions, is likely to provide the least odds of running into escape mutations. Comparing the spike protein structures of SARS-COV and SARS-COV2 led to the discovery of Sotrovimab in a 2003 SARS-COV outbreak survivor. So far, this method of screening and discovering Sotrovimab has made it one of the most promising monoclonals to date. Nonetheless, the concern still exists that a variant may escape the neutralizing capabilities of Sotrovimab.
Part II, where we dive into some of the available preprints and examine molecular dynamics/ nonclinical studies will be out later today. Please stay on the lookout!