
Fluvoxamine- The Little SSRI That Could: Part II
Nonclinical Examination of Lysosomotropism and the ASM/Ceramide Pathway

This post has gone over the email limit and may become truncated. If so, please check for the full post at the Substack Page.
Just a bit More Information
So, I said that I would truncate the information in the prior post, but there’s just a few more things to add that are important for evaluating the nonclinical studies in this post. This will mostly include the other few MOAs not yet covered from the schematic diagram and a few more additional points.
SARS-COV2 Viral Entry
So we’ve mentioned that Omicron’s main route of viral infection is likely to depend upon the endosomal pathway to a greater extent. However, it should be worth noting the 2 routes of viral entry into host cells.
Viral membrane fusion to host cells: When SARS-COV2 comes into contact with ACE2 cells, the spike protein of SARS-COV2 gets cleaved by serine proteases. The cleavage of S1 and S2 subunits allows the S2 subunit to fuse to host cell membranes eventually leading to the fusion of viral membrane to host cell membrane. Afterwards, the viral genome is then spewed into the cytosol of host cells which eventually leads to viral replication and protein production.
Endosomal Pathway: When SARS-COV2 attaches to the surface of of a host cell, it may not fuse with the host cell membrane. Instead, another set of events leads to the host cell lipid membrane budding inward, carrying the virions into the cell through endosomes (specifically early endosomes). As these viral packages make their way deeper into the cell the pH of these endolysosomes continue to decline (becomes more acidic). When they reach a low enough pH, lysosomal enzymes are activated leading to the eventual escape of viral particles into the host cell where they then undergo viral replication and protein production. It is here that Hydroxychloroquine and Fluvoxamine (along with other SSRI’s) are likely to elicit their lysosomotropic effects. By increasing the pH here, lysosomal enzymes are not activated and viral particles are not released from the lysosomes. A similar effect is likely to occur with the export of newly made viral particles as well. This will be a topic that will come up again when we take a closer look at nonclinical studies.
Fluoxetine vs Fluvoxamine- Interchangeable SSRI’s?
Usually, I try to refrain from interchanging two different drugs in case there are subtleties of MOAs that are themselves not interchangeable (Granted, I have interchanged Chloroquine and Hydroxychloroquine because it’s only a change of one -OH group).
However, many people have considered Fluoxetine to be a somewhat viable alternative to Fluvoxamine. Steve Kirsch has mentioned Fluoxetine when Fluvoxamine is not available, and many literature reviews tend to include both of them together.
Fluoxetine is quite similar in structure to Fluvoxamine, although it mostly differs with the additional cyclic ring and N-methyl group. It is usually sold under the name Prozac®.

Fluoxetine is considered to be not as effective as Fluvoxamine, most notably with respect to Sigma-1 receptor agonistic effects. However, in areas where nonclinical studies of Fluvoxamine are not available I may refer to studies on Fluoxetine in its place. Remember that these drugs are similar and not the same, and the results of studies should be seen more as relative than quantitative. However, we may see that it is possible to broaden the group of drugs under examination even further.
Note: Know that these reviews are not intended to be complete reviews, and therefore many topics will be missed. The studies presented here are based predominately on the available literature that I was able to find and access, so please take that into account. In areas where additional information is required I shall add it there.
Nonclinical Studies
I was hoping to separate this section by nonclinical studies before and during COVID as I have done in prior posts. Unfortunately, the search for specific studies prior to COVID has been somewhat fruitless, partly because of paywalls and also because of exact examination of either Fluvoxamine/Fluoxetine within the literature. Therefore, I will categorize studies based on MOA instead. I may also refer to other therapeutic agents, meaning that this analysis will be somewhat broader than I would have initially intended.
Mast Cell Degranulation
This is one of the MOAs that I did not cover previously, so I will provide brief detail here before examining the literature.
If mast cells sound familiar, it’s because they play a vital role in allergies. Mast cells are a group of cells responsible for allergic reactions and many innate and adaptive immune responses (taken from Krystel-Whittemore et. al.):
Mast cells are involved in the regulation of variety of physiological functions, including vasodilation, angiogenesis, bacterial, and parasite elimination. In addition, mast cells regulate functions of many cell types, such as dendritic cells, macrophages, T cells, B cells, fibroblasts, eosinophils, endothelial cells, and epithelial cells. Since, mast cells generate and release multi-potent molecules, such as histamine, proteases, prostanoids, leukotrienes, heparin, and many cytokines, chemokines, and growth factors, they have the capacity to be involved in regulating the functions of many organs and tissues. One of the mostly studied functions of the mast cell is its role in vascular and bronchial homeostasis. Mast cells also play a significant role in the regulation of bone growth, remodeling, and mineral homeostasis.
“Degranulation” of mast cells refer to the release of pro-inflammatory biomarkers such as histamines and cytokines, and its this release that is likely to play a role in the damage seen in allergic reactions and viral infections after excessive activation of mast cells.
More specifically, mast cells exhibit a high level of ACEII receptors, and post-mortem biopsies of lung tissue have shown activated mast cell invasion of these biopsies. This would suggest that viral infection of mast cells may lead to excessive degranulation, eventually leading to extensive inflammation, lung damage, and possibly death.
However, this effect is not exclusive to lung tissue alone, as any region of mast cell accumulation may elicit cytotoxic and organ damage.
SSRIs such as Fluoxetine and Fluvoxamine have been known to reduce histamine release, and may play an inhibitory role in mast cell degranulation.
In a study by Chen et. al. researchers examined whether Fluoxetine would inhibit mast cell degranulation in the gastric tract of depressed (chronically stressed) mice models.
Researchers first checked for the expression of rat mast cell protease (rMCP-I), an enzyme who’s expression depends upon IgE antibodies released by mast cells and plays an important role in inflammation. Therefore, higher mast cell activity is related to high rMCP-I expression. rMCP-I expression was examined with immunofluorescence imaging.
Here, researchers found that depressed mice treated with Fluoxetine showed decreased expression of rMCP-I compared to untreated depressed mice, suggesting a protective effect of Fluoxetine.

The researchers then compared normal mast cells (granulated) against activated mast cells (degranulated) by examining tissue under an electronic microscope. The tissue was dissected into quadrants and stained for the presence of granules. Normal mast cells would show staining inside cells while degranulated cells should not show similar staining.
The researchers also saw decreased levels of activated mast cells in depressed mice treated with Fluoxetine, suggesting that mast cell activation was inhibited by treatment with Fluoxetine.

The results of this study suggest that SSRIs, in particular Fluoxetine, may inhibit mast cell degranulation in those under heavy stressors. Within the context of COVID, it would suggest that inhibition of degranulation may prevent excessive inflammation from severe viral infection.
Unfortunately, this study requires a few leaps in order to compare it to our situation with COVID. For one, Fluoxetine was used instead of Fluvoxamine. We can assume similar effects between the two, although the extent to which they are similar cannot be determined. Also, we need to assume that the results of this gastric examination may translate into other tissues such as lung tissue. It presupposes that the behaviors and activities of mast cells would remain similar within different tissues. However this doesn’t take into account the drug distribution of Fluoxetine/Fluvoxamine and thus the difference in therapeutic effects across different organs.
It’s also difficult to relate exogenous, physical stressors used on these mice models and compare them to the dynamics of viral infections (these mice were stressed with stressors such as cold baths, tail nipping, etc.). If mast cells, by virtue of their high expression of ACEII receptors, are likely targets of viruses, and we also know that SSRIs such as Fluvoxamine are able to target multiple points of viral entry and replication, then it seems more rational to argue that Fluvoxamine’s multifaceted nature is likely to be a more important role than inhibition of mast cells through enzymatic expression alone.
Therefore, I would take this study with a skeptical eye as these results may not be well generalized towards COVID.
*A Brief Aside*
In my search for nonclinical studies on Fluvoxamine, as outlined by multiple schematic diagrams, I was hoping to find specific studies in support of such MOAs proposed. Instead, it appears that several of these MOAs are more relegated to hypotheticals and extrapolated from more distant studies than I would feel comfortable to use, such as the one indicated above.
Now, I could just as well not include the above study, even though many literature reviews of Fluvoxamine and COVID have cited this study. However, I’ve decided to keep it to show that MOAs depend upon actual evidence-based studies in order to validate or rebut proposed hypotheses.
It is on me for not having looked deeply into the actual literature before examining the MOAs alone, but this points to an important aspect of science in that care must be taken to understand the limitations to which one can extrapolate and generalize a study without the proper evidence.
Endolysosomal Pathway
For this MOA, I have but one study to provide. However, there is a pretty broad literature review available on other lysosomotropic agents and their relationship to lung infection with SARS-COV2 for those who would like more information. For that, I point those people to this literature review from Blaess et. al.
I will delve deeper into another MOA that goes along with this pathway, but for now we will focus solely on lysosomes as possible traffickers.
We will focus solely on this study from Glebov, O. in which the sole researcher examined Fluvoxamine-mediated uptake of spike protein into lysosomes:
Here, I investigated the effect of an antidepressant drug fluvoxamine on membrane trafficking of the SARS-CoV-2 spike protein and its cell host receptor ACE2 in HEK293T cells. A sub-therapeutic concentration (80 nM) of fluvoxamine rapidly upregulated fluid-phase endocytosis, resulting in enhanced accumulation of the spike-ACE2 complex in enlarged early endosomes. Diversion of endosomal trafficking provides a simple cell biological mechanism consistent with the protective effect of antidepressants against COVID-19, highlighting their therapeutic and prophylactic potential.
The sole researcher used HEK293T cell lines and treated them with varying concentrations of Fluvoxamine to take into account the difference in concentration of Fluvoxamine between blood plasma and the concentration found within the brain. Cells were incubated for 1 hour, and uptake of a fluorescent dye was used as an indicator for endocytosis.
The increase in dye uptake was considered indicative of increased endocytosis.
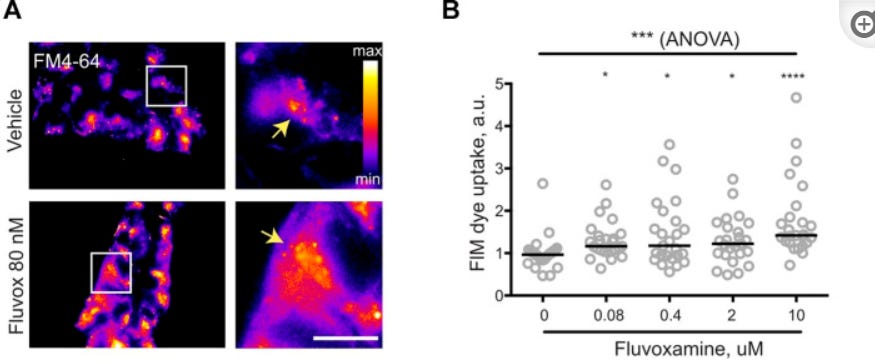
The researcher then wanted to examine if Fluvoxamine itself may upregulate endocytosis, which would suggest that endocytosis may increase with exposure to Fluvoxamine. Here, the researcher did see an increase in endocytosis in a dose-dependent manner, and that even a low dose of Fluvoxamine may increase endocytosis. However, the researcher did not provide an explanation as to why higher doses showed lower dye uptake (2 & 10 uM in particular), although this may be explained by a possible upper threshold of upregulation.

Lastly, in order to examine whether spike protein uptake increased with Fluvoxamine, recombinant SARS-COV2 spike proteins were transfected to cells. Internalization of Fluvoxamine was then measured with fluorescent dyes. Again, the internalization of membranous spike protein increased with the addition of low-dose Fluvoxamine. It’s also worth noting that ACEII expression did not statistically increase with the addition of Fluvoxamine, suggesting that increased uptake of spike protein is not related to increased ACEII expression.

Overall, this study would suggest that Fluvoxamine is likely to to increase endocytic uptake of SARS-COV2. The researcher notes this is likely to occur within the early endosome (Figure not included), as indicated by a staining assay specific to early endosomes. Another staining assay for late endosomes indicated no visible fluorescence. Taken together, this evidence would suggest that Fluvoxamine may elicit antiviral properties with the uptake and processing of viral particles by early endosomes and that processing/export of viral particles through late endosomes may not be targeted by Fluvoxamine.
Unfortunately, the researcher does not allude to the overall effect of spike protein uptake and endocytosis. As we have mentioned earlier, lysosomotropic agents may enter into endosomes, increase the pH, and halt the regular activities of endosomes and lysosomes likely through trapping of viral particles. This study merely alludes to the fact that Fluvoxamine may increase uptake of viral particles (actually, spike protein by the study design), but it does not provide any evidence as to the fate of such viral particles afterwards. Granted, the researcher states that the overall effects are not known, but that this is likely to be indicative of one of many possible therapeutic effects.
This study provides more questions than answers, as the exact mechanism of Fluvoxamine’s antiviral activity could not be discerned from this study. It is also important to state that spike protein internalization was examined with spike protein already located on test cell membranes and does not reflect the actual dynamics of SARS-COV2 attachment to ACEII receptors and that cascade of events. This study does provide an avenue for greater research, especially if the endosomal route of viral entry plays a more important role with Omicron, but as it stands this study alone is more difficult to assess within the overall context of infection.
Fortunately, we are able to flesh out another endolysosomal pathway to a greater extent.
Acid Sphingomyelinase/ Endolysosomal Route
This is another one of those pesky MOAs that I skipped over, as I thought it to be quite similar to the lysosomal route that we’ve covered already (my bad on my part!). As we will see this MOA is part of the overall endolysosomal pathway, but will focus on a more narrow aspect of the pathway.
This MOA is quite important, as it is likely the first point before viral infection occurs and is likely to play an early antiviral role.
Acid Sphingomyelinase (ASM) refers to a class of enzymes found on cell membranes, although they are also found within endolysosomes due to their budding and fusing interchangeable nature with cell membranes. ASMs are part of the overall ASM/ceramide system where activation of ASM leads to the cleavage of sphingomyeline proteins to release ceramides. If ceramides sound familiar, it’s because you have likely heard of them in many skincare products as they are added to products to supposedly aid in moisturization and provide “anti-aging” benefits.
Ceramides are hydrophobic/lipophilic proteins which means they prefer other fats and lipids. Supposedly, when ASMs are activated they lead to cleavage of sphingomyelin and the release of ceramide. Their lipophilic nature causes them to aggregate and create lipid-rich regions on cell membranes where other proteins may aggregate. Hypothetically, one of these possible membranous proteins are ACEII receptors, and one of the ideas here is that a large release of ceramides aggregate together bringing many ACEII receptors along as well. The high number of aggregate ACEII receptors may drastically increase signaling sensitivity, thus allowing for viruses to infect host cells.
Therefore, the inhibition of ASMs by drugs are likely to prevent ceramide production, ACEII aggregation, and therefore prevent viral entry. These classes of drugs are informally titled Functional Inhibitors of ASMs (FIASMAs), and they include various SSRIs such as Fluoxetine and Fluvoxamine.
Because ASMs are located both on cell membranes and within endolysosomes the effects here are likely multifold, and likely adds to the multifaceted nature of these SSRIs on viral infection. ASMs, as their name implies, operate under acidic conditions (pH~5.0), and are the main target enzyme of lysosomotrops as uptake of FIASMAs into lysosomes increase the pH and lead to the inactivation of ASM. Whether this prevents the eventual fusing of lysosomes to cell membranes is unclear, but this would lead to reduced production of ceramides and reduce the ability for SARS-COV2 to invade.
For additional information, I suggest this literature review from Kornhuber et. al.
The study we will look at is by Carpinteiro et. al. in which researchers tested for the inhibition of ASM by various agents and examined whether this led to SARS-COV2 uptake prevention. There’s quite a few therapeutics included here, most notably another FIASMA called Amitriptyline, along with several antibodies, so this evaluation will not look at Fluoxetine alone. I will try to briefly summarize the other experiments conducted. I highly suggest those who are interested take a full look at this study, as the researchers did a thorough job of elucidating this possible viral entry pathway, including possible effective therapeutics.

The sequence of studies here should be noted, as they provide accumulating evidence in favor of FIASMAs as possible COVID therapeutics and help to elucidate the endosomal pathway for viral infection.
The first few experiments conducted by the researchers suggested that FIASMAs, more specifically Amitriptyline, can inhibit viral infection by pseudoviruses containing SARS-COV2 spike protein (Figures 1 & 2, not included) and that both ASM activation and ceramide release are important to SARS-COV2 infection. Here, researchers found that ASM downregulation led to reduced pseudovirus spike protein infection, indicating that ASM activation is important for viral infection (Figure 3, not included):
To confirm the role of acid sphingomyelinase in infection with SARS-CoV-2 independent of pharmacological inhibition, we used shRNA-mediated suppression of the expression of acid sphingomyelinase in Caco-2 cells. We confirmed the downregulation of acid sphingomyelinase by measuring the activity of the enzyme in lysates of uninfected cells (Figure 3A). The results showed that genetic downregulation of acid sphingomyelinase prevented infection with pp-VSV-SARS-CoV-2 spike (Figure 3A). Control shRNA constructs had no effect on cellular infection with pp-VSV-SARS-CoV-2 spike. We further tested whether neutral sphingomyelinase may also be involved in cellular infection with SARS-CoV-2. To this end, we transfected Caco-2 cells with shRNA targeting neutral sphingomyelinase 2 and control shRNA. Transfection reduced neutral sphingomyelinase activity by approximately 60% but had no effect on cellular infection with pp-VSV-SARS-CoV-2 spike (Figure 3A).
In the last of the summaries, the researchers wanted to see if SARS-COV2’s spike protein itself may lead to activation of the ASM/Ceramide pathway. Researchers used 3 different pseudoviruses in this part of the study, and found that only pseudoviruses that expressed spike proteins were able to activate the ASM/Ceramide pathway.
In contrast, treating Vero cells with pp-VSV lacking SARS-CoV-2 spike or with pp-VSV-G particles did not result in the activation of acid sphingomyelinase or in a release of ceramide (Figures 3B and 4A), a finding indicating that the activation of acid sphingomyelinase and the release of ceramide are specifically induced by the spike protein. Pretreatment of the cells with 5, 10, 20, or 25 μM amitriptyline prevented the activation of acid sphingomyelinase and the release of ceramide upon infection with pp-VSV-SARS-CoV-2 spike for 30 min (Figures 3B and 4A). Controls showed that amitriptyline reduced both the constitutive and the viral-induced activity of acid sphingomyelinase (Figure 3B)…
To confirm the formation of ceramide and to determine whether ceramide is released in the plasma membrane after infection, we stained Vero cells prior to and after infection with pp-VSV-SARS-CoV-2 spike with Cy3-coupled anti-ceramide immunoglobulin M (IgM) antibodies and analyzed the cells by flow cytometry. These results revealed the formation of ceramide within the outer leaflet of the plasma membrane upon infection (Figure 4B).
Taken altogether, this study suggests that SARS-COV2’s spike protein is important for activation of ASM and the release of ceramides. This is an extremely important finding; it may suggest another possible cytotoxic effect of spike proteins. More importantly, because these studies did not use actual SARS-COV2 viruses and instead used pseudoviruses that expressed spike proteins, we may extrapolate these results to suggest that the spike protein alone may be solely responsible for ASM activation and ceramide release rather than the entire virion, something that should raise a few concerns as to spike protein focused products…
For the next assays of the study I will include some of the figures.
Next, researchers examined whether other FIASMAs would work in a similar manner as Amitriptyline. Vero cells were incubated with various FIASMAs, including Fluoxetine (Flu), and then challenged with pseudovirus with SARS-COV2 spike protein. The results of these assays showed that many FIASMAs are comparable in effect to one another (Figure 5B), which suggests that selectivity of ASM may not be too specific and that many FIASMAs are likely to be comparable to one another in effectiveness. Researchers also incubated Vero cells with ceramide to simulate ceramide-rich cell membranes and challenged them with pseudovirus-SARS-COV2 spike. Here, infection by pseudovirus appears to have been restored, adding validity to the importance of ceramide-rich membranes to SARS-COV2 infection (Figure 5C).

The final 2 Figures/Experiments of these studies are extremely important; they indicate a possible direct mechanism of action likely to occur in actually human infections.
Here, researchers isolated nasal epithelial cells from volunteers. However, one set of cells were pretreated with Amitryptiline (for 1 hour) after being isolated from volunteers (ex vivo) while another set of cells was isolated after a low, single dose of Amitryptiline (0.5 mg/kg) was administered to volunteers, essentially providing an in vivo analysis of ceramide inhibition. The in vivo nasal epithelials were isolated 1.5 hours and 24 hours after the single dose of Amitryptiline. After isolation and pretreatment, both groups of cells were challenged with pseudovirus expressing SARS-COV2 spike.
Remarkably, in both instances Amitryptiline pretreatment led to reduced ASM activation, and in the case of the in vivo cell line infection by pseudovirus was hindered up to 24 hours after the single dose.


There’s a few things to go over with this study.
For one, this study fully fleshes out the possible pathway for the ASM/Ceramide system, how viral infection from SARS-COV2 is likely to occur, and provides evidence that FIASMAs inhibit viral infection. What’s important here is that not only did various FIASMAs inhibit viral infection, but they did so at very low doses.
In summary, our findings indicate that SARS-CoV-2 activates the acid sphingomyelinase/ceramide pathway and uses this pathway for infection. Pharmacological or genetic inhibition of acid sphingomyelinase activity prevents infection with authentic SARS-CoV-2 virus or pp-VSV-SARS-CoV-2 spike particles in cell culture models and in freshly isolated human nasal epithelial cells from volunteers treated with amitriptyline and infected ex vivo.
Whether or not there is any validity to criticisms against Ivermectin or Hydroxychloroquine, many critiques have targeted their supposed low, ineffective doses, leading these critics to argue that much higher doses may result in toxicity.
The doses of the various FIASMAs deployed in this study were actually lower than typical antidepressant doses (an equivalent of 75 mg for a 150 lb adult). Considering that dosing for antidepressants can reach up to 200 mg/day, these result would suggest an effective dose that may not result in a high risk of adverse reactions. Strangely enough, because FIASMAs target lysosomes through an increase in pH they are known (although rare) to prolonged QT intervals in a similar manner to that of Hydroxychloroquine. However, it appears that in the rare instances that QT intervals may be prolonged this usually occurs at doses of SSRIs above 100 mg/day. FIASMA effectiveness under this dose would mean that prolonged QT intervals may not be a big concern.
Our studies demonstrate that even low dosages of amitriptyline provide long-lasting and very efficient protection against infection. Our findings also indicate that other drugs, such as imipramine, desipramine, fluoxetine, sertraline, escitalopram, and maprotiline, with concentrations similar to that of amitriptyline22 prevent infection with pp-VSV-SARS-CoV-2 spike.
Unfortunately, one flaw to this study is evaluating the role that spike protein dynamics play in ACEII binding and cellular modulation. The researchers did not indicate which SARS-COV2 spike variant they used. By now we should be well aware that Omicron’s spike protein is very different than prior variants, and therefore we should be hesitant when studies don’t discern the type of spike protein being deployed as it would likely have an effect on the results. Why Omicron depends upon the endolysosomal pathway to a greater extent is unclear, but it’s known that it is not as dependent upon the serine protease. This would likely suggest that cleavage of S1 and S2 spike subunits plays an important role in viral membrane fusion to host cell membranes and loss of cleavage function may cause Omicron to depend upon the endolysosomal route.
This study also looked predominately at Amitryptiline and not Fluvoxamine or Fluoxetine, but the other results suggest a generalized MOA of FIASMAs, and in fact indicates that several may be comparable in effectiveness.
Lastly, this study does not fully discern the exact time point of ASM inhibition. Does this occur within lysosomes as FIASMAs accumulate and increase the pH, rendering these ASMs ineffective and incapable of fusing to cell membranes, or is it that FIASMAs can target ASMs already located on cell membranes? Both certainly could be possible, and it’s likely that the synergistic effect is what prevents infection.
Overall, it appears that many antidepressants and SSRIs are likely to be extremely beneficial in preventing SARS-COV2 infection from a nonclinical perspective. They should also be taken into consideration as a prophylactic due to their relatively safe profile and proven prophylactic effects, as indicated in this study.
Here’s also something extremely important to point out within the context of COVID; elevated ceramide levels have been associated with diseases such as obesity, hypertension, and other forms of cardiac disease, all of which are some of the greatest comorbidity factors that contribute to severe COVID and death. So not only does this study provide a possible infection pathway, it also adds a possible causative role that comorbidities may play in increased viral infection and more severe illness due to chronically elevated ceramide levels.
Aside: Is it Better to Generalize?
I chose to look at Fluvoxamine itself because of the air surrounding it. It’s also one of the only SSRIs that have been used in clinical studies. However, we can clearly see that many antidepressants elicit similar functions to Fluvoxamine, and many could even be considered FIASMAs. A big part of this study has indicated that, although Amitryptiline appears to be highly effective so too do many other antidepressants. Therefore, these studies may not be indicative of one drug alone but adds veracity to the broad class of drugs alone.
So it may not necessarily be important to focus on one drug alone, but to analyze the class as a whole and their activities with respect to specific cellular activities.
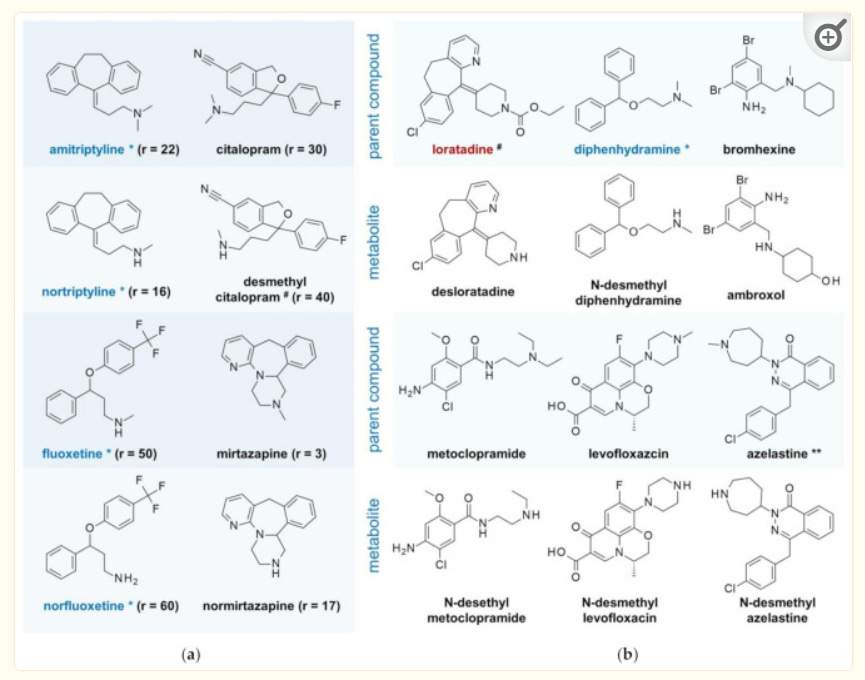
What’s interesting is that the activity of FIASMAs are not highly specific to one molecular structure. In fact, it appears that only a few factors are important for an antidepressant to act as an FIASMA.
Here’s an excerpt from Kornhuber et. al.:
Functional inhibition of ASM requires only a few structural conditions; the molecules need to contain a lipophilic organic ring that integrates into the inner lysosomal membrane, a short spacer and a charged tertiary amine group that displaces ASM from the inner lysosomal membrane, which results in the proteolysis of the enzyme in the lysosomal lumen [36, 37].
Another Aside: Look for Evidence, not Hypotheticals
Going through this portion of Nonclinical studies have shown me a few things. Hypothetical frameworks provide a jumping off point for further research, but should not be taken as an indication that such cellular pathways are in play. Many literature reviews on Fluvoxamine have reiterated similar mechanisms of actions as one another. However, the research itself may not end up validating these hypotheses at the time of construction, and I have found that out personally while writing this section. It has been very difficult finding any evidence of Fluvoxamine’s role in platelet aggregation and their effects on thrombosis or SARS-COV2 infection. The same can be somewhat said about lysosomotropism, although lysosomotropism goes hand in hand with the ASM/Ceramide system.
It also may be important to not be so parochial in the search for studies and evidence. Here, I focused solely on any studies on Fluvoxamine and nearly came up empty handed under many circumstances. Instead, it may be more appropriate to analyze the MOAs and nonclinical effects of drugs on a class basis. We can see here that I have cited studies that have either used Fluoxetine or Amitriptyline and have tried to remain reserved on doing such a thing. Yet both drugs can be categorized as FIASMAs and both also elicit lysosomotropic effects. The results of these studies may not be comparable, but they may at least suggest a possible correlative effect that may be validated with further research. There’s a reason why many review literatures I have found have reviewed SSRIs or antidepressants as a whole rather than individually.
Because this post has once again run afoul in size, I will keep the last MOA of Sigma-1 Receptors for Part III.