


Beware of those Proposing "Snake Venom"
An analysis of “Watch the Water” and the grave faults of the COVID dissenting community.

Note: Citations will be added later due to email limit.
A few days ago another Substack(-er?) Brian Mowry created a post about a Rumble video in which Dr. Ardis is interviewed by Stew Peters. Brian provided his own opinion and analysis of the video and I provided my own pontification based on his analysis. Of course, that approach is both wrong and one I should try to avoid, so eventually I decided to watch the video (which can be found here).
Now, I have heard of Dr. Ardis before when I was researching for videos on Rumble (either a removed Dr. Malone or Dr. Bret Weinstein YouTube video), and so I had some reservations beforehand that made me skeptical of Dr. Ardis’ claims. But nonetheless I decided to watch this new video for myself.
And I’m glad I did, because I would not have been able to understand the actual problems with the video had I not watched it for myself.
So here I’ll provide my own opinions and draw from science to critique the opinions made by Dr. Ardis, and also explain my concerns about the growing level of conspiracy and unscientific assumptions that are arising among COVID dissenters.
Before we begin…
The video covers quite a few topics and before diving into the actual meat of it I find it fit to actually provide a brief over of some of the topics- most notably Remdesivir and Monoclonal Antibodies. I have written about these two before in my Anthology Series but I will provide some more information here. As you go through the information see if you may be able to piece together some issues with said Rumble video if you have watched it already.
Remdesivir
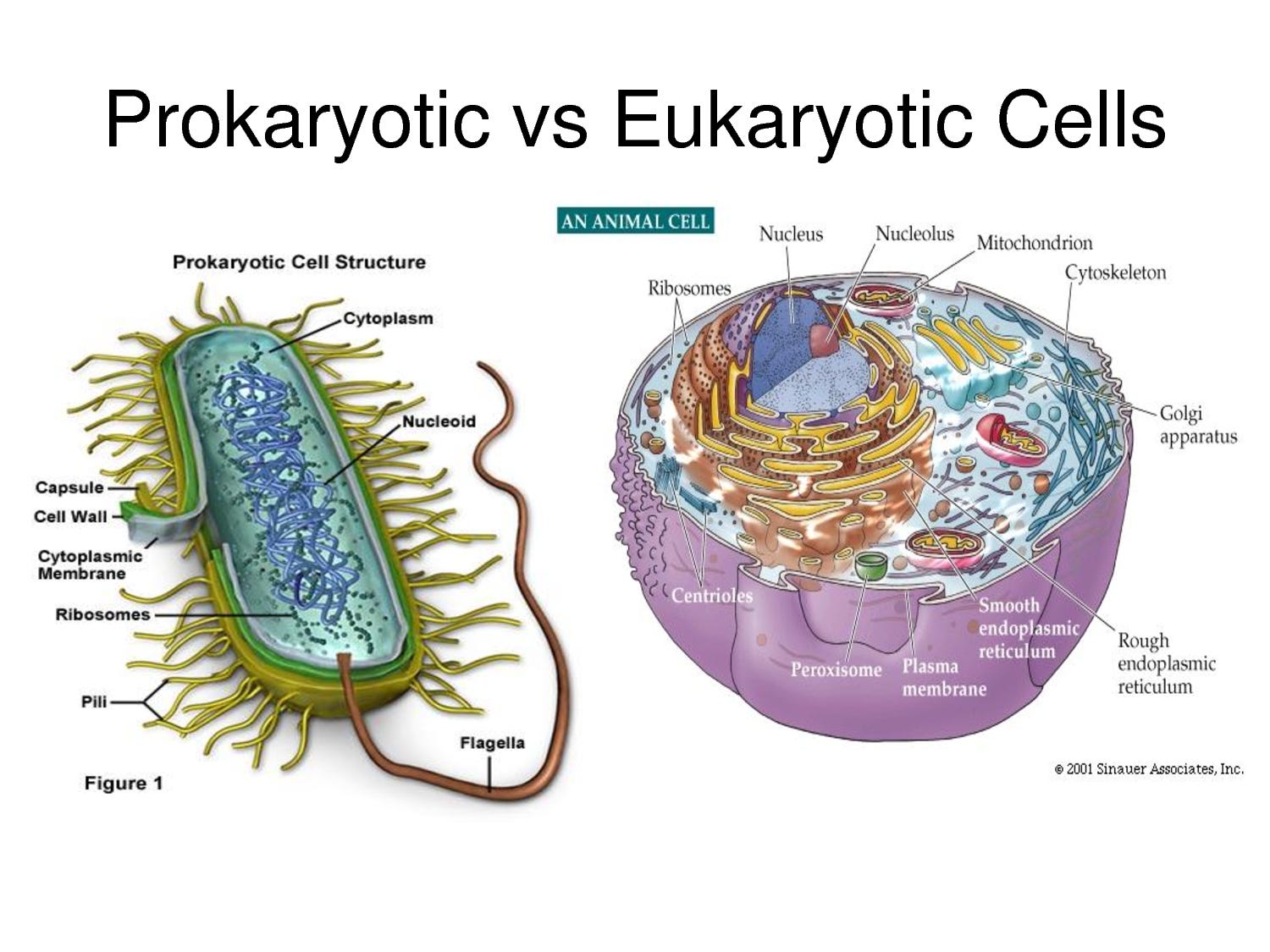
When developing a drug candidate researchers focus on reducing the toxicity while increasing the therapeutic effects. This is mainly done by observing differences in structure between the pathogen and the host. For example, bacteria are prokaryotes while human cells are eukaryotes. Animal eukaryotic cells are comprised of what’s called a cellular membrane which contain fatty acids and other structures. Prokaryotic cells, however, have another outer coating to their cells called a peptidoglycan/proteoglycan cell wall. Because our own cells are not comprised of these walls, we can target these structures and kill off the pathogenic bacteria while keeping our own cells relatively intact. This is where antibiotics come in, which target these bacteria walls selectively, making these prokaryotic cells porous and thus killing off these bacteria while keeping our cells relatively unscathed.
Viruses are a lot more difficult to target because they do not act on their own. They require entryway into our own cells and the utilization of our own cells’ machinery to copy itself. This conundrum therefore requires a different approach; instead of targeting a virus’ structure it may be more appropriate to target a key factor in the virus’ processes- in this case replication. Because viruses must replicate their genome in an alarming rate relative to our own cells, it may be possible to target the actual process of viral replication with selectivity towards viral replications over our own cells replications. Therefore, if a drug was able to look similar to the building blocks of a virus’ genome, it may be mistakenly picked up and thus halting the replication process. Remdesivir is one such drug.
Remdesivir comes from a class of drugs called nucleoside analogues which are intended to mimic the structure of our own nucleosides. Nucleosides (more specifically the triphosphate nucleotides) serve as the building block of our genome as well as those of bacteria, viruses, and all other organisms. By inserting this “pseudonucleotide” into the virus’ genome we may halt the virus’ replication process. For Remdesivir, its structure looks similar to that of Adenosine with a minor modification to the sugar ring through the addition of a cyano (-CN) group.

However, this similarity in structure between nucleoside analogues and endogenous nucleosides/nucleotides means that these drugs may be target for degradation by enzymes such as nucleases. There’s also an issue of drug distribution within the body and the analogues reaching their destination (remember ADME from pharmacology). Therefore, nucleoside analogues are administered as a prodrug, which is a form of the drug before it becomes bioactive. Usually these analogues have an addition of what’s called a protection group which both protects the drug from degradation as well as making it more easy to distribute within the body and enter into necessary cells.
Remdesivir has what’s called a McGuigan Protide as its protecting group (seen above). Unfortunately, this group causes a few problems- it actually reduces the solubility of Remdesivir so much that its bioavailability is greatly reduced. It also requires special disassembly by specific enzymes, mostly found within the liver in order to become active. Taken altogether, Remdesivir’s design caused a fatal flaw- it cannot be administered orally.
The workaround created was to administer Remdesivir with a carrier agent- essentially something that acts as an emulsifier and draws Remdesivir into solution so that it can be administered. This carrier agent is known as sulfobutylether-β-cyclodextrin, or SBECD for short. For more on this structure and its relationship to Remdesivir’s toxicity please take a look at my paid-member’s Remdesivir post.

But in general this means that Remdesivir must be administered intravenously rather than orally because the carrier agent requires a liquid solution to carry Remdesivir. Again, all of this is important to keep in mind as it explains why Remdesivir is administered in the way that it is.
Also, for more on Remdesivir refer to my Anthology Series on this matter.
Monoclonal Antibodies
I’m quite shocked at how foreign of a concept Monoclonal Antibodies (MAbs for short) are to people. It feels as if this is one drug that people should actually be drawing parallels to a commonly found factor of immunity- antibodies.
Our immune system’s ability to target various antigens of pathogens requires it to recognize the antigen. However, our immune system has no way of knowing what to expect until the antigen presents itself. Early on in our development our naïve B cells undergo differentiation and mutation to create a diverse number of B cells each with their own distinct antibody. These B cells are all made with the concept that they will become useful in the future.
When an antigen is presented to B cells within our lymph nodes it may come into contact with a B cell that recognizes said antigen. By recognizing this antigen the B cell essentially directs itself to a life of self-propagation, such that it must make more of itself (clones) and the antibody that can target the antigen. This process is called clonal selection theory and it filters out the best, most specific B cells and corresponding antibodies to deal with an infection. In the grand scheme of immunity, the collection of B cells that target a pathogen would be considered polyclonal, as in multiple distinct B cells will produce clones of themselves. However, when examining one B cell/antibody in particular, this process is called monoclonal for one distinct clone of B cells.
It is this selection process that Monoclonal Antibodies as a therapeutic derives its name- researchers select for B cell lines that produce the best antibody against a specific pathogen and thus utilizes this clonal process to produce even more of that same antibody.
This is how many of the monoclonal antibodies that target SARS-COV2 were developed. Convalescent plasma from previously infected patients were collected, their B cells isolated, and the best antibody for targeting the spike protein was harvested for therapeutic use. Altogether, the utilization of Monoclonal Antibodies is derived from the process that we use to create our own antibodies, which highlights the fact that these processes are one and the same. It also raises questions as to why Monoclonal Antibodies are considered to be some sort of mystified, strange process that bears no resemblance to our own antibody production. But regardless, this concept is important to understand.
To the Main Event
Now that actually brings us to the meat of the matter, which is the actual video and interview. At this point you may have noticed some holes in Dr. Ardis’ claims based solely on the brief information I provided above. But nonetheless, we will dive in even further and dissect many of the claims presented.
When tackling this dissection I was unsure whether it would be proper to highlight certain aspects of the interview or to breakdown every aspect of the video. However, after watching the video for a second time I am leaning more towards the former for the same reason as to why I watched this video in the first place- I think everyone should watch it. Not because I find it to be full of factual information, but because it is so full of misinformation that I find it pertinent for others to watch and provide their own sound judgement and not rely solely on the accounts of either Brian or me.
The Ebola Trial
Dr. Ardis’ claim to fame comes from his stark criticism of Remdesivir (he does call himself the Remdesivir guy after all), rooted mostly from a December 2019 study published in the New England Journal of Medicine (NEJM). He uses this study as a validation that Remdesivir is not only ineffective, but also deadly. In fact, so deadly that the patients being administered Remdesivir were abruptly removed from Remdesivir and put on other treatments.
What Dr. Ardis has apparently neglected is that Ebola is a deadly virus with no real known effective therapeutic. Late stages of the disease leads to organ failure, so even on such a preliminary analysis of claim we can see that the evidence is confounded by the deadliness of Ebola itself. The case fatality rate of Ebola can range from 25% up to 90%, so is it any wonder why the death rate was so high? The researchers of this study even noted the grim prognosis of those who were included in their study:
A longer duration of symptoms before treatment was associated with significantly worse outcomes. Of note, 19% of patients who arrived at the treatment center within 1 day after the reported onset of symptoms died, as compared with 47% of patients who arrived after they had had symptoms for 5 days (Table S4). The odds of death increased by 11% (95% CI, 5 to 16) for each day after the onset of symptoms that the patient did not present to the treatment center (Table 3).
By the end of this 28 day study nearly half (43.1%) of all patients succumbed to Ebola. Therefore, I would argue that this causal relationship is moot for this study. It’s made even more moot by the fact that parallels cannot be drawn between this study and SARS-COV2, a completely different virus that presents with different symptoms. A big miss I would argue by Dr. Ardis.
But the issues don’t end there. One claim that Dr. Ardis has made was that Monoclonal Antibodies are snake antivenom. Well, a good-faith argument may take into consideration that Monoclonals are not just used against antivenom, but such a consideration would actually require a great deal of speculation on the part of his viewers, and such a shift in burden to conduct good-faith interpretations should not be needed- remember, it is his claim that both COVID and Remdesivir are snake venoms, and thus Monoclonals, which are treatments, must be used against them.
All this to say that Dr. Ardis never, in fact mentions, that the other drugs used in the Ebola treatment were actually Monoclonals. Actually, one of the Monoclonals used, ZMAPP, is considered a standard of care for Ebola:

So if we are to follow Dr. Ardis’ line of thinking are we to believe that Ebola is snake venom that we are providing antivenom for? This is made even more curious as Dr. Ardis has referenced this study excessively in interviews, but obfuscates the fact that these are Monoclonals and instead refers to them as “experimental drugs”. You may have noticed that he never made mention to these other therapeutics in his interview with Stew Peters, which raises questions as to “lies by omission”- is Dr. Ardis intentionally not detailing the other drugs used in this Ebola trial because it undermines his narrative, or is he just unaware that the other drugs were Monoclonals even though he has discussed this study for well over the past two years?
*Edit: Steve was changed to Stew. Apologies for the typo.
The Snake Venom Conundrum
There’s a lot to say about Dr. Ardis’ ability to come to a conclusion about snake venom. A random text from a not so subtle ambiguous figure, coming at the most opportune time, to inspire him to search up anti-venom. It sounds like something right out of a Hollywood film (or a highly produced documentary…).
Dr. Ardis’ argument about snake venom follows what’s considered the transitive property which states that things that are equal/the same can be made equal to other things:
A=B, B=C, therefore A=C.
Or in the concept of the transitive snake venom hypothesis:
Snake venom is treated with Monoclonals, Monoclonals are used to treat COVID, therefore COVID is snake venom and is treated with Monoclonals.
Or here’s a transcript taken from Lead Stories (the proper timestamp starts at 20:36, but that’s being nitpicky):
It’s a basic concept most people learn in their elementary level math courses, and it may work well for conceptualizing math. However, it does not hold the same water when it comes to matters that require nuance and context.
We should be wise to know that the Monoclonal argument is moot at this point- we produce monoclonal antibodies against many antigens, and thus Monoclonals are not designed for the sole treatment against snake venom. As to why Monoclonals have been removed against SARS-COV2, I wrote about that extensively in my Monoclonal Anthology Series.
And if you are wondering why snake venom treatment are antibodies, well Dr. Ardis states it himself- snake venom is a peptide, or a more fancy word for proteins. Antibodies tend to target exogenous proteins such as the spike protein and the nucleocapsid protein of SARS-COV2 as well as any other pathogens and their proteins. So Dr. Ardis’ line of thinking is faulty here for the simple fact that he is conflating the virtues of antibodies. Antibodies, by design, predominately target exogenous proteins, so it is this mechanism of action as to why Monoclonals target antivenom. And apparently, people who have been previously bitten by snakes produce antibodies against the venom.

Which brings us to the next point: Dr. Ardis proposes that people are being poisoned twofold- first through the drinking water through low dose venom and then again when hospitalized and injected, yet again, with more venom.
For those who have been around the neighborhood here for quite some time they should understand that toxins, just like drugs, enter into our bodies in a specific manner to their toxicity. Snakes bite and inject venom; spiders bite and inject venom; bees sting; and toxic plants are ingested.
So when presented with the idea that people are both ingesting and injecting venom, we may want to stop and think what this means pharmacologically, and we can look at the snake venom’s structure as a peptide to discredit this utility of its use.
Proteins are the sum of their amino acid parts, and thus their structure and influence are altered based upon the changes that occur in the amino acids. It’s why spike protein mutations alter the binding efficacy of antibodies. Therefore, changes in the behavior of amino acids would most certainly alter the behavior of the protein.
When proteins are ingested our stomach acids denature these proteins and cause them to become ineffective, likely due to the acidic environment causing massive protonation of amino acid residues and disrupting important ionic interactions and hydrogen bonding, which may cause misfolding of the proteins due to gastric pH. Proteases may also start the digestion process and help break down these proteins as well.
So what happens when snake venom, as a peptide, is swallowed? Well, under most circumstances it is likely to become denatured and stop working- it’s essentially made ineffective. Now, this certainly doesn’t mean that it’s safe to consume snake venom! We must also keep in mind that snake venom is comprised of various proteins and carbohydrates, and the chemical makeup will vary across different snakes. But what it does mean is that this is hardly an effective way of administering a peptide toxin. It’s why snake venom must be injected to work effectively.
Not only that, but this would also raise questions as to whether minor exposure to snake venom, not enough to produce cytotoxicity, may actually produce immunity against the venom- again, a bad way to try to harm millions of people!
This concept is even made more concerning because it appears that Dr. Ardis’ light bulb moment was an episode of Blacklist in which the main character was poisoned by snake venom. Yes, a TV show was part of the inspiration for coming up with this idea. I suppose that lawyers should start watching episodes of SVU to learn about court cases. TV producers also had the bright idea to believe that you could combat attempts at hacking by having two people typing on the same keyboard!
OK, that may be a bit much, but you get the point. Ardis’ argument must be substantiated with verifiable evidence. It requires proper analysis of the data to make such a point, and without such proper foundation the entire concept collapses under its own weight. Instead, Ardis’ claims rely on false pretenses, strung together with the use of a TV show in a haphazard attempt to warn of the impending doom that comes for millions of Americans. Its sense of urgency calls for you to listen and believe what he says, not to stop and spend a moment thinking about the actual veracity of the claims being made.
Additional Egregious/Moot Points
Just to summarize relatively quickly, I will point to a few other contentions points brought up in the video:
Ardis argues that Remdesivir, a lyophilized white powder, must also be the same as snake venom, which comes in a lyophilized white powder. Lyophilized means that it’s freeze dried- it is free of water, and that’s it! Similarities in color and structure is by no means a valid way of arguing that these are one and the same- should I be careful of my salt, sugar, and flour for fear they may be snake venom?
Along those lines Dr. Ardis also describes how Remdesivir is made in a solution of sodium chloride, just like snake venom. What’s another term for a sodium chloride solution? A saline solution, or salt water. Salt water is needed to help stabilize the structures of compounds in a solution (salt, just like acidity, affects the structure of proteins).
There is a point in the video where a person is shown to take an antigen test and have sink water flow over the assay. Now, if this was an actual lab setting and a PI, graduate student or manager saw someone doing this they would likely be scolded, mostly for the mere fact that you do not flood your assay! There’s a reason why these antigen tests come with a stopper! Doing so is likely to damage the assay by overwhelming the antibodies, at which point you may cause anything to bind to it and give it a false positive. It’s also important to note that the line in the antigen test is very faint. Most companies will argue that any faint line will be indicative of a positive COVID test. However, part of me wonders if the producers of this video looked at the wrong line- the C, or control line, and assumed that that bold red line was indicative of a positive test. Again, this is the control line, not the test line (T) that is used to diagnosis a COVID positive patient.
Dr. Ardis actually got one point correct, albeit for all the wrong reasons. There are concerns that Remdesivir is cardiotoxic, but that’s because of the mere fact that Remdesivir is a nucleoside analogue of Adenosine and thus looks similar enough to Adenosine to be recognized as such by Adenosine receptors. Adenosine receptors are abundant in the heart and affects bloodflow and contractility. Too much may cause arrythmias and prolonged QT intervals similar to that of Hydroxychloroquine. So it’s not a surprise that a drug that’s intended to mimic Adenosine may also cause adverse reactions similar to Adenosine- it is by virtue of the drug’s nuceloside mimicry that these possible cardiotoxic events may be occurring (taken from Nabati, M. & Parsaee, H.):
Remdesivir is a 1′-cyano-substituted adenosine nucleotide prodrug which inhibits viral RNA synthesis. This metabolite is an adenosine analog but with a significantly longer half-life than adenosine. Adenosine is a powerful vasodilator that can cause profound hypotension which is followed by the compensatory release of catecholamines. It can also shorten atrial action potential and refractoriness and lead to atrial fibrillation (AF). These effects may also occur in ventricular cells and predispose patients to ventricular fibrillation. Remdesivir can also induce significant cytotoxic effects in cardiomyocytes that is considerably worse than chloroquine cardiotoxic effects.
Presentation is Everything
There’s so much more to be said, but I may be belaboring the idea at this point.
However, what I find concerning is that for many dissenters of the COVID narrative there appears to be this immediate pivot to view dissenters as being truthful. You’ve heard such phrases as “I do the opposite of whatever the CDC and FDA says”, which is actually an irresponsible argument. It argues that, by virtue of not being those I oppose, I can therefore state I am for whatever the argument is that is being made. So many people appear to rightfully be critical of the mainstream narrative, which wrongly causes them to assume that those who also state the opposite will be telling you the truth and are deserving of your trust and attention.
And it is here where Dr. Ardis bolsters his argument through the use of urgency- millions of lives are on the line, I am being targeted, and this message must get out! Listen and believe folks!
I find it rather troubling the level to which many dissenters evoke religious language, and this is coming from someone who is rather secular. The evocation of religious allusions of the snake, the flimsy connections to corona, the idea that “virus” is derived from a French word for poison, are all used as a form of mental trickery, almost like those seen by televangelists. It lulls those into a state of anxiety, a state in which they are left vulnerable and unable to think for themselves, looking for answers and whoever it may come from.
And these prayers are answered, but by merchants of fear; people who wish to keep you in a state of panic but from the opposite of what the staunch COVID fear mongers are forcing. Instead of telling you that you will all die from COVID, these merchants will tell you there’s a grand scheme to depopulate the earth, a satanic cult hellbent on damning all of us to a massive grave. I find it so frustrating that those who have learned to be skeptical of others are so gullible to believe whatever they find online, and it especially feels more frustrating to see how easily the religious community can be captivated by the sudden evocation of religion as done throughout the documentary.
Isn’t there a section in the bible about being wary of false prophets? So why is it that people are so willing to cling to those who ascribe to religious viewpoints, those who are willing to tell you that your savior has arrived in the form of Dr. X. Escape from mainstream science and return to religion, as if to say they are two irreconcilable viewpoints.
Such displays of cognitive dissonance creates confusion and doesn’t allow one to think critically, and that’s what these merchants of both sides want; it’s what they all crave! And yet people are so willing to provide them the sustenance they so desire, but with such willingness and admiration that I may actually consider horrifying.
I have commented in Brian’s comment section, but I will reiterate it here.
Dr. Ardis’ strength is not derived from the factual basis of his arguments, but by the naivety and ignorance of his listeners and viewers. I don’t know anything about Stew Peters, but it is easy to tell that he is not well-equipped to rebut what Dr. Ardis is saying. That’s mainly because he is relying on Dr. Ardis to be factual in his assumptions. Stew is not properly armed to rebut the claims made by Dr. Ardis, and instead is relegated to a back-seat position where Dr. Ardis makes his claims and Stew may allow minor inputs every now and then.
There’s a reason why Joe Rogan is so beloved. It’s not because he interviews high-profile people, but that he is someone who makes an attempt to understand what his guests are saying. He is well-read, and it comes out in his interviews. When something smells like bullshit Joe Rogan is not afraid to state it as such because he has the ability to do so- he tries to arm himself well against these types of points.
Contrast Joe Rogan’s interview style against Stew Peters and see the stark difference.
That’s not to say that Stew Peters is a bad interviewer, but when you are not well-equipped to argue against a guest it is very easy for a guest to make any claims under the sun whether substantiated or not. The best discourse can be brought out by rebuttals because it puts people in a position to either bolster their argument or flounder unequivocally. It challenges those who make bold claims to fully understand the claims they are making. It’s rather disheartening to see, based on some of the Substacks and other posts around the internet, that there appears to be a milquetoast approach to criticizing Dr. Ardis’ stance by those of us whose viewpoints have dissented from the mainstream COVID narrative.
What to make of the interview
Overall, I find that almost none of Dr. Ardis’ claims hold up to scrutiny.
Those who are quite skeptical will likely disregard it and not watch it. Many who are in agreement with the COVID dissenting narrative may blindly trust the claims they are made without doing their own research.
Although I find most of the arguments made in this interview to be made under false pretenses, I still find value in people watching it. It’s important to not immediately disregard ridiculous claims, especially when we don’t know which ridiculous claims are out there to disagree with.
I originally would have dismissed this video based on just reading Brian’s account, but it’s by watching it for myself I was able to spot all of the holes in Dr. Ardis’ line of thinking.
As of right now the video has near 2.5 million views on Rumble and is likely to gain more. I encourage those who have not watched the video to do so and make their own opinions.
I also encourage people to add their own comments in the comments section, whether to add their own insights or if there are questions that you would like addressed.
Anyways, thanks for telling us about the video Brian. I hate it.
There were so many things I left out because I hit the limit, such as Remdesivir being administered late in the disease progression being a factor, how there was no actual indication as to "what" snake venom he is referring to- snake venom is actually comprised of many proteins, enzymes, carbohydrates, etc. that would all be factors to consider, how acetylcholine is actually found in many neuromuscular junctions and not just in the brain. If anyone finds anything else they had questions on please leave a comment!
If you haven't already seen it watch Amandha Vollmer's video rebutting this absurd snake-alicious sensationalism.
She also speaks to the problems in the "Covid truther" movement so it's worth the time as her talk addresses more than just Ardis' documentary and interview with Stew Peters.
It helps that she's pretty funny and straightforward.
https://t.me/amandhavollmer/3428
"Everything is Covid-19- remember they sold you a story. It's all bullshit."
This is what too many who are "in the know" including Malone, McCullough, Kennedy, Kirsch, etc. won't confront. It's all fraud- it's all lies- the whole thing.