
Boosting Our Way into Insanity (Rant)
When at first it doesn’t succeed, try and try again-much to our dismay.

Recently the FDA has indicated that boosters for J&J’s Adenovirus-based vaccine as well as Moderna’s mRNA vaccine would be approved for the elderly. This comes nearly a month after the selective booster approval for Pfizer/BioNTech’s mRNA vaccine. Along with this new information, the FDA stated that the booster can be interchangeable with any of the other vaccines, and not the same ones that were given originally to patients.
Unfortunately, this once again does not seem like an evidence-based approach to medicine, because clearly there has to be evidence there to indicate that boosters are necessary.
Validated under False Pretenses?
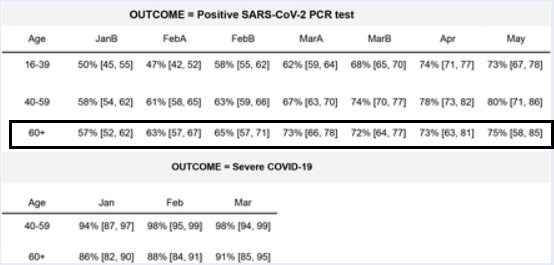
Most of this booster validation comes from a retroactive Israeli study by Bar-on et. al. 2021, in which infection rates in Israel citizens 60 years old and up were compared between booster and nonbooster groups. According to the researchers greater reduction in infection was found in those that were boosted vs nonboosted. Sounds great on paper, and may indicate that boosters should be administered in the elderly. However, let’s look at some limitations with this study.
Previous Evidence
The authors point to previous evidence that a booster shot lead to a 10-fold increase in neutralizing antibodies. However, the link leads to Pfizer’s Second Quarter 2021 Earnings Teleconference, and the only mention of this “10-fold increase” was from one of the slides.

Although this may seem nitpicky, I’d be hard pressed to assume the veracity of a slide for quarterly earnings conference without the actual study. This would have to be taken with a large grain of salt, especially considering this is being used in a quarterly earnings conference (you’d want to fluff up your numbers to investors).
Not a Randomized Control Trial/ Double-Blinded Study
The study used a retroactive approach and went through Israel’s Ministry of Health database to collect information between the time period of July 30th – August 31st, 2021. RCT/DB studies have become the bread and butter of the science community when it comes to COVID, but here this study does not follow that approach, opening itself up to plenty of confounding influences.
Our analysis was based on medical data from the Ministry of Health database that were extracted on September 2, 2021. At that time, a total of 1,186,779 Israeli residents who were 60 years of age or older had been fully vaccinated (i.e., received two doses of BNT162b2) at least 5 months earlier (i.e., before March 1, 2021) and were alive on July 30, 2021. We excluded from the analysis participants who had missing data regarding sex; were abroad in August 2021; had received a diagnosis of PCR-positive Covid-19 before July 30, 2021; had received a booster dose before July 30, 2021; or had been fully vaccinated before January 16, 2021. A total of 1,137,804 participants met the inclusion criteria for the analysis (Figure 1).
The researchers relied on reported PCR tests (something I have been critical about) to compare infection rates between there 2 groups. Unfortunately, the data set is scant in data, and doesn’t take into account why someone may get tested.
There are many reasons why someone would get tested which the database does not take into account:
Rise in Delta may have changed testing procedures (increased testing rates)
increases in vaccination may mean many people who are mildly symptomatic may not be likely to get tested, especially if they utilize a vaccine passport
It also would not take into account behavioral differences between the 2 groups that may change how they interact with other people (does a booster make people more likely to visit social areas?)
Severely ill and immunocompromised citizens may be encouraged to get boosters, but these people may also be less likely to routinely go out in public and conflating numbers.
Take a look at how the researchers discuss this bias:
Although our analysis attempted to address possible biases in the source data, such as the effects of confounders and behavioral changes after vaccination, some sources of bias may not have been measured or corrected adequately. These biases include differences between the booster recipients and those who did not receive the booster with respect to care-seeking behaviors and cautiousness, along with differences in coexisting illnesses that are not recorded in the national database. Some of these possible biases are transient and fade with time after the booster vaccination, as schematically shown in Figure S1. This suggests that the real effectiveness of vaccination can be estimated by comparing infection rates before receipt of the booster dose and after a suitable time period (e.g., 12 days) following vaccination. Although independent research is required to fully understand this behavioral model, several indications suggest that our 12-day cutoff is reasonable. First, persons tend to undergo fewer PCR tests on the day of vaccination and during the subsequent few days, which is a potential source for detection bias. Consistent with such behavioral change is the pattern shown in Figure 2, which indicates a large reduction in infection rate on the first day after vaccination, a decrease that is attenuated during the subsequent days before starting to increase as the booster dose becomes effective.
The “transient” nature of these biases are based on behavioral changes; people who have gotten boosters may want to avoid public areas for the first 2 weeks. But there’s a lot more to the biases than just behavioral changes, and to argue that they all are transient and brush off all possible biases that may affect this study is honestly concerning. Remember this is a retrospective study, not a randomized-control trial.
But, more importantly, the database doesn’t seem to include comorbidities, something that seems really important to include. You would think something so important would be mentioned, especially since people who are immunocompromised or severely ill would most likely be told to get a booster.
The data included vaccination dates (first, second, and third doses); information regarding PCR testing (sampling dates and results); the date of any Covid-19 hospitalization (if relevant); demographic variables, such as age, sex, and demographic group (general Jewish, Arab, or ultra-Orthodox Jewish population), as determined by the participant’s statistical area of residence (similar to a census block)8; and clinical status (mild or severe disease). Severe disease was defined as a resting respiratory rate of more than 30 breaths per minute, an oxygen saturation of less than 94% while breathing ambient air, or a ratio of partial pressure of arterial oxygen to fraction of inspired oxygen of less than 300.9
There’s plenty of ways the data can be influenced, and those need to be taken into account.
Where did the 50% come from?
I’ll skip over the statistical evidence, and I’ll go with the notion that there does seem to be a decrease in infection rate in the booster group. However, what’s extremely concerning is this paragraph in the Discussion portion:
In our study, we found that a booster dose of the BNT162b2 vaccine reduced the rates of both confirmed infection and severe Covid-19 illness in a large Israeli population of participants who were 60 years of age or older. Our findings can be understood through the following example. Suppose, first, that the combined effect of waning immunity and the increased prevalence of the delta variant decreases the efficacy of a vaccine that had been administered 6 months earlier to approximately 50% relative to thesusceptibility in an unvaccinated person, as recent reports have suggested.2,16,17 Then suppose that, as suggested by our results, the booster dose reduces the rate of infection for such vaccine recipients by a factor of 10. This would mean that the susceptibility of a person who receives a booster dose would decrease to approximately 5% (i.e., 50% divided by 10) relative to that in an unvaccinated person and would bring the vaccine efficacy among booster recipients to approximately 95%, a value similar to the original vaccine efficacy reported against the alpha variant.9,18
The authors suggest that the efficacy of the vaccine has been reduced by half relative to the unvaccinated group and cites 3 papers; one paper examined the waning effectiveness of the Pfizer vaccine while the other 2 compared Pfizer’s to Moderna’s. The only possible evidence of the 50% decrease between vaccinated and unvaccinated individuals comes from the Goldberg et. al. 2021 study.
But none of the studies were powered to indicate whether or not the decrease in effectiveness was due to both/either the waning immunity or the increased prevalence of Delta. The other 2 studies linked compared the effectiveness of Moderna to Pfizer against both Alpha and Delta. Unless I am examining these studies wrong (FYI I’m not good with the statistics), there’s no true evidence to indicate that 50% value.
The authors do state it’s their “supposition”, but it seems like a bold claim to assume the 50% value and to extrapolate that to the 95% efficacy previously indicated, especially since it matches up with the original clinical trial efficacy data (this sends up a lot of red flags).
The original efficacy data was deserving of scrutiny and yet this number is once again being paraded to indicate how effective these boosters are without any clear evidence of the sort. Maybe this is once again the dangers of the media frivolously reporting such numbers, but researchers should be careful to extrapolate their conclusions, especially if it can be abused by the media.
Now, know that I may have absolutely botched the interpretation of this study (and I welcome corrections), but if we are to go along with implementing policies we should hope that these policies are rooted in science, and as of now it seems like there really is no evidence of this occurring.
No Two Vaccines are Alike
We have known since the vaccine roll outs began that there have been different levels of effectiveness between these vaccines. Moderna, according to their clinical trials, had around 94% efficacy, and seems more effective than Pfizer against Delta (the studies cited by the Israeli one indicated as much), followed by Pfizer and then J&J. It should be obvious, then, that these differences in efficacy should be taken into account.
Although both Moderna and Pfizer are mRNA based, Moderna contains a higher concentration of mRNA (100 mcg/shot vs Pfizer’s 30 mcg/shot), and may indicate why a recipient’s antibody levels do not wane to the same extent that Pfizer’s does as indicated by the Puranik et. al. 2021 study.
J&J is also a DNA based vaccine that uses an adenovirus vector. The idea with a vector-based vaccine would be to have it stimulate an immune response over longer periods, and thus provide longer immunity, but the use of DNA means that the DNA would need to enter the nucleus of a cell, be transcribed, and the proceeding mRNA would then be translated into the proper spike protein. This process may end up reducing the effectiveness if the DNA has difficulty reaching the nucleus.
Edit: Following my post on OAS, note that there needs to be huge concerns about antibodies being produces against the adenovirus vector. If this were to occur, there absolutely should be no reason that people should receive a 2nd dose of the adenobased vaccines. This honestly may explain one of the reasons for the mix and match, but this seriously needs to be looked into.
All of these factors indicate that all of these vaccines, although they target COVID, do have differences, and these differences should be taken into account when assessing for risk of adverse events or compromised immune system.
The idea that these vaccines, which have varied efficacies and adverse events, are being allowed to be mixed and matched, undermines the nuances of each vaccine and how these may affect recipients.
Not only does this approach seem nonsensical, it also goes against any sensible approach to medicine and science. Imagine if you were allowed to choose the type of statin or blood pressure medication you wanted to take and were allowed to mix and match without the oversight of a doctor.
As of now there is absolutely no evidence indicating what will occur when different vaccines are mixed. Even if the safety profile remains unaffected, the concern here is the vaccine effectiveness, and we need to find evidence that mixing vaccines provides good protection, otherwise this seems like an absolutely ridiculous position to take.
The Consequences of Aging
The main cohort that the boosters are intended to target are the elderly, and these studies suggest that waning effects are more severe in this group. However, this is expected, and is in fact a consequence of aging. Many elderly undergo immunosenescence; their immune systems are not as robust and their naïve memory cell repertoire is depleted.
Take this excerpt from Crooke et. al. 2019:
Aging is associated with the decline of various biological systems and the development of numerous co-morbidities, such as diabetes mellitus, cancer, and various autoimmune and neurological disorders [1]. The immune system suffers equally from the effects of biological aging, exhibiting a progressive decline in function—referred to as immunosenescence—that collectively results in diminished humoral and cellular immune responses [2–4]. (Figure (Figure1)1) Mechanistic analyses of immunosenescence are complicated by the integrated nature of the immune system, as it is difficult to discern if immune cell dysregulation is a result of inherent cellular changes or a reactionary mechanism to changes elsewhere in the body. Regardless of origin, functional differences in the aging immune system are well-documented [5, 6], and several studies have attributed negative clinical outcomes in populations of older adults (i.e., 65 years and older) to immunosenescence. The severity of viral and bacterial infections (e.g., influenza, respiratory syncytial virus [RSV], herpes zoster, pneumococcal disease) is notably increased among older adults compared to younger individuals, and more acute and long-term sequelae often develop as a result [7–10]. Vaccination serves as the main strategy for preventing such infections, yet primary vaccine responses are often lower in older adults, frequently failing to induce long-term protective immunity and placing these individuals at further risk for subsequent disease [11–14]. These findings have been predominantly linked to the function and perceived failure of the adaptive immune response in older adults.

This is, and always should have been, a huge concern when vaccinating the elderly. Take for example seasonal flu vaccines. There are specially formulated vaccines that usually contain either a higher concentration of the antigen or would be developed to contain adjuvants (compounds that stimulate immune response).
Once again, the type of vaccine matters, and the immune status of those in higher age brackets absolutely need to be taken into consideration.
So why is this not being discussed? They way I see it the elderly are almost being used as experimental guinea pigs to validate this unfounded idea to provide boosters, and even worse to approve of mixing vaccines.
Don’t be surprised if we eventually see news reports indicating that mixing and matching is both safe and effective by utilizing data from the elderly.
Don’t Commit to Insanity
Before we commit ourselves to insanity, how about we try to rationalize the need for boosters by examining what we can (and possibly should) do before we think about boosters.
If antibody levels are being used to validate the waning effectiveness of vaccines, why not test for antibody titers before administering boosters?
Even adding onto that, memory cells serve a more important role than antibodies alone, so why not test for memory cells?
Conduct more studies indicating that boosters provide long-lasting immunity – the Israeli study only measures about a month out from the study, so we don’t even know for how long boosters will last.
Again, this needs to be reiterated, we need to have clinical studies that suggest that mixing vaccines are safe before we start treating the elderly as our experimental group.
And I’ll end this rant with this:
In 2018 then President Trump signed the “Right to Try” bill, which allowed people the ability to try experimental therapeutics for life-threatening illnesses. Many people began to write on online websites such as Reddit about family members and loved ones who passed without access to possible treatments, and discussed the possible benefits of this bill.
Of course, many detractors came out arguing that this bill would essentially allow Big Pharma the ability to subvert traditional clinical procedures, essentially experimenting on naive people without the need to go through regulatory bodies such as the NIH and FDA.
Over the course of the pandemic we have seen this exact scenario play out, but instead of utilizing anger and mounting criticisms against the federal government and Big Pharma, we instead see a populace fully complacent about the subversion of typical procedures due to a pandemic.
The elderly were never included in the original vaccine clinical trials (the age cutoff was around 65), and they certainly were not included in any booster trials (remember the Israeli study is retroactive, meaning they gave them without actual evidence about its efficacies), and here we see the NIH, FDA, and Big Pharma subverting those same procedures that people were warning about over 3 years ago.
Sure, the pandemic may mean we need to speed up the processes, but it doesn’t mean that full abandonment of the scientific process is warranted to achieve the results that those higher up intend to see.
The elderly are one of the most vulnerable groups, and we should be more than ashamed when we see our elders being taken advantage of and be used as test subjects.
It’s bad enough that we may also deal with the possibility that young children may be used as massive test subjects as well, now that there’s talk of giving the vaccine to children aged 5-11.
So maybe it’s not just the notion that repeating the same things over again and hoping to get different results as the idea of insanity; it may be that expecting results predicated on hardly evidence, at the sacrifice of science and the health of our fellow Americans, that would suffice as well.
Note: Like I said I am absolutely horrible with statistics-and honestly numbers, so if anyone sees any faults with the way I examined/interpreted the Bar-on et. al. study please let me know and I’ll make sure to make a correction!
Edit: Additional information was added to the adenovirus vaccine section.
Thank you for reading my newsletter. If you enjoy my articles please consider becoming a free subscriber in order to receive notifications.
And share with others who may find these newsletters interesting.
Also, please consider becoming a paid member. The research and work put into these articles takes many hours and being a paid subscriber allows me to continue to do this full time.
In-Text Citations
Bar-on et. al. 2021. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8461568/
Pfizer’s Second Quarter 2021 Earnings Teleconference Presentation. Taken from https://s21.q4cdn.com/317678438/files/doc_financials/2021/q2/Q2-2021-Earnings-Charts-FINAL.pdf
Goldberg et. al. 2021. Waning immunity of the BNT162b2 vaccine: A nationwide study from Israel. Taken from https://www.medrxiv.org/content/10.1101/2021.08.24.21262423v1
Tang et. al. 2021. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the Delta (B.1.617.2) variant in Qatar. Taken from https://www.medrxiv.org/content/10.1101/2021.08.11.21261885v1
Puranik et. al. 2021. Comparison of two highly-effective mRNA vaccines for COVID-19 during periods of Alpha and Delta variant prevalence. Taken from https://www.medrxiv.org/content/10.1101/2021.08.06.21261707v3
Crooke et. al. 2019. Immunosenescence and human vaccine immune responses
Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6743147/
Additional Sources
Pfizer’s Second Quarter 2021 Earnings Teleconference Transcript (I suggest people look into this. I think there’s probably some juicy stuff-I skimmed it a bit). Taken from https://s21.q4cdn.com/317678438/files/doc_financials/2021/q2/PFE-USQ_Transcript_2021-07-28.pdf
Compans et. al. 2009. Immunosenescence and Influenza Vaccine Efficacy. Taken from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7121450/
Regarding #2 above: https://www.medrxiv.org/content/10.1101/2021.08.19.21262111v1
This paper seems to imply that there is no b-cell memory as a result of "vaccination" and therefore may explain why the perceived need for furthers jabs of the same "formula". The question is why are the titers for synthetic immunity so much higher than those with natural acquired immunity and why does synthetic spike antibodies decay at a 40%/month rate and diminish to non-detectable after only 6 months? Whereas NI antibodies/titers wane at only 5%/month are are still detectable much longer. The question is would they "vaccines" have worked if the dose was set to be similar to that of NI titers in recently recovered individuals? I suspect the answer would be no and they probably knew this well before they jabbed anyone outside of their trials.
See: There's An Off Ramp - But It Has A Price https://market-ticker.org/akcs-www?post=243442
"But, as Israel has now shown with conclusive data antibody titers from vaccination wane at 40% a month while those from infection decrease at a much slower rate and in fact broaden in terms of recognition to the virus over time.
Why?
The broadening is indicative of B-cell recall, which is utterly crucial for lasting immunity. Antibodies do not circulate forever in the blood and other tissues; they eventually degrade and are replaced -- if your body's immune system has been trained. Your B-cells are largely responsible for this, along with T-cells and a whole cadre of other components of the immune system. This is why monoclonal antibody infusions protect you right now, when infected, but do not provide lasting immunity on their own. The infection itself does, but not the infusion. If you give the infusion to a non-infected person you wasted it; they have protection for a short period of time but it goes away.
The evidence from these now-published decay rates is that B-cell training does not happen with any of these vaccines. This is important and, it would appear, both Pfizer and Moderna (along with J&J) either knew or should have known this. In fact they all may have deliberately rigged their studies to be submitted for EUAs knowing the failure to produce a durable immune response was not going to be discovered due to time considerations. This cannot be proved without a bevvy of subpoenas of course but it is a reasonable and rational explanation for setting the dose and produced titer where they all did.
You can bet the vaccine makers will all do everything in their power to evade disclosure of what they knew and when in this regard because if in fact they knew that B-cell induction did not happen and deliberately set dosing to produce a result intended to game the EUA process that is quite-arguably intentional misconduct which is the bar that must be cleared to void their legal immunity for all of the adverse events PLUS all those who got infected as the defectively-produced immunity waned.
Consider a 40% per month decay rate for these injections and a natural infection that produces a titer of "100" (units don't matter for this purpose, nor does the actual number -- just the ratio.)
If the jab produces an original titer of 1,000 (10x as much) you get the following titer level on a monthly basis for the jabs:
0: 1,000
1: 600
2: 360
3: 216
4: 129
5: 77
6: 46
At six months you're probably below the protection threshold. Note that it takes 12 months, starting from 100 with a 5% monthly decay for natural infection, to reach the same titer.
So why does the titer decay so much slower if you get infected? Simple: It doesn't actually go away; natural infection trains your B-cells which is a durable response and thus capable of immediately restoring protection if you get challenged with the virus again, which you will. This is why the Cleveland Clinic, following their employees who got infected, found zero re-infections over more than a year's time among more than 1,000 infected and recovered individuals. It is also why a recent study found that natural infection and recovery was 13x as protective as the jabs."
Seems Pfizer hasn't actually released any of their data on the boosters - just the infamous press releases claiming wonderful efficacy! No data for anyone to even ponder or scrutinize. Also, with the mixed jabs (and the coercion to gets everyone vaccinated) it seems they are truly vaccinating their way out of control groups which will make their data even more confounding.