
Fluvoxamine- The Little SSRI that Could: Part IV
Nonclinical Examination of Fluoxetine/Fluvoxamine & Emerging Clinical Trial Results

With Mechanisms of Actions out of the way, we can now focus on Clinical Trials. However, I’ll first start with two more in vitro studies; one that examined Fluoxetine and another that examined Fluvoxamine against SARS-COV2 infection. I will go through these briefly and focus mostly on the pertinent results.
Note: Obligatory comment about not taking this as medical advice but use it to make informed decisions. Please consult a medical professional in regards to prescription medications. This is intended to be informative, not prescriptive.
In Vitro Assay of SSRIs Fluoxetine & Fluvoxamine
The serotonin reuptake inhibitor Fluoxetine inhibits SARS-CoV-2 in human lung tissue (Zimniak et. al.)
This is a very brief, straightforward assay in which researchers wanted to fast-tract the search for possible SARS-COV2 antivirals by screening drugs that have had prior indication of effectiveness and testing them against SARS-COV2:
To circumvent time-consuming clinical trials, testing whether existing drugs are effective inhibitors of SARS-CoV-2, has led to the discovery of Remdesivir6. We decided to follow this path and screened approved medications "off-label"7 against SARS-CoV-2. In such a trial, we investigated the effect of the serotonin reuptake receptor inhibitors (SRRI) Fluoxetine, Escitalopram, and Paroxetine on viral replication. Fluoxetine blocks the serotonin reuptake transporter in the presynaptic terminal. Fluoxetine is applied at a concentration of 20 mg daily.
*It should be noted that Fluoxetine’s dosage is relative lower than Fluvoxamine, with a maximum dose of Fluoxetine usually around 80 mg while Fluvoxamine can be up to 300 mg. Take these dose differences into account, and if mix ups occur in this post take into account the overall lower dose of Fluoxetine when making comparisons.
It’s interesting that the researchers draw parallels to Remdesivir, one of the only repurposed drugs that has been adopted as standard practice against COVID. Strange that many other therapeutics were not afforded the same fast-tracking process, and so I find this comment quite ironic, but we’ll focus on that more later.
Even though the researchers commented on Fluoxetine’s role as an SSRI, the study here is not powered to address whether this is the actual way that Fluoxetine exhibits antiviral properties, and remember we have gone over several other MOAs already.
The researchers provided the 3 above labeled SSRIs at different concentrations to both Vero and Huh7 cells (measured in ug/mL). After incubation at the respective concentrations viral replication was measured over the course of 3 days. Fluoxetine hindered viral replication at standard therapeutic doses used to treat depression (0.8 ug/mL), indicating that typical dosing regimens for other diseases may be just as effective at treating SARS-COV2 infection (Fig. 1A). Fluoxetine also did not show cytotoxicity at these therapeutic doses, suggesting a safe profile with respect to the cytotoxicity assay (Fig. 1B). Escitalopram and Paroxetine did not significantly stop viral replication (Fig. 1A).

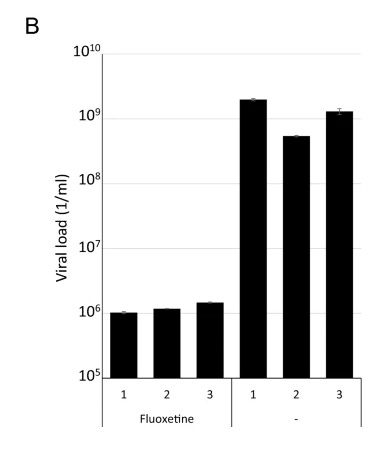
Afterwards, researchers wanted to examine the actual antiviral effects of Fluoxetine in human models by using human precision-cut lung slices (PCLS) and incubating them with either Fluoxetine or Lopinavir. After 3 days the supernatants from the lung tissue were then used to infect Vero cells over the course of 3 additional days. Isolates were taken and viral titers were determined by rt-PCR. Fluoxetine treatment of lung tissues showed lower viral titers, suggesting that Fluoxetine reduced viral replication compared to Lopinavir which did not show any effects (Fig. 2B).
T
his was a simple straightforward study that indicates possible therapeutic effects of using Fluvoxamine. More importantly, the effective concentrations used in this study were similar to those prescribed for depression, and so there’s already a reference population to examine for Fluoxetine’s safety. Considering that Fluoxetine has been around for decades (a few years longer than Fluvoxamine) and tends to be prescribed longterm, there really shouldn’t be longstanding skepticism about prescribing Fluoxetine for COVID (note: this is not prescription to take Fluoxetine nor Fluvoxamine, but is merely informative assessment of the situation).
I do have to say that the organization of this study is strange. Even though the researchers mentioned using Lopinavir, there are no references to those results or any figures included. The researchers also included a figure (Fig. 2A) showing that they incubated cells with both Fluoxetine and other viruses or vaccine strains and found that Fluoxetine did not inhibit viral replication there. It’s strange that this was included without any reference within the body of the study, so I’m quite skeptical as to the layout of this study and how much review was put over the organization of the information.
Nonetheless, this study does provide evidence to further examine Fluoxetine’s usage in clinical trials, although the study should rightfully be viewed with a bit of skepticism as well.
Antidepressant and Antipsychotic Drugs Reduce Viral Infection by SARS-CoV-2 and Fluoxetine Shows Antiviral Activity Against the Novel Variants in vitro (Fred et. al.)
In this study a group of drugs were examined to see if they may provide any benefit against SARS-COV2 in vitro:
In the present study, we addressed if the psychoactive drugs can be used to reduce SARS-CoV-2 infection of host cells in vitro. We show that pharmacologically diverse antidepressant drugs, as well as several antipsychotics were able to reduce the infection by pseudotyped viruses harboring SARS-CoV-2 S protein. Treatment of human lung epithelial cell line Calu-1 infected with the B.1 lineage of SARS-CoV-2 with these drugs was also successful in reducing the amount of infectious virus.
One thing I will skip over is the examination of Fluoxetine and its direct interaction with the spike protein. The precarious nature of SARS-COV2’s spike protein, along with its high mutation rate makes direct targeting by pharmaceuticals a very risky move. Remember that the treatment should fit the disease, and if the spike protein is constantly changing I would argue that, aside from antibodies the direct targeting of the spike may not be something worth investigating if effectiveness will vary greatly between variants.
Now, with that out of the way we will focus on the pertinent experiments. Fortunately, the researchers provide an outline so this will help to follow along with their workflow.

In Protocol I researchers took HEK293T-ACE2-TMPRSS2 cells (cells that express higher levels of ACEII and serine proteases) and infected them with pseudovirus. At the same time the cells were treated with different antidepressants and the level of viral infection was measured. Researchers also conducted a parallel experiment to examine the cytotoxic effects of the drugs at the corresponding concentrations. Overall, viral replication was reduced in nearly all assays in a dose-dependent manner (Fig. 2, red lines). Also, at higher concentrations cytotoxicity was seen in several of the antidepressants including Fluoxetine and Fluvoxamine (Fig. 2A & 2D, blue lines).
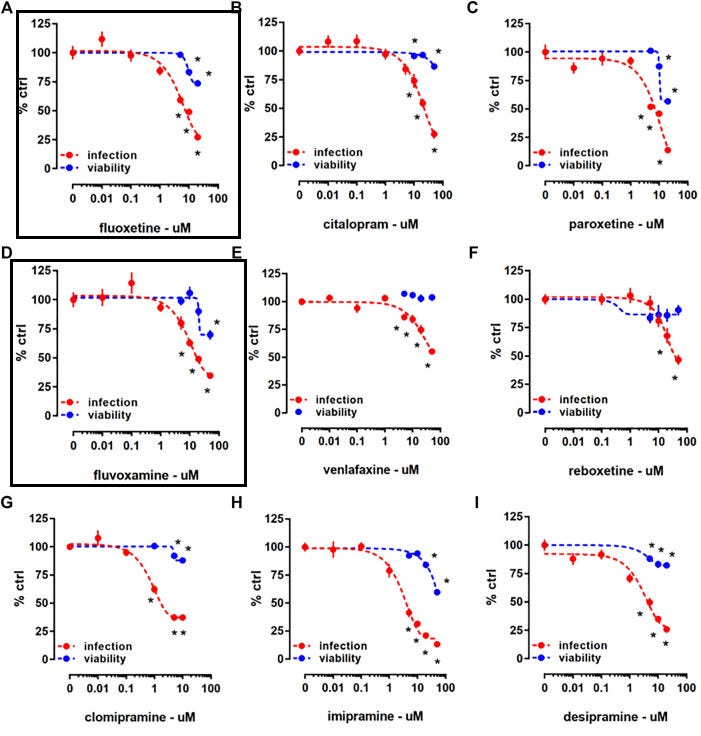
An examination of both viral replication and cytotoxicity helps to compare possible risk/benefit analyses. Remember that you don’t want to provide a medication if the therapeutic dose may also cause adverse reactions. The important thing to note here is whether the cytotoxic doses are the doses seen in typical regimens for depression. We have already indicated from Zimniac et. al. that effective doses of Fluoxetine occurred at typical doses used to treat depression (0.8 ug/mL, or ~2.6 uM), and so it may be appropriate to assess the results of this experiment at lower concentrations (such as 10 uM). At such a concentration we can see that cell viability was not greatly affected by the doses of Fluvoxamine/Fluoxetine provided to cells.
This is further validated in Protocol II, where SARS-COV2 infected Calu-1 cells were treated with anitdepressants at various concentrations (0, 5, 10, and 20 uM) for 48 hours. Genome copies of SARS-COV2 were then examined along with cell viability. The results suggest that therapeutic doses of Fluoxetine may reduce cell viability (Fig. 3A-3C), but once again we must assess the results from the perspective of viable, typical doses. It should also be reiterated that in vitro cytotoxic effects are not reflective of toxic effects in humans.

The researchers also included experiments examining antipsychotics and Fluoxetine’s effect against many of the prior variants pre-Omicron. However, for brevity I will exclude those experiments and suggest readers take a look for themselves if curious. Just remember to view Fluoxetine’s effect across variants with a skeptical eye as any direct binding to the spike protein may be heavily attenuated with spike protein mutations.
Overall, what these two studies have provided is not just the in vitro safety/efficacy of SSRIs as a COVID treatment, but that many of these therapeutics are effective at doses already commonly used when prescribed for depression and other cognitive impairments. The question of dosage has weighed heavily on many COVID therapeutics. One group may argue that a drug is not effective based on one clinical trial while an opposing argument may say that the dosing was far too low to be effective. Dexamethasone is one of the best examples, where many proponents have argued that the typical dosage seen in hospitalized patients are scant compared to what should actually be administered. Corticosteroids provide a difficult perspective where the concerns over continuous viral replication and a hyper inflammatory immune response must be balanced for the safety of patients.
Ironically, that perspective would add more to the idea of examining and repurposing outpatient therapeutics where the risks of using many of these repurposed drugs could be kept at a minimum because the severity of the disease is at a minimum during the time of treatment. This is heavily reiterated in my remarks about Remdesivir and Hydroxychloroquine, and it is likely why the approaches taken to these treatments have been very wrong as they relate to COVID.
Nonetheless, having nonclinical evidence that actually provides viable, effective doses of both Fluvoxamine and Fluoxetine adds further validation to examining these therapeutics within the context of early COVID treatment in humans.
Examining Clinical Studies
With all of the prior information out of the way we can finally turn our attention to clinical trials. First off, I would suggest people look at the c19early treatment website if they haven’t done so already (here’s the link specifically to Fluvoxamine). Now, whether anyone agrees with the information displayed I think the layout and presentation is worth looking into. Not only is the information quite exhaustive, the presentation makes it highly approachable as well.
With that being said we will examine some of the available clinical trials. Just like with many other prior drugs, the clinical trials conducted so far have been limited, but we will go through what’s available based on the emergence of these studies.
Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19 (Lenze et. al.)
The first study will be the one that kicked off the examination of Fluvoxamine for COVID. In this study, researchers conducted a double-blind, randomized, fully remote (contactless) clinical trial utilizing participants from a community-living home.
The study design is outlined below:
152 patients (80 in the Fluvoxamine, 72 in the control) enrolled between April and August 2020
Mean age: 46, SD of 13 years
109 (72%) Female
Treatment group was given stratified Fluvoxamine dosage (50 mg on day 1, 100 mg 2x a day for the next 2 days, then 100 mg 3x a day up until day 15)
Primary outcome was based on worsening symptoms including a reduction in oxygen saturation below 92%, pneumonia development, and increasing shortness of breath within 15 days of randomization.
Overall, none of the Fluvoxamine participants showed clinical deterioration while 6 of the 72 placebo participants showed clinical deterioration. Out of the 6 participants who deteriorated, 4 required hospitalization and 1 required ventilation. Fortunately none of the participants died.

This study provided the first clinical evidence in support of Fluvoxamine’s use for COVID treatment, as none of the patients within the treatment group showed signs of clinical deterioration compared to the placebo group.
However, the results should be viewed within the context of the study limitations. Aside from the obviously low number of patients, the study had a long period of enrollment from the time of symptom onset (within 7 days of positive test). We should know full well by now that timing is important for treatment. Because this study took place near the beginning of the pandemic these results are most likely reflective of wildtype/D614G strain of the virus and should be examined with this in mind.
Also, the study skewed fairly young (late 40s with a SD range between mid 30s to early 60s) and may also add bias to skew the data towards a population that may not suffer as severe of COVID outcomes. A large proportion of patients (over 70%) were also female, and sex-based dynamics of SSRI response as well as viral infection severity should be taken into account as possible confounding variables.
What’s unique to this study is the contactless approach where boxes were provided to patients including instructions, an oxygen saturation monitor, automated blood pressure monitor, thermometer, and blinded drug. Although many doctors have encouraged people to keep a few of these items on hand for their COVID infection to monitor their vitals, the high possibility of human error should be taken into consideration. Considering that a reduction in oxygen saturation is considered one of the endpoints for this study, we can see how misuse of these instruments could alter the results collected (patients self-assessed their own measures). A patient who may not understand how to use the oxygen saturation monitor may provide an incorrect reading and thus affect the clinical outcome results. This could explain the large number of participant drop offs, although that may also be reflected of typical clinical trial participant drop offs, along with possible concerns about being enrolled within a study based on an emerging pandemic where not much information was available at the time.
It’s strange that the researchers used an oxygen saturation cutoff at 92%. From what I’ve seen the typical oxygen saturation cutoff has been around 95%, and so one has to wonder why the 92% cutoff was used. It could be that supplemental oxygen has been suggested by the NIH for when patients’ oxygen saturation falls within the range of 92%-96%, and so it may reflect the lowest end of requiring supplemental oxygen.
One last thing to point out is the dosage used here. The maximum indicated dosage of Fluvoxamine has been 300 mg/day and tends to be provided at such a high dose for possible antipsychotic effects. Questions should be raised as to possible adverse reactions and whether such high doses may increase incidences of suicidal ideations or mania. Granted, the lower rate of adverse reactions within the treatment group along with the shorter treatment period relative to typical prescriptions may keep such concerns to a minimal.
Overall, these initial results proved promising, although many caveats are required to assess the information and the generalizability of said results. Nonetheless, this study helped kick off further studies utilizing Fluvoxamine.
Prospective Cohort of Fluvoxamine for Early Treatment of Coronavirus Disease 19 (Seftel, D. & Boulware, D.R.)
The results of the Lenze et. al. study proved fortuitous, as Dr. Seftel applied the results in a real-world setting. At the end of 2020 a massive COVID outbreak took place at a race horse track in California, spurring the authors of the paper to deploy Fluvoxamine to willing employees. Apparently, Dr. Seftel is a tending physician at the track, and so that should provide some perspective as to why a race horse track, of all places, would be at the center of this study.
This study was considered open-labeled as people were able to choose whether to receive treatment. Enrolled patients were given the option of treatment the same day that they received a positive antigen test.
The study and demographics breakdown are provided below:
113 volunteer patients
Median age was 42 (IQR was 33-56)
75% Men
84% Latino, 14% White
65 volunteers opted for Fluvoxamine, 48 opted for observation only
A majority of symptomatic patients opted in for Fluvoxamine; a majority of asymptomatic patients opted for observation alone
More diabetic patients opted in for Fluvoxamine than did not; more treated hypertension patients opted out of Fluvoxamine than opted in showing a reversal compared to diabetic patients
Fluvoxamine volunteers were provided 50-100 mg loading dose followed by 50 mg 2x a day for 14 days.
During the treatment period none of the Fluvoxamine patients required hospitalization, ICU admission, or died. However, 6 of the opt out patients required hospitalization, with 2 requiring ICU admission and mechanical ventilation, and 1 passed away.

What’s interesting is that none of the patients who received Fluvoxamine had symptoms at day 14 while 60% of those who didn’t receive treatment still had symptoms, with the common symptoms being persistent anxiety, difficulty concentration/memory issues, fatigue, insomnia, myalgia/arthralgia (muscle/joint pain), and headaches.

The results of this study provided further validation of Fluvoxamine’s effectiveness against COVID, as well as helped to validate the results of Lenze et. al.’s study. More importantly, this study provided real-world evidence of outpatient treatment as indicated by the outbreak in a workplace setting.
Separate from the Lenze et. al. protocol was the lower dosage used (50 mg 2x a day- 100mg/day overall) which suggests that even lower doses of Fluvoxamine may be viable to treat COVID relative to the Lenze et. al. protocol. This also aligns with the typical lower dose regimen usually used with Fluvoxamine.
There are a few things that require pointing out with this study.
For one, many comorbidities have been associated with worse COVID outcomes, and so it would be difficult to extrapolate the information without multivariate analyses as more diabetic patients enrolled to receive treatment than those who didn’t. On the other hand, more of the patients who were receiving hypertension treatment opted to not receive Fluvoxamine than those who had hypertension and opted in.

Barring the inclusive nature of these comorbidities it’s interesting why such a dynamic took place. Could it be that those who were prescribed ACEII inhibitors for hypertension may have conflated some type of protective role to these medications, and thus did not believe they needed additional treatment? There’s really no evidence to suggest that, but we also can’t forget that most of the initial information surrounding COVID was that it bound to ACEII receptors and that there may be some concerns over taking ACEII inhibitors and how that may affect COVID infections. We also need to take into consideration the benefits of Fluvoxamine with respect to diabetes and other inflammatory diseases. This study was not powered to examine whether the results within the Fluvoxamine group could be attributed to Fluvoxamine’s possible antiviral properties, or if the alleviation of comorbidities may have played a role as well. Remember we have previously discussed that elevated ceramide levels and ER stress are found in diabetic patients, and therefore Fluvoxamine may play a role across many different diseases and that may have provided some additional benefits.
With the large portion of opt-out volunteers still experiencing symptoms at day 14, one has to wonder if this may be symbolic of possible long COVID. The results here clearly indicate that not only did the Fluvoxamine group not require hospitalization, but that none of them had reported symptoms on day 14. In fact, by day 7 a larger number of Fluvoxamine patients saw a reduction in respiratory rate relative to the control groups. A few things that confound these results is the positivity rate within the opt-out group. It could be that those within the opt-out group may still be experiencing viral replication and may explain the lingering symptoms. The researchers did not conduct either PCR or antigen tests at the 14 day mark and so it’s hard to assess where the symptoms may be coming from whether it be continuous viral replication or possible long COVID symptoms.
Lastly, the use of an open-label, volunteer protocol will greatly alter who decides to take Fluvoxamine and who decides to opt out. As indicated in this study, people who are likely to be experiencing more symptoms at the time of enrollment and diagnosis may be more inclined to receive treatment, and therefore both the treatment group and control group may contain heterogeneity and may not be entirely comparable.

Nonetheless, if a higher number of symptomatic patients opted to take Fluvoxamine, we should expect some bias against Fluvoxamine use if it was not beneficial (if we assume that greater symptom onset correlates with a greater likelihood of severe illness). Instead, we can clearly see that none of the patients within the Fluvoxamine group required hospitalization and in fact improved quicker than the control group, which would actually add more validity to Fluvoxamine as being an effective therapeutic.
Once again another study proved Fluvoxamine beneficial within an outpatient setting. Even more important is that this study is reflective of a real-world incidence of Fluvoxamine, and thus contributes even further to the idea of utilizing a cheap, generic, widely available therapeutic for repurposing against COVID.
Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial (Reis, et. al.)
Both of the prior studies suffered from low sample sizes and a good deal of heterogeneity. Having a good sample size is vital to allowing for greater generalizability to a much large population. Here, we will examine the TOGETHER clinical trial in regards to Fluvoxamine and see how it fares with a larger treatment group.
The TOGETHER trials have been quite a point of contention. They’ve been pointed to quite extensively for the trials on Ivermectin and Hydroxychloroquine as proof of lack of effectiveness, resulting in many critiques about the study protocols. Fluvoxamine has not met the same form of infamy, and (spoiler alert) is actually the only therapeutic from the TOGETHER trials to have been found to be effective.
This makes for an interesting conundrum. Do we accept the trials that suggest both Ivermectin and Hydroxychloroquine are ineffective while at the same time accepting the study about Fluvoxamine’s effectiveness? Or is it more appropriate to take into account the differences in MOA, bioavailability, and other forms of heterogeneity of protocol and patient structure? For the sake of this study, we will not dive into such a comparison, but just know that such critiques have been previously made against the results of the TOGETHER trials, and that the Fluvoxamine trials were conducted at the same time as the other therapeutics.
This randomized trial took place in Brazil at 11 different sites with a similar protocol as seen in other trials:

One thing to point out here is that a shorter time frame was used here (10 days vs 14 days). Also, the Fluvoxamine dosage used here fell between the prior two studies (100 mg 2x a day).
As is typical of the other TOGETHER trials patients with at least one high risk association were included in the study. In order to meet eligibility criteria patients were also included if they presented with symptoms within 7 days of COVID screening.
For more information on the demographic make-up of participants, refer to Figure 2 of the paper. In general, many of the demographics were even among both the Fluvoxamine group and the control group, including the make up of the high risk categorizations.
Slightly more females were enrolled than males, the median age was 50 (IQR 38-56).
For those unaware, IQR refers to interquartile range. In statistics, if you take the median (middle) value, in this case 50, the IQR takes into account the make up of the 25% of patients above the median age as well as the 25% below the median age of 50. In an evenly distributed population, you should expect a similar IQR for the upper half compared to the lower half. However, there is a discrepancy here, as the upper range indicates that 25% of participants fall within the age range of 50-56 while the lower range indicates that 25% of participants fall within the age range of 38-50. This is essentially a difference of range of 6 and 12 years, respectively. When looking at age distribution, the smaller range indicates that many of the participants’ ages clumped together around the early to mid 50s range while younger patients were more widely distributed. In short, it means that a larger portion of patients skewed slightly above 50 in this study
This actually contrasts the patient make-up seen in Seftel, D. & Boulware, D.R. where the lower IQR was smaller than the upper IQR, suggesting that the distribution skewed slightly younger in that study.
This is not a huge issue, but should be taken into account when the concerns over age, risk factors, and disease severity are being examined within the context of a study.
Overall, the results mimic those found in the two prior studies such that hospitalization rates were lower in those given Fluvoxamine treatment compared to placebo:

In the fluvoxamine group 79 (11%) participants had a primary outcome event compared with 119 (16%) in the placebo group (table 2). Most events (87%) were hospitalisations. On the basis of the Bayesian beta-binomial model, there was evidence of a benefit of fluvoxamine reducing the composite primary endpoint of hospitalisation defined as either retention in a COVID-19 emergency setting or transfer to tertiary hospital due to COVID-19 (RR 0·68; 95% Bayesian credible interval [BCI] 0·52–0·88) in the ITT population (figure 2A) and RR 0·69; 95% BCI 0·53–0·90 in a modified ITT population (figure 2B). The number needed to treat was 20. Per-protocol analysis showed a larger treatment effect (0·34, 95% BCI 0·21–0·54). The probability that the event rate was lower in the fluvoxamine group compared with placebo was 99·8% for the ITT population and 99·7% for the mITT population (figure 2A, B). When the DSMC met on Aug 5, 2021, it recommended that the TOGETHER trial stop randomly assigning patients to the fluvoxamine group, as this comparison had met the prespecified superiority criterion for the primary endpoint (prespecified superiority threshold 97·6%).
Secondary outcomes also showed greater improvement within the Fluvoxamine group (Table 3, not included) including a lower death rate, lower need for mechanical ventilation, and a greater time of death relative to the control group. Also, subgroup analysis showed greater risk reduction within the Fluvoxamine group as well (Figure 3, not included).
Once again, this study helps support the idea of providing Fluvoxamine to treat COVID. What’s interesting is that the interim results were so promising that comments were made to end the trial early due to superiority of the results. We’ve seen how such an approach has backfired, as was the case with Molnupiravir, and so there may be concerns about differing results if the trial was to continue. However, the largest issue with Molnupiravir’s latter half of the Phase III clinical trial was the emergence of Delta. The shorter replication period for Delta compared to prior variants is likely to contributed to the atrocious latter results. Because the TOGETHER trials took place in Brazil another variant was in circulation during the early portion of the study (P.1, or Gamma) with Delta taking over during the later winter/early spring months of the southern hemisphere. It’s actually quite strange how many interim studies stop abruptly with the emergence of Delta. We should know well by now that the variant plays a determining factor in treatment timing along with the type of drug deployed, and so we can see how this may alter results if enrollment and treatment continued.
I won’t discuss the dosage as it falls within the middle of the dosage regimens of the prior studies. The same goes for the enrollment period (7 days within positive test and symptom onset), as we may assume that earlier treatment is always better. It’s far better to treat the disease at a lower viral load than it is when other confounding variables are at play such as inflammation and organ damage.
A point should be made about the 10 day regimen used in this study. Considering that the prior studies called for a two-week protocol it’s strange that this study did not do the same. It is likely due to having a standardized protocol across all treatment groups. However, one has to wonder if the outcomes may be different if allowed to follow a 2 week protocol. Although we may assume better outcomes within the Fluvoxamine group if allowed to continue 4 extra days, there’s no way of knowing within the context of this study.
One strength of this study is the study size which provides several magnitudes greater patient enrollment as compared to the prior two studies. Also, the inclusion of high-risk groups adds further evidence to Fluvoxamine’s well-tolerated, high safety profile. The combination of both being very safe and effective makes Fluvoxamine a highly attractive drug candidate. Add on the cheap cost of Fluvoxamine and there really appears to be no excuse about the hesitation seen with prescribing Fluvoxamine.
The researchers noted that Fluvoxamine is not included within the WHO Essential Medicine List but that Fluoxetine is. They raised the question as to the association between classes of drugs rather than an individual therapeutic. We have continuously reiterated in previous posts the emerging importance of examining SSRIs as a whole, and several in vitro studies have pointed to the beneficial effects of antidepressants. Because prior evidence already exists, there should be greater emphasis placed on conducting clinical trials that further assesses the validity of the SSRI class of therapeutics.
Early Fluvoxamine Use for COVID is Heavily Supported by the Science
Usually repurposed drugs for COVID have been met with mixed evidence. The dosage and treatment time period can be all over the place, and so the spotty records may sometimes be attributed to inconsistent studies between protocols. Yes, the evidence so far is limited, but we can clearly see that the evidence supports early Fluvoxamine use in treating COVID.
Considering that Fluvoxamine has been in use for several decades there have been a clear safety signal. Even more important is that the dosage used within the clinical trials, as well as the in vitro studies mimic the same dosage typically used to treat depression. Paired with the results of these studies and we can see that the evidence against using Fluvoxamine is not supported by the literature. I did not even cover possible inpatient treatment effects of Fluvoxamine, but so far some of the studies also provide evidence of possible effectiveness in hospitalized patients as well providing even greater avenues for treatment and research (Calusic et. al., Hoertel et. al.).
The argument surrounding both Ivermectin and Hydroxychloroquine has created a very heated atmosphere as to the direction modern medicine has taken. When cheap drugs that have been in use for decades have suddenly become demonized one has to wonder what could cause such a pivot in perspective. Even if we say that they are ineffective for treating COVID, their relatively safe profile makes it hard to argue against a doctor’s imperative to attempt to treat a patient.
Note, I am not a doctor and please don’t take my writings as medical advice.
I’ve become quite tired of having to constantly reiterate that at the number of outpatient treatment options for COVID is severely limited. The only available monoclonal antibody now is Sotrovimab, and its availability has been severely limited with the coming of Omicron. It’s also been severely targeted as some “miracle cure” pushed by vaccine skeptics, at least from the perspective of many vaccine zealots who have touted nothing but vaccines as the panacea to end the pandemic.
Molnupiravir still has a very concerning safety and efficacy profile. We still don’t know the possible mutagenic effects of Molnupiravir, and as far as I am aware Merck has not addressed the horrendous latter half of their Phase III clinical trial. PAXLOVID is likely to be effective, but considering that its distribution will be severely limited, and that both Molnupiravir and PAXLOVID are expected to cost several hundred dollars per treatment for the hope that these drugs will be beneficial I can’t help but think of possible malfeasance on the part of the medical and pharmaceutical industry.
I usually have not put this into perspective, but let’s assume that the cost of a Fluvoxamine regimen hovers around $20-30. Even at the severely conservative end, a doctor would be able to treat over 20 patients for every 1 they can treat with either Molnupiravir or PAXLOVID at a similar cost. Again, this is a severely conservative estimate and is likely to be orders of magnitude higher. Even just taking this perspective the idea that any treatment would be barred from use with such a population benefit ratio should raise many question.
Note: This article originally stated that Fluvoxamine could treat 100 COVID patients for every 1 Molnupiravir/PAXLOVID could treat. That number came from an estimate in which $4 was used to calculate Fluvoxamine’s cost. However, I went with the $20-30 range commented on within my first post but forgot to take that change into account. The number has now been changed to 20 rather than 100.
Both Ivermectin and Hydroxychloroquine have been highly contentious drugs, and yet Fluvoxamine has gone relatively unscathed with respect to being targeted as some form of a “pseudodrug” treatment for COVID. The idea that Fluvoxamine has not been severely targeted by doctors or the mainstream press, has essentially gotten approval through the TOGETHER trial as the only effective treatment, AND is still not being fully utilized as a treatment option speaks of something truly horrifying occurring behind the scenes. For a drug who has not been dragged through the mud to the same extent as other repurposed drugs, and is still not being deployed should speak volumes as to the nature of the entire COVID narrative.
Regardless of our beliefs, we make it a goal to follow the science as closely as possible, and when all signs point to the effectiveness of Fluvoxamine and it is still being ignored as a possible therapeutic, we have to wonder if we are still working within the realm of science or if the political nature of COVID has run far too deep, placing us all in harm’s way for the benefits of a select few pharmaceutical elites and bureaucrats.
The final post will be tangential and I will go more into a possible hypothesis to try to connect COVID infection, vaccines, and ER Stress.
You are wise and perspicacious; more power to you , as you strive to benefit all of us , and have already done so much good
An amazingly satisfying continuation of the theses being developed, kudos being due to the author. The completed series will, I venture to guess,be a superbly cogent separate publication if the author decides on that route of distribution .